Download as pdf or txt
You might also like
- Primary Health Care: Mr. John Michael M. Pitoy, B.S.N., R.NDocument44 pagesPrimary Health Care: Mr. John Michael M. Pitoy, B.S.N., R.NJohn Michael Manlupig Pitoy100% (9)
- CANNABISDocument5 pagesCANNABISGeorgina AttipoeNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Medical Student Performance Evaluation ForDocument2 pagesMedical Student Performance Evaluation ForКостя РоманівNo ratings yet
- SI Indicator Formula Remarks No: Advers e Event: Any UntowardDocument11 pagesSI Indicator Formula Remarks No: Advers e Event: Any UntowardYogesh ChandraNo ratings yet
- Medication Safety: Reducing Anesthesia Medication Errors and Adverse Drug Events in Dentistry Part 1Document11 pagesMedication Safety: Reducing Anesthesia Medication Errors and Adverse Drug Events in Dentistry Part 1laur112233No ratings yet
- 258 QsDocument3 pages258 Qsujangketul62No ratings yet
- Potential Determinants of Drug-Drug Interaction Associated Dispensing in Community PharmaciesDocument8 pagesPotential Determinants of Drug-Drug Interaction Associated Dispensing in Community Pharmaciessaw thidaNo ratings yet
- A Bow Tie Analysis of Medical ErrorDocument4 pagesA Bow Tie Analysis of Medical ErrorJobNo ratings yet
- E151 Medicationerrors-QJMDocument10 pagesE151 Medicationerrors-QJMWens BambutNo ratings yet
- Medication Error PDFDocument61 pagesMedication Error PDFChelsea Ritz MendozaNo ratings yet
- E151 Medicationerrors-QJMDocument10 pagesE151 Medicationerrors-QJMRestu AriyusNo ratings yet
- Medication Errors: P AperDocument4 pagesMedication Errors: P Aperdesk ayu okaNo ratings yet
- 355 FullDocument5 pages355 FullRania SaadNo ratings yet
- Reducing Prescribing Error: Competence, Control, and CultureDocument5 pagesReducing Prescribing Error: Competence, Control, and CultureBev YuNo ratings yet
- Medication Error - Michael SandinDocument5 pagesMedication Error - Michael Sandinapi-379546477No ratings yet
- Medication Safety: Reducing Anesthesia Medication Errors and Adverse Drug Events in Dentistry Part 2Document12 pagesMedication Safety: Reducing Anesthesia Medication Errors and Adverse Drug Events in Dentistry Part 2laur112233No ratings yet
- Medication ErrorsDocument10 pagesMedication Errorsjuliana bNo ratings yet
- Medication Errors and Risk ReductionDocument3 pagesMedication Errors and Risk ReductionjellybeandumpppNo ratings yet
- Medication Errors: What They Are, How They Happen, and How To Avoid ThemDocument9 pagesMedication Errors: What They Are, How They Happen, and How To Avoid ThemMoisesNo ratings yet
- Medication Errors PaperDocument6 pagesMedication Errors Paperapi-542442476No ratings yet
- Medication Errors FinalDocument5 pagesMedication Errors Finalapi-379817190No ratings yet
- DRPs PDFDocument4 pagesDRPs PDFLeticiaNo ratings yet
- BJSTR MS Id 007162Document5 pagesBJSTR MS Id 007162Catrin_HutaurukNo ratings yet
- Defensive Medicine - A Bane To HealthcareDocument2 pagesDefensive Medicine - A Bane To Healthcareyashkh415No ratings yet
- Drug Errors: Consequences, Mechanisms, and Avoidance: Key PointsDocument7 pagesDrug Errors: Consequences, Mechanisms, and Avoidance: Key PointsRavikiran SuryanarayanamurthyNo ratings yet
- Running Head: Error in Medical Prescription 1Document5 pagesRunning Head: Error in Medical Prescription 1King Mugitah18No ratings yet
- CH 03Document18 pagesCH 03Emmanuel GaliciaNo ratings yet
- 42 PDFDocument5 pages42 PDFDaniela HernandezNo ratings yet
- Vein RomDocument4 pagesVein RomaksinuNo ratings yet
- Pharmacology ScrapbookDocument89 pagesPharmacology ScrapbookJesell France PlanaNo ratings yet
- Clarification of Terminology in Drug Safety.3Document20 pagesClarification of Terminology in Drug Safety.3JoaquinHernandezNo ratings yet
- Medication SafetyDocument54 pagesMedication SafetyJuwitaASih100% (2)
- Community Pharmacists' Opinions Towards Poor Prescription WritingDocument9 pagesCommunity Pharmacists' Opinions Towards Poor Prescription WritingJasmin Kae SistosoNo ratings yet
- Lecture 3Document66 pagesLecture 3gokulkrishnayadhavNo ratings yet
- Book For NurdrDocument34 pagesBook For NurdrFarmisa MannanNo ratings yet
- Case StudyDocument3 pagesCase StudygbasxuioqweNo ratings yet
- Medications Error PaperDocument7 pagesMedications Error Paperapi-676526945No ratings yet
- Drug-Related Problems: Definitions and Classification: January 2007Document4 pagesDrug-Related Problems: Definitions and Classification: January 2007salsaNo ratings yet
- Social Pharmacy: Medication ErrorsDocument62 pagesSocial Pharmacy: Medication ErrorsEmmanuel KingsNo ratings yet
- PharmacoviilanceDocument93 pagesPharmacoviilancekirti.unadkat70.nuNo ratings yet
- Med ErrorsDocument6 pagesMed Errorsapi-641561231No ratings yet
- MODULE 2 - Nursing Process in PharmacologyDocument5 pagesMODULE 2 - Nursing Process in PharmacologyDonna MarieNo ratings yet
- NURS-FPX4020 - MuaClaude - Assessment 1-1Document6 pagesNURS-FPX4020 - MuaClaude - Assessment 1-1marvinNo ratings yet
- Medication Error 2017Document51 pagesMedication Error 2017Christina100% (1)
- Drug-Related Problems:: Definitions and ClassificationDocument3 pagesDrug-Related Problems:: Definitions and ClassificationArdiansyah FarizalNo ratings yet
- Drug-Related Problems:: Definitions and ClassificationDocument3 pagesDrug-Related Problems:: Definitions and ClassificationAliff Dhurani ZakiNo ratings yet
- Concepts and Principles of Pharmacology To Ensure Safe and Proper Use of DrugsDocument21 pagesConcepts and Principles of Pharmacology To Ensure Safe and Proper Use of DrugsBea Bianca CruzNo ratings yet
- FoodDocument3 pagesFoodNorman MabalotNo ratings yet
- Types and Causes of Medication Errors From A Nurse'S ViewpointDocument3 pagesTypes and Causes of Medication Errors From A Nurse'S ViewpointMaryjoy Gabriellee De La CruzNo ratings yet
- Edwards Sharon Axe Sue 10 Rs of Safe Multidisciplinary Drug Administration PDFDocument9 pagesEdwards Sharon Axe Sue 10 Rs of Safe Multidisciplinary Drug Administration PDFNimrod Bautista SolosaNo ratings yet
- Medication Safety: Mita Restinia, M.Farm, AptDocument57 pagesMedication Safety: Mita Restinia, M.Farm, Apt094DNORMINo ratings yet
- 1-Guidelines For Safe Medication Adminstration (Non Parentral Medication Adminstration)Document6 pages1-Guidelines For Safe Medication Adminstration (Non Parentral Medication Adminstration)onco learnNo ratings yet
- The Ten R's of Safe Multidisciplinary Drug Administration: Better PracticeDocument12 pagesThe Ten R's of Safe Multidisciplinary Drug Administration: Better PracticeDarlene Faith BeroñaNo ratings yet
- PC2014 02 Spring - LookalikeSoundalike PDFDocument6 pagesPC2014 02 Spring - LookalikeSoundalike PDFRanil AcademiaNo ratings yet
- PHV TerminologyDocument5 pagesPHV TerminologyKadir AmirNo ratings yet
- Med Errors PaperDocument7 pagesMed Errors Paperapi-733165948No ratings yet
- Prescriber - 2009 - Edwards - Withdrawing Antidepressants Guide To Patient ManagementDocument5 pagesPrescriber - 2009 - Edwards - Withdrawing Antidepressants Guide To Patient Managementjosipa.vulic108No ratings yet
- Case StudyDocument10 pagesCase StudyRezwan DihanNo ratings yet
- PN-Chapter 3-Medication AdministrationDocument36 pagesPN-Chapter 3-Medication AdministrationmysNo ratings yet
- Liang Et Al 2023 Understanding Medical Malpractice LawsuitsDocument5 pagesLiang Et Al 2023 Understanding Medical Malpractice LawsuitskrisnawatiNo ratings yet
- Medication Safe PracticeDocument5 pagesMedication Safe Practiceapi-288858560No ratings yet
- The Essential Guide to Prescription Drugs, Update on RemdesivirFrom EverandThe Essential Guide to Prescription Drugs, Update on RemdesivirNo ratings yet
- Aplikasi WISNDocument9 pagesAplikasi WISNErni Yessyca SimamoraNo ratings yet
- Antimicrobial Stewardship Program (Ri)Document50 pagesAntimicrobial Stewardship Program (Ri)Erni Yessyca SimamoraNo ratings yet
- Hubungan Kelengkapan Rekam Medis DGN Klaim Bpjs PDFDocument7 pagesHubungan Kelengkapan Rekam Medis DGN Klaim Bpjs PDFErni Yessyca SimamoraNo ratings yet
- RWJF Collaboration PDFDocument2 pagesRWJF Collaboration PDFErni Yessyca SimamoraNo ratings yet
- Laporan Indikator Kepatuhan Formularium 2020Document26 pagesLaporan Indikator Kepatuhan Formularium 2020Erni Yessyca SimamoraNo ratings yet
- Comparison of Ultrasound Elastography, Mammography, and Sonography in The Diagnosis of Solid Breast LesionsDocument9 pagesComparison of Ultrasound Elastography, Mammography, and Sonography in The Diagnosis of Solid Breast LesionsErni Yessyca SimamoraNo ratings yet
- Effects of Work Environment and Engagement On Nurses Organizational Commitment in Public Hospitals Lahore, PakistanDocument6 pagesEffects of Work Environment and Engagement On Nurses Organizational Commitment in Public Hospitals Lahore, PakistanErni Yessyca SimamoraNo ratings yet
- Review Visi Dan Misi - Arief Wahyu SDocument3 pagesReview Visi Dan Misi - Arief Wahyu SErni Yessyca SimamoraNo ratings yet
- HBP Moving-Ahead PDFDocument2 pagesHBP Moving-Ahead PDFErni Yessyca SimamoraNo ratings yet
- Visi Dan Misi Rsud MatramanDocument2 pagesVisi Dan Misi Rsud MatramanErni Yessyca SimamoraNo ratings yet
- ValidasiDocument2 pagesValidasiErni Yessyca SimamoraNo ratings yet
- Misi-Visi Rsup PersahabatanDocument2 pagesMisi-Visi Rsup PersahabatanErni Yessyca SimamoraNo ratings yet
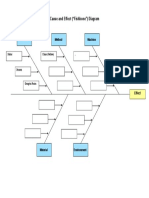
- Cause and Effect ("Fishbone") Diagram: Person Method MachineDocument1 pageCause and Effect ("Fishbone") Diagram: Person Method MachineErni Yessyca SimamoraNo ratings yet
- Meningitis TBDocument11 pagesMeningitis TBErni Yessyca SimamoraNo ratings yet
- 10 E-LibraryDocument18 pages10 E-LibraryErni Yessyca SimamoraNo ratings yet
- Meningitis TBDocument11 pagesMeningitis TBErni Yessyca SimamoraNo ratings yet
- Pneumonia AspirasiDocument7 pagesPneumonia AspirasiErni Yessyca SimamoraNo ratings yet
- Jurnal DHF IndonesiaDocument6 pagesJurnal DHF IndonesiaErni Yessyca SimamoraNo ratings yet
- Hepa-Merz: Hepatic EncephalopathyDocument40 pagesHepa-Merz: Hepatic EncephalopathyErni Yessyca Simamora83% (6)
- Lucy Mangan Updated Resume-3Document1 pageLucy Mangan Updated Resume-3api-296940298No ratings yet
- Universidad Iberoamericana: UnibeDocument3 pagesUniversidad Iberoamericana: UnibeMaria Paula Coss FernandezNo ratings yet
- Mental Health Case StudyDocument10 pagesMental Health Case Studyapi-401649778No ratings yet
- NP 1Document22 pagesNP 1June DumdumayaNo ratings yet
- Assignment-1 Why Do We Use Data Science in Healthcare?Document7 pagesAssignment-1 Why Do We Use Data Science in Healthcare?Eedula GaneshreddyNo ratings yet
- Client Feedback FormDocument4 pagesClient Feedback FormASHLEE DADOR FERRERNo ratings yet
- Professional Strength: Curriculum VitaeDocument2 pagesProfessional Strength: Curriculum Vitaeamr ahmedNo ratings yet
- Activity 1 in STSDocument3 pagesActivity 1 in STSzaidelfaye pagelaNo ratings yet
- Faktor Yang Berhubungan Dengan Kesiapan Persalinan Ibu Primigravida Di Wilayah Kerja Puskesmas Batulappa Kabupaten PinrangDocument5 pagesFaktor Yang Berhubungan Dengan Kesiapan Persalinan Ibu Primigravida Di Wilayah Kerja Puskesmas Batulappa Kabupaten PinrangPapy AleshaNo ratings yet
- Murtagh S Patient EducationDocument3 pagesMurtagh S Patient EducationMAYNo ratings yet
- DIASS SOC Work 1Document59 pagesDIASS SOC Work 1Anne Dela Cruz-BanaagNo ratings yet
- Are We Prepared To Detect Subtle and Nonconvulsive Status Epilepticus in Critically Ill Patients?Document7 pagesAre We Prepared To Detect Subtle and Nonconvulsive Status Epilepticus in Critically Ill Patients?succa07No ratings yet
- CHN Notes For Prelim ExamDocument26 pagesCHN Notes For Prelim ExamAldjen SetiasNo ratings yet
- Kerala Economic Review PDFDocument541 pagesKerala Economic Review PDFAyanasreeNo ratings yet
- DHIS Secondary Health Facility Monthly Report FormDocument4 pagesDHIS Secondary Health Facility Monthly Report FormBd Db50% (2)
- Madison Payne ResumeDocument2 pagesMadison Payne Resumeapi-598709763No ratings yet
- Resume 2Document3 pagesResume 2api-503171442No ratings yet
- NESTLE Kasambuhay Program - GRP1Document30 pagesNESTLE Kasambuhay Program - GRP1Zheanne ClaireNo ratings yet
- ReferencesDocument9 pagesReferencesJaz BenitoNo ratings yet
- Zimbabwe - Medical - CPIN - v2.0 - GOV - UKDocument39 pagesZimbabwe - Medical - CPIN - v2.0 - GOV - UKsammy redganjiNo ratings yet
- What Need Know About Wild OreganoDocument21 pagesWhat Need Know About Wild OreganoMatt PintoNo ratings yet
- Jones Etal 2019 Enhanced SupervisionDocument10 pagesJones Etal 2019 Enhanced SupervisionErick TavaresNo ratings yet
- медицинаDocument10 pagesмедицинаDariaNo ratings yet
- Controversiesin Dentoalveolarand Preprostheticsurgery: Deepak G. KrishnanDocument8 pagesControversiesin Dentoalveolarand Preprostheticsurgery: Deepak G. Krishnanmehak malhotraNo ratings yet
- Factors Affecting Students Preference of Nursing Education in SiDocument104 pagesFactors Affecting Students Preference of Nursing Education in SiLiza AingelicaNo ratings yet
- DS SalbutamolDocument1 pageDS SalbutamolLarr SumalpongNo ratings yet