Download as pdf or txt
You might also like
- PFA Accomplisment ReportDocument4 pagesPFA Accomplisment ReportSHEILA MAE PERTIMOS100% (16)
- KATATAGAN ProgramDocument27 pagesKATATAGAN ProgramDarlene Corbilla CorderoNo ratings yet
- CHED NSTP Exemption FINALDocument12 pagesCHED NSTP Exemption FINALAvel RiveraNo ratings yet
- Computer System Validation Risk Assessment ToolDocument3 pagesComputer System Validation Risk Assessment Toolcpkakope100% (1)
- 4100XPB 4198 Grupo Mexico CananDocument758 pages4100XPB 4198 Grupo Mexico CananWalissonNo ratings yet
- Presence: A Primer on Trauma and Recovery for the Use of Trauma WorkersFrom EverandPresence: A Primer on Trauma and Recovery for the Use of Trauma WorkersNo ratings yet
- Fotocopias Ingles Tema Climate 1º EsoDocument6 pagesFotocopias Ingles Tema Climate 1º EsoMayOrdóñezNo ratings yet
- Introduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesDocument8 pagesIntroduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesManoj Kumar ChaurasiaNo ratings yet
- Katatagan. 2015 PDFDocument27 pagesKatatagan. 2015 PDFJuancho Reyes0% (1)
- EverlyFlynnPFAAfterDisasters PDFDocument13 pagesEverlyFlynnPFAAfterDisasters PDFKatalin GyüsziNo ratings yet
- Pfa Action Principles BTG-BRIDGE THE GAPDocument97 pagesPfa Action Principles BTG-BRIDGE THE GAPDung TuNo ratings yet
- Keefektifan Psychological First Aid (Pfa) Sebagai Pertolongan Pertama Pada Korban Bencana & TraumaDocument8 pagesKeefektifan Psychological First Aid (Pfa) Sebagai Pertolongan Pertama Pada Korban Bencana & TraumaAtiiiaaNo ratings yet
- Advances in Psychological and Social Support After DisastersDocument149 pagesAdvances in Psychological and Social Support After DisastersjprewittdiazNo ratings yet
- Psychological First Aid An Australian GuideDocument28 pagesPsychological First Aid An Australian GuideRajesh DhakeNo ratings yet
- Disaster Nursing SAS Session 13Document7 pagesDisaster Nursing SAS Session 13Niceniadas CaraballeNo ratings yet
- The Lived Experiences of Anxiety and Depression Support Philippines' (ADSP) Members Amid Public Stigma: A Phenomenological Hermeneutic StudyDocument10 pagesThe Lived Experiences of Anxiety and Depression Support Philippines' (ADSP) Members Amid Public Stigma: A Phenomenological Hermeneutic StudyJournal of Interdisciplinary PerspectivesNo ratings yet
- Advances in Disaster Mental Health and Psychological SupportDocument191 pagesAdvances in Disaster Mental Health and Psychological SupportKalmunai Mental Health Association100% (1)
- Handouts Psy121Document2 pagesHandouts Psy121Kael LuzonNo ratings yet
- Prof Fareed's Presentation1Document11 pagesProf Fareed's Presentation1Mahmood Ali Khan JafriNo ratings yet
- Psychodynamic Contributions To Early Intervention in PsychosisDocument10 pagesPsychodynamic Contributions To Early Intervention in PsychosiscaveolemuresNo ratings yet
- Mental Health and Psychosocial Support: Disaster Risk Management For HealthDocument2 pagesMental Health and Psychosocial Support: Disaster Risk Management For HealthyopanaNo ratings yet
- Disaster Nursing SAS Session 22Document8 pagesDisaster Nursing SAS Session 22ZiaNo ratings yet
- Essential MHPSS PresentationDocument24 pagesEssential MHPSS PresentationarifrahmaniNo ratings yet
- Psychological First Aid and Crisis InterventionDocument4 pagesPsychological First Aid and Crisis Interventionabigailgracesabu00No ratings yet
- Final Copy of Sustainability ProgramDocument17 pagesFinal Copy of Sustainability ProgramREADS RESEARCHNo ratings yet
- Group 2 - DMH - Draft - Written ReportDocument9 pagesGroup 2 - DMH - Draft - Written ReportIan MartinezNo ratings yet
- Crisis InterventionDocument15 pagesCrisis Interventionneethus10100% (2)
- Artigo Sueco CatastrofeDocument8 pagesArtigo Sueco CatastrofeEugénia Porto E NunoNo ratings yet
- Fpsyg 12 616426Document7 pagesFpsyg 12 616426Fabrizio ForlaniNo ratings yet
- Psychological First Aid and Nursing: ReviewDocument7 pagesPsychological First Aid and Nursing: ReviewMarcelo Fernandez GomezNo ratings yet
- Unit - 1 PfaDocument5 pagesUnit - 1 PfaSavithaNo ratings yet
- 617 - 23MHP10056Document11 pages617 - 23MHP10056liza.adventureNo ratings yet
- AnalisaDocument16 pagesAnalisaSeptyariNo ratings yet
- Introduction To PFADocument7 pagesIntroduction To PFACHRISTINE KYLE CIPRIANONo ratings yet
- Group 2 Disaster Nursing Summary ReportDocument11 pagesGroup 2 Disaster Nursing Summary ReportFrancis TolentinoNo ratings yet
- Critical Incident Stress DebriefingDocument29 pagesCritical Incident Stress Debriefinghubertbiangalen5No ratings yet
- Chapter 4Document57 pagesChapter 4Jaycel AquinoNo ratings yet
- Guidelines For Supporting Volunteers 2Document18 pagesGuidelines For Supporting Volunteers 2monica cmillosNo ratings yet
- 1-PFA-Rapid Proliferation - Disaster HealthDocument10 pages1-PFA-Rapid Proliferation - Disaster HealthBibire VasileNo ratings yet
- Effectiveness of The Therapeutic Intervention Program On The Socio-Emotional Development of Persons With Substance Use DisorderDocument8 pagesEffectiveness of The Therapeutic Intervention Program On The Socio-Emotional Development of Persons With Substance Use DisorderPsychology and Education: A Multidisciplinary JournalNo ratings yet
- CBPSS Training Day3Document26 pagesCBPSS Training Day3Lupeni Centru Comunitar de ZiNo ratings yet
- Red Cross Psychological First Aid Book PDFDocument23 pagesRed Cross Psychological First Aid Book PDFJankov1105100% (1)
- LAS3Document3 pagesLAS3CHEESESUS FRIESNo ratings yet
- PsychFirstAidSchools PDFDocument186 pagesPsychFirstAidSchools PDFAna ChicasNo ratings yet
- P - SMAIT Cahaya Bangsa - Salsabila Sofia & BQ - Alya Inanta Aurelia - Makalah - Nas2020Document4 pagesP - SMAIT Cahaya Bangsa - Salsabila Sofia & BQ - Alya Inanta Aurelia - Makalah - Nas2020Kusma watiNo ratings yet
- FacinguptotheChallengeofTyphoonYolanda June2014cDocument4 pagesFacinguptotheChallengeofTyphoonYolanda June2014cMarichelle AbreganaNo ratings yet
- Post-Disaster Mental Health Care in Japan: CorrespondenceDocument1 pagePost-Disaster Mental Health Care in Japan: CorrespondenceGahan DiwanNo ratings yet
- Applications of Psychological First Aid in Disaster and Emergency Situations: Its Relationship With Decision-MakingDocument14 pagesApplications of Psychological First Aid in Disaster and Emergency Situations: Its Relationship With Decision-MakingIrnanti WahyuriniNo ratings yet
- Unit 4Document15 pagesUnit 4Marbe HmtNo ratings yet
- Conclusion 2Document4 pagesConclusion 2LwhynnNo ratings yet
- Psychological First Aid For SchoolsDocument7 pagesPsychological First Aid For Schoolsmark anthony paraguisonNo ratings yet
- Disaster and Crises Mental Health CounsellingDocument12 pagesDisaster and Crises Mental Health CounsellingMuhammad HussainNo ratings yet
- Content ServerDocument8 pagesContent ServerSahara Iman AlontoNo ratings yet
- (Disaster Health 2013-Aug 02 Vol. 2 Iss. 1) Shultz, James M - Forbes, David - Psychological First Aid (2013) (10.4161 - Dish.26006) - Libgen - LiDocument11 pages(Disaster Health 2013-Aug 02 Vol. 2 Iss. 1) Shultz, James M - Forbes, David - Psychological First Aid (2013) (10.4161 - Dish.26006) - Libgen - LiMiguel OliveiraNo ratings yet
- Red Cross Psychological First Aid BookDocument28 pagesRed Cross Psychological First Aid BookQuique ParadaNo ratings yet
- Ladrido Ignacio1995Document50 pagesLadrido Ignacio1995Vj LoyaoNo ratings yet
- Emergency HandbookDocument13 pagesEmergency HandbookAshrafNo ratings yet
- 8731-Article Text-139123-1-10-20240112Document9 pages8731-Article Text-139123-1-10-20240112Matt Keanu CatapiaNo ratings yet
- Ni Hms 478574Document26 pagesNi Hms 478574adri90No ratings yet
- Blank 22Document2 pagesBlank 22LwhynnNo ratings yet
- Review of Psychological Trauma: Theory, Practice, Policy and ResearchDocument10 pagesReview of Psychological Trauma: Theory, Practice, Policy and ResearchMohammad TahanNo ratings yet
- 5 AiDocument8 pages5 AisifaNo ratings yet
- Early Psychosocial Intervention Following Traumatic EventsDocument4 pagesEarly Psychosocial Intervention Following Traumatic EventsAdrian CantemirNo ratings yet
- Annex 33 Mental Health and Psychosocial Support 23032020Document22 pagesAnnex 33 Mental Health and Psychosocial Support 23032020Mon LuffyNo ratings yet
- Multimodal Treatment of Acute Psychiatric Illness: A Guide for Hospital DiversionFrom EverandMultimodal Treatment of Acute Psychiatric Illness: A Guide for Hospital DiversionNo ratings yet
- Assessment in Industrial Setting: Current Trends and IssuesDocument41 pagesAssessment in Industrial Setting: Current Trends and IssuesAvel RiveraNo ratings yet
- HR Report As of May 29, 2020Document5 pagesHR Report As of May 29, 2020Avel RiveraNo ratings yet
- DDB Citizen Charter 2018 NewDocument10 pagesDDB Citizen Charter 2018 NewAvel RiveraNo ratings yet
- Summary of SAP Issuances As of April 7Document5 pagesSummary of SAP Issuances As of April 7Avel RiveraNo ratings yet
- 1-Intro To LeadershipDocument15 pages1-Intro To LeadershipAvel RiveraNo ratings yet
- Madac: Madac Committee On Youth Chair: Mydwb Vice Chair: SK Federation Members: DCS Pdea DilgDocument5 pagesMadac: Madac Committee On Youth Chair: Mydwb Vice Chair: SK Federation Members: DCS Pdea DilgAvel RiveraNo ratings yet
- Implementing The Integration Planning ProgramDocument39 pagesImplementing The Integration Planning ProgramAvel Rivera100% (1)
- Intervention Programs For Children in Conflict With The Law (Cicl) : Gearing Towards Sustainable DevelopmentDocument6 pagesIntervention Programs For Children in Conflict With The Law (Cicl) : Gearing Towards Sustainable DevelopmentAvel Rivera100% (1)
- Updates On SK Policies, Guidelines, and Other ProjectsDocument18 pagesUpdates On SK Policies, Guidelines, and Other ProjectsAvel RiveraNo ratings yet
- Telepsychology Guidelines PDFDocument2 pagesTelepsychology Guidelines PDFAvel RiveraNo ratings yet
- Andronic, Razvan-Lucian - VolunteeringDocument4 pagesAndronic, Razvan-Lucian - VolunteeringAvel RiveraNo ratings yet
- Supporting Diverse StudentsDocument12 pagesSupporting Diverse StudentsAvel RiveraNo ratings yet
- Muay Thai Beginners GuideDocument44 pagesMuay Thai Beginners GuideAmar Cooper67% (3)
- Module 7: Health Care Delivery SystemDocument9 pagesModule 7: Health Care Delivery SystemDanz KieNo ratings yet
- Heterocyclic Aromatic CompoundsDocument67 pagesHeterocyclic Aromatic CompoundsTuyenHHC100% (1)
- Starkville Dispatch Eedition 7-29-20Document16 pagesStarkville Dispatch Eedition 7-29-20The DispatchNo ratings yet
- Livebook ACBDocument420 pagesLivebook ACBShubhangi JagtapNo ratings yet
- Microsoft Word - ETERSET 2960-2 - MSDSDocument5 pagesMicrosoft Word - ETERSET 2960-2 - MSDSWinsonLimHuiWahNo ratings yet
- OlanzapineDocument1 pageOlanzapineKallie ChartrandNo ratings yet
- MPT ProjectDocument10 pagesMPT ProjectTina SanghaviNo ratings yet
- Drug Ana Surgery WardDocument11 pagesDrug Ana Surgery WardJames QuilingNo ratings yet
- Fiberdyne G.652.D Single Mode Fiber SpecificationsDocument1 pageFiberdyne G.652.D Single Mode Fiber SpecificationsjunedNo ratings yet
- Vegetarian Meals On College CampusesDocument14 pagesVegetarian Meals On College CampusesVegan FutureNo ratings yet
- On Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Document9 pagesOn Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Ansh MishraNo ratings yet
- Aisyah Fadiyah - SPEECH DRAFTDocument5 pagesAisyah Fadiyah - SPEECH DRAFTAisyah FawNo ratings yet
- ECA DatabaseDocument22 pagesECA DatabaseRidhwan JamaludinNo ratings yet
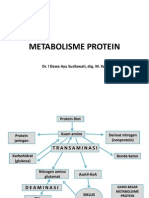
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- Long Quiz Earth Sci 11Document2 pagesLong Quiz Earth Sci 11Jesha mae MagnoNo ratings yet
- TN-4620190912122 Form21B Signed PDFDocument1 pageTN-4620190912122 Form21B Signed PDFDHEEN MEDICALSNo ratings yet
- Proforma A1: Residential/Domicile CertificateDocument6 pagesProforma A1: Residential/Domicile CertificateSamim ParvezNo ratings yet
- MASB7 Construction Contract7Document3 pagesMASB7 Construction Contract7hyraldNo ratings yet
- Pop That PimpleDocument24 pagesPop That Pimpleapi-666592607No ratings yet
- Bence Bays Resume July 2015Document2 pagesBence Bays Resume July 2015api-292242662No ratings yet
- Internet Article Showing Utah DCFS Ordered To Implement Changes in Lawsuit-1Document7 pagesInternet Article Showing Utah DCFS Ordered To Implement Changes in Lawsuit-1Roch LongueépéeNo ratings yet
- NeuroVascular (NV) Holding PointsDocument2 pagesNeuroVascular (NV) Holding PointsHatem Farouk100% (2)
- Problem Sets For Solutions AnalysisDocument2 pagesProblem Sets For Solutions AnalysisKamil Guillergan100% (1)
- It's A Safe World After All : TÜV FS EngineerDocument5 pagesIt's A Safe World After All : TÜV FS Engineerizadi1979No ratings yet
- Science G7 Q2 LP4Document13 pagesScience G7 Q2 LP4Lovely GuintoNo ratings yet