Download as doc, pdf, or txt
You might also like
- DR Write UpDocument15 pagesDR Write Upjansestacio100% (3)
- Date/Time Focus Progress Notes: Charisse Dl. LimosDocument6 pagesDate/Time Focus Progress Notes: Charisse Dl. LimosCharisse Limos100% (6)
- 13 Areas of Assessment 3yrs OldDocument2 pages13 Areas of Assessment 3yrs OldLegendX100% (2)
- Delivery Room Write UpDocument15 pagesDelivery Room Write UpDavid Calalo0% (1)
- Actual and Potential NCPDocument5 pagesActual and Potential NCPkevinzky100% (4)
- Impaired Physical MobilityDocument1 pageImpaired Physical Mobilitykyaw100% (1)
- Marcos Fdar CesareanDocument1 pageMarcos Fdar CesareanArian May Marcos100% (1)
- 13 Areas of AssessmentDocument13 pages13 Areas of Assessmentrachael95% (21)
- Sample 13 Areas of AssessmentDocument4 pagesSample 13 Areas of AssessmentLes Tarnate FechaNo ratings yet
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentAnonymous 0fiCdLOooXNo ratings yet
- 13 Areas of AssessmentDocument2 pages13 Areas of AssessmentJefferson JaramillaNo ratings yet
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentCamilogsNo ratings yet
- Most Common Used FDAR For Ortho WardDocument19 pagesMost Common Used FDAR For Ortho WardMiguelito Galagar Gultiano75% (4)
- Nursing Care Plan (Post Op Exlap)Document2 pagesNursing Care Plan (Post Op Exlap)Kay D. Beredo100% (2)
- BAMBALAN - ABPS3A - SOCSCI103N - Activity 7, Module 3Document2 pagesBAMBALAN - ABPS3A - SOCSCI103N - Activity 7, Module 3DexterJohnN.Bambalan100% (2)
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentCheska YsabelleNo ratings yet
- 13 Areas CKDDocument10 pages13 Areas CKDGwen Stefanie Lagrimas ValloyasNo ratings yet
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentShehada Marcos BondadNo ratings yet
- 13 AREAS of ASSESSMENTDocument2 pages13 AREAS of ASSESSMENTCrystal Queen MarquezNo ratings yet
- 13 Areas of AssessmentDocument4 pages13 Areas of Assessmentnusdhockey0% (1)
- SAMPLE 13 Areas of AssessmentDocument6 pagesSAMPLE 13 Areas of AssessmentKatie Lacuata100% (1)
- 13 Areas of AssessmentDocument7 pages13 Areas of AssessmentJazmine GayleNo ratings yet
- 13 Areas of Assessment I. Psychosocial StatusDocument4 pages13 Areas of Assessment I. Psychosocial StatusDizah Faye OsboroNo ratings yet
- 13 Areas of Assessment BGHDocument2 pages13 Areas of Assessment BGHZamranosNo ratings yet
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentSoleil MaxwellNo ratings yet
- 13 Areas of Assessment 1. Psychosocial StatusDocument3 pages13 Areas of Assessment 1. Psychosocial StatusCheska Ysabelle100% (1)
- 13-Areas-of-Assessment-2017 2Document3 pages13-Areas-of-Assessment-2017 2Alyssa Moutrie Dulay ArabeNo ratings yet
- 13 Areas of AssessmentDocument2 pages13 Areas of Assessmentapi-3718174100% (3)
- 13 Areas of AssessmentDocument10 pages13 Areas of Assessmentobietobi50% (2)
- 13 Areas of Assessment (Tomas Claudio Memorial College)Document14 pages13 Areas of Assessment (Tomas Claudio Memorial College)jorden36067% (3)
- OR Write-up-NSDDocument6 pagesOR Write-up-NSDBernardNo ratings yet
- 13 Areas of AssessmentDocument2 pages13 Areas of Assessmentmarkraymundangelica50% (2)
- 13 Areas of Assessment FrejDocument3 pages13 Areas of Assessment FrejJoMa TuazonNo ratings yet
- FDAR Charting - Readiness For Enhanced ComfortDocument1 pageFDAR Charting - Readiness For Enhanced ComfortWyen Cabatbat100% (1)
- 13 Areas of Assessment (Elderly)Document3 pages13 Areas of Assessment (Elderly)Znarf100% (1)
- OR Write Up - Repeat LSCSDocument2 pagesOR Write Up - Repeat LSCSWyen CabatbatNo ratings yet
- Nursing Program FDAR Charting Focus Data Action ResponseDocument2 pagesNursing Program FDAR Charting Focus Data Action ResponseJear Romero100% (1)
- FDAR Charting NICUDocument1 pageFDAR Charting NICUYuvi LuardoNo ratings yet
- Fdar For UtiDocument2 pagesFdar For UtiCARL ANGEL JAOCHICONo ratings yet
- TasadayDocument2 pagesTasadayRodolfo CampoNo ratings yet
- 13 Areas of AssessmentDocument10 pages13 Areas of AssessmentNicole Anne TungolNo ratings yet
- Nurses Progress NotesDocument2 pagesNurses Progress Notesvan100% (1)
- University of The Cordilleras College of NursingDocument38 pagesUniversity of The Cordilleras College of NursingCheshire AnnecyNo ratings yet
- Activity in Eyes ConceptDocument2 pagesActivity in Eyes ConceptWiljohn de la CruzNo ratings yet
- Lorenzo's Oil Movie Reaction PaperDocument4 pagesLorenzo's Oil Movie Reaction Paperharley olzanskiNo ratings yet
- DR WriteUpDocument40 pagesDR WriteUpDyanne BautistaNo ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationAlyssa Moutrie Dulay Arabe100% (1)
- Aminoleban Drug StudyDocument1 pageAminoleban Drug StudyNajmah Saaban100% (1)
- Fdar Risk For InfectionDocument1 pageFdar Risk For InfectionMatelyn OargaNo ratings yet
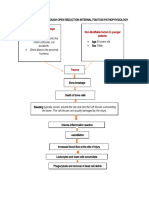
- Post Open Reduction Internal Fixation PathophysiologyDocument3 pagesPost Open Reduction Internal Fixation PathophysiologyRizalyn QuindipanNo ratings yet
- Body WeaknessDocument1 pageBody Weaknessnymphaaugustus100% (3)
- Comprehensive Assessment Is Not A Neutral ProcessDocument2 pagesComprehensive Assessment Is Not A Neutral ProcessGrape JuiceNo ratings yet
- Pathophysiology of NSDDocument2 pagesPathophysiology of NSDJNDNNSBM50610% (1)
- Thirteen Areas of Assessment I. PsychologicalDocument2 pagesThirteen Areas of Assessment I. PsychologicalShehada Marcos BondadNo ratings yet
- 13 Areas of AssessmentDocument5 pages13 Areas of AssessmentPau-pau BasiNo ratings yet
- MattDocument3 pagesMattMatthew CalaraNo ratings yet
- Marcos - Er - 13 AreasDocument2 pagesMarcos - Er - 13 AreasAssasination ClassroomNo ratings yet
- 13 Area of AssessmentDocument3 pages13 Area of AssessmentLea CortesNo ratings yet
- 13 Areas DutyDocument3 pages13 Areas DutyAndrei MarcosNo ratings yet
- 13 Areas of Assessment I. Psychological StatusDocument3 pages13 Areas of Assessment I. Psychological StatusjoharaqohNo ratings yet
- OXYTOCINDocument1 pageOXYTOCINBernardNo ratings yet
- Delivery DrugsDocument2 pagesDelivery DrugsBernardNo ratings yet
- OR Write-up-NSDDocument6 pagesOR Write-up-NSDBernardNo ratings yet
- Neurologic Disorders - NCM 102 LecturesDocument12 pagesNeurologic Disorders - NCM 102 LecturesBernard100% (4)
- NpiDocument9 pagesNpiBernardNo ratings yet
- Clinical Case PresentationDocument20 pagesClinical Case PresentationدرالجمانNo ratings yet
- Arthroscopic Surgery Patient InformationDocument3 pagesArthroscopic Surgery Patient InformationSylvia LoongNo ratings yet
- MSDS RO1 enDocument5 pagesMSDS RO1 enTito Prastyo RNo ratings yet
- EmergencydepartmentcrashDocument7 pagesEmergencydepartmentcrashnermeen diabNo ratings yet
- IFS Conversations Vol 6 PDFDocument32 pagesIFS Conversations Vol 6 PDFrakhi goyalNo ratings yet
- FFT Neuroma Morton PDFDocument6 pagesFFT Neuroma Morton PDFdasamoroNo ratings yet
- Assessing The Abdomen Basic Concept: Abdominal Assessment Is A Valuation of The Abdomen, Liver and BladderDocument6 pagesAssessing The Abdomen Basic Concept: Abdominal Assessment Is A Valuation of The Abdomen, Liver and BladderMay Chelle ErazoNo ratings yet
- Enteral Feeding: Indications, Complications, and Nursing CareDocument6 pagesEnteral Feeding: Indications, Complications, and Nursing CareSheena CabrilesNo ratings yet
- Necrotizing Ulcerative GingivitisDocument24 pagesNecrotizing Ulcerative Gingivitissvk_chatterjeeNo ratings yet
- Material Safety Data Sheet: ZenithDocument5 pagesMaterial Safety Data Sheet: ZenithFery FebryantoNo ratings yet
- Managing Heat StressDocument14 pagesManaging Heat StressMuhammad Aliff100% (1)
- Validated UHPLC-MS - MS Method For Quantification of Doxycycline in Abdominal Aortic Aneurysm PatientsDocument14 pagesValidated UHPLC-MS - MS Method For Quantification of Doxycycline in Abdominal Aortic Aneurysm PatientsAkhmad ArdiansyahNo ratings yet
- Health Ecstasy Group ProjectDocument11 pagesHealth Ecstasy Group ProjectIbtihalNo ratings yet
- August 3Document6 pagesAugust 3IceNo ratings yet
- Tongue Body ColorDocument4 pagesTongue Body ColorTanuku Net100% (1)
- Midi-And Mini-Primer Sets For Mtdna Control Region Sequence Analysis From Highly Degraded Forensic SamplesDocument1 pageMidi-And Mini-Primer Sets For Mtdna Control Region Sequence Analysis From Highly Degraded Forensic Samplesoday_ada76No ratings yet
- Emotional DisturbanceDocument62 pagesEmotional Disturbanceapi-340604729No ratings yet
- Advanced Critical Reading - Columbian ExchangeDocument4 pagesAdvanced Critical Reading - Columbian ExchangeVahid UzunlarNo ratings yet
- Biology Notes IGCSE Excretion NoteDocument9 pagesBiology Notes IGCSE Excretion NoteCorina HuNo ratings yet
- Sr. No Name Defination Eytmology DiagramDocument10 pagesSr. No Name Defination Eytmology DiagramMaheen AamirNo ratings yet
- YU PANG CHENG v. CADocument2 pagesYU PANG CHENG v. CAAlfonso DimlaNo ratings yet
- Careplan Week2Document2 pagesCareplan Week2api-302138606No ratings yet
- Biofluid Mechanics Chapter 6Document21 pagesBiofluid Mechanics Chapter 6AbcdNo ratings yet
- Complementary Therapies in Clinical PracticeDocument8 pagesComplementary Therapies in Clinical PracticeSeva Ikhsan PambudiNo ratings yet
- Case Spina BifidaDocument5 pagesCase Spina Bifidaroseavy100% (1)
- Senior Project PaperDocument18 pagesSenior Project Paperapi-403904589No ratings yet
- Food Safety Management SystemsDocument87 pagesFood Safety Management SystemsAshish SahuNo ratings yet
- Measles Case Reporting Form I.Case Identification/ Demographic DetailsDocument2 pagesMeasles Case Reporting Form I.Case Identification/ Demographic DetailsActivity ManagerNo ratings yet
- Ntruhs Thesis FormatDocument8 pagesNtruhs Thesis Formatheatherharveyanchorage100% (1)
- Times of India Chennai 04.04.2020 PDFDocument18 pagesTimes of India Chennai 04.04.2020 PDFnts1020No ratings yet