
Functional Capacity Evaluation
Functional Capacity Evaluation
You might also like
- Wickes UnderlayDocument2 pagesWickes UnderlayfloodanddrainageNo ratings yet
- AOTA Exam PrepDocument2 pagesAOTA Exam PrepKenny ClayNo ratings yet
- Assessing Childhood Depression From Multiple Perspectives Via The CDI 2 ToolkitDocument53 pagesAssessing Childhood Depression From Multiple Perspectives Via The CDI 2 ToolkitSamar DakkakNo ratings yet
- OARS Adl IadlDocument5 pagesOARS Adl IadlSamuelNo ratings yet
- SLD GuidelinesDocument231 pagesSLD Guidelinesgryphon688No ratings yet
- RCI - Book On LD PDFDocument49 pagesRCI - Book On LD PDFNikhil Kumar DasNo ratings yet
- Helping You To Assess Cognition: A Practical Toolkit For CliniciansDocument45 pagesHelping You To Assess Cognition: A Practical Toolkit For Cliniciansdaniel serraniNo ratings yet
- Wolf Motor Function Test PDFDocument31 pagesWolf Motor Function Test PDFLydia MartínNo ratings yet
- Membership List: Russell 3000® IndexDocument33 pagesMembership List: Russell 3000® IndexJordi Oller SánchezNo ratings yet
- Functional Capacity Evaluation TemplateDocument11 pagesFunctional Capacity Evaluation TemplateMalik Muhammad Bilal Ali NissoanaNo ratings yet
- Modified Interest Checklist PDFDocument2 pagesModified Interest Checklist PDFMas EdoNo ratings yet
- Wee FimDocument9 pagesWee FimdeffyNo ratings yet
- Examiner's Manual & Technical Report: The Early Learning Accomplishment Profile EditionDocument48 pagesExaminer's Manual & Technical Report: The Early Learning Accomplishment Profile EditionRocioNo ratings yet
- Mini-Mental State Exam: 1 Orientation Questions ScoreDocument1 pageMini-Mental State Exam: 1 Orientation Questions ScoreAbegail GallardoNo ratings yet
- Functional AssesmentDocument22 pagesFunctional AssesmentHeri WibisonoNo ratings yet
- Global Developmental DelayDocument6 pagesGlobal Developmental DelayLiza Perlas Policarpio CarpioNo ratings yet
- Spinal Cord Assesment Form PTDocument8 pagesSpinal Cord Assesment Form PTSureaka PonnusamyNo ratings yet
- WeeFIM Clinical ReviewDocument10 pagesWeeFIM Clinical Reviewsss_sarzzzNo ratings yet
- Activity Analysis, Creativity and Playfulness in Pediatric Occupational TherapyDocument16 pagesActivity Analysis, Creativity and Playfulness in Pediatric Occupational TherapySofia VieiraNo ratings yet
- DyslexiaDocument19 pagesDyslexiaJubie MathewNo ratings yet
- f.02 Intellectual Disabilities (Dr. Rebucal) 04-11-2019Document4 pagesf.02 Intellectual Disabilities (Dr. Rebucal) 04-11-2019Dasha VeeNo ratings yet
- Guidelines Down Syndrome Assessment and Intervention PDFDocument292 pagesGuidelines Down Syndrome Assessment and Intervention PDFZenithaMeidaNo ratings yet
- Cognitive DisordersDocument3 pagesCognitive DisordersKayze UbaldoNo ratings yet
- Parenting - AsdDocument9 pagesParenting - Asdapi-391945267No ratings yet
- The Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsDocument8 pagesThe Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsCarol AlvaradoNo ratings yet
- Late Onset SchizophreniaDocument6 pagesLate Onset SchizophreniaVijay MgNo ratings yet
- AutismMotorSkillEvaluationFINALBESt028.8 27 09Document6 pagesAutismMotorSkillEvaluationFINALBESt028.8 27 09Shayne Tee-MelegritoNo ratings yet
- Group Process: Occupational Therapy Tool of PracticeDocument25 pagesGroup Process: Occupational Therapy Tool of Practiceemesep18No ratings yet
- Kaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationDocument7 pagesKaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationJhudith De Julio BuhayNo ratings yet
- Kaplan & Sadocks Synopsis of Psychiatry, 11th Edition (2015) - 634-711!53!78Document26 pagesKaplan & Sadocks Synopsis of Psychiatry, 11th Edition (2015) - 634-711!53!78Priyanka KrishnaNo ratings yet
- General Self-Efficacy Scale (GSE)Document2 pagesGeneral Self-Efficacy Scale (GSE)Angelus MoreNo ratings yet
- Adults With Autism Spectrum DisorderDocument9 pagesAdults With Autism Spectrum DisorderAnaLaura JulcahuancaNo ratings yet
- Australian Cerbral Palsy PDFDocument148 pagesAustralian Cerbral Palsy PDFnewhaberNo ratings yet
- Short Course 360 Wcpa Aota 2018Document46 pagesShort Course 360 Wcpa Aota 2018api-405162391100% (1)
- SPM IntroduccionDocument20 pagesSPM IntroduccionConstanzaNo ratings yet
- MOHO Intervention Implementation - GUADALQUIVERDocument3 pagesMOHO Intervention Implementation - GUADALQUIVERKoyceNo ratings yet
- CatDocument12 pagesCatnini345No ratings yet
- Development Assessment Scales: Chair Person: DR - Ami Patel Speaker:Dr - YogeshDocument24 pagesDevelopment Assessment Scales: Chair Person: DR - Ami Patel Speaker:Dr - YogeshTharindu WewaldeniyaNo ratings yet
- Handwriting PortfolioDocument8 pagesHandwriting Portfolioapi-254940946No ratings yet
- Aphasia ADocument305 pagesAphasia ANinoska OrtizNo ratings yet
- Atik Indryani, Corina Lisa, Eggy Argumi, SurivianaDocument13 pagesAtik Indryani, Corina Lisa, Eggy Argumi, SurivianapediatricaugmNo ratings yet
- Interpretative Considerations IN THE DRAW A Person TEST Interpretative Considerations IN THE DRAW A Person TESTDocument13 pagesInterpretative Considerations IN THE DRAW A Person TEST Interpretative Considerations IN THE DRAW A Person TESTSuresh LukoseNo ratings yet
- Intervention & Goal Update For Annalise (SP Lab) Taylor StamperDocument3 pagesIntervention & Goal Update For Annalise (SP Lab) Taylor Stamperapi-547889945No ratings yet
- Toilet Training AafpDocument6 pagesToilet Training AafpyusditaoNo ratings yet
- Functional Capacity EvaluationDocument17 pagesFunctional Capacity EvaluationNigel Z NyambuyaNo ratings yet
- Contoh Ot ReportDocument10 pagesContoh Ot ReportHanum HamkaNo ratings yet
- AUTISM 101: A Psychoeducational Intervention For Parents of Newly Diagnosed Children With Autism Spectrum DisorderDocument1 pageAUTISM 101: A Psychoeducational Intervention For Parents of Newly Diagnosed Children With Autism Spectrum DisorderAUCDNo ratings yet
- Screening MMSE PaediatricsDocument14 pagesScreening MMSE PaediatricsFrancisco J. RapelaNo ratings yet
- OT - Milestone RetypedDocument6 pagesOT - Milestone RetypedAubrey Vale SagunNo ratings yet
- FIM ManualDocument24 pagesFIM ManualAnshuman MihirNo ratings yet
- Beery Vmi Performance in Autism Spectrum DisorderDocument33 pagesBeery Vmi Performance in Autism Spectrum DisorderJayminertri Minorous100% (1)
- Case ReportDocument9 pagesCase ReportsadiaNo ratings yet
- Dads and AutismDocument50 pagesDads and AutismcirclestretchNo ratings yet
- Canadian Occupational Performance Measure NOC LinkDocument3 pagesCanadian Occupational Performance Measure NOC LinkRatna Sulistya DewiNo ratings yet
- JoDD 17-1 26-37 Schroeder Et AlDocument12 pagesJoDD 17-1 26-37 Schroeder Et AlEspíritu Ciudadano100% (1)
- Functional Capacity Evaluation 1Document114 pagesFunctional Capacity Evaluation 1Bishal BistaNo ratings yet
- Quick DASHDocument4 pagesQuick DASHKennedy Hindley100% (1)
- The Children's Eating Behavior InventoryDocument14 pagesThe Children's Eating Behavior Inventoryguilherme augusto paroNo ratings yet
- Peds Soap NoteDocument4 pagesPeds Soap Noteapi-488745276No ratings yet
- Functional Assessment Checklist For Programmeing of Children With Profound Mental Retardation (Facp-Pmr)Document20 pagesFunctional Assessment Checklist For Programmeing of Children With Profound Mental Retardation (Facp-Pmr)HimaniNo ratings yet
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeFrom EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeNo ratings yet
- MEETING 5 - Describing PeopleDocument6 pagesMEETING 5 - Describing Peoplerizky.ameliaNo ratings yet
- Uruguay The Owners Manual 5th EdDocument240 pagesUruguay The Owners Manual 5th EdlinkgineerNo ratings yet
- Note On Comparison On IFRS 17 and IAS 19Document2 pagesNote On Comparison On IFRS 17 and IAS 19xinaxulaNo ratings yet
- Statistics Final Pre TestDocument4 pagesStatistics Final Pre TestLorienelNo ratings yet
- PCG 30 September 2023 Quarterly Bursa AnnouncementDocument24 pagesPCG 30 September 2023 Quarterly Bursa AnnouncementoodidayooNo ratings yet
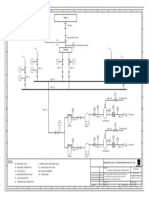
- Schematic For Tank Wagon Decanting Project PDFDocument1 pageSchematic For Tank Wagon Decanting Project PDFlataNo ratings yet
- 9 PowerPoint 2013Document23 pages9 PowerPoint 2013Justz CollectsNo ratings yet
- OsiSense XU XUK8TAE1MM12 DocumentDocument6 pagesOsiSense XU XUK8TAE1MM12 Documentحمزة صباحNo ratings yet
- Getting To Grips With FDADocument84 pagesGetting To Grips With FDATanishq VashisthNo ratings yet
- Electricity & MagnetismDocument18 pagesElectricity & MagnetismM HASIN ISHMAM JEETNo ratings yet
- Dav Gandhinagar Holiday HomeworkDocument8 pagesDav Gandhinagar Holiday Homeworkafodfexskdfrxb100% (1)
- Lecture Notes Week 3 CanonsDocument11 pagesLecture Notes Week 3 CanonsAnna Mharize TanoNo ratings yet
- JOGCan 2018 Fetal Surveillance A AntepartumDocument21 pagesJOGCan 2018 Fetal Surveillance A AntepartumMiguel Guillermo Salazar ClavijoNo ratings yet
- Different Types of Loading SchemesDocument14 pagesDifferent Types of Loading SchemesChintan100% (1)
- sr1 Cup Infopack 2016Document8 pagessr1 Cup Infopack 2016Stef PoienaruNo ratings yet
- 1 s2.0 S0959652610001368 MainDocument10 pages1 s2.0 S0959652610001368 Mainducduy55No ratings yet
- 2 Terms and Definitions SectionDocument12 pages2 Terms and Definitions SectionJawed AkhterNo ratings yet
- Light Emitting Diode PresentationDocument22 pagesLight Emitting Diode PresentationRetro GamerNo ratings yet
- JFFS3 Design Issues: Artem B. BityutskiyDocument36 pagesJFFS3 Design Issues: Artem B. Bityutskiyolena1000000No ratings yet
- WWW Interfarfacing ComDocument13 pagesWWW Interfarfacing ComspiraldaoNo ratings yet
- Analysis of IoT in Healthcare and Computer TechnologyDocument16 pagesAnalysis of IoT in Healthcare and Computer TechnologyBhamini SekarNo ratings yet
- BKM Chapter 9Document4 pagesBKM Chapter 9Ana Nives RadovićNo ratings yet
- Team EkowDocument4 pagesTeam EkowDavid Ekow NketsiahNo ratings yet
- SnsjvuDocument112 pagesSnsjvudocwavy9481No ratings yet
- FAMY Brief Profile (2012)Document18 pagesFAMY Brief Profile (2012)Arlon Ryan ChavezNo ratings yet
- Opium 160604163652Document14 pagesOpium 160604163652roberto cabungcagNo ratings yet
- Finpro FeatureDocument2 pagesFinpro FeaturesinglerakeshNo ratings yet
- MWL 1.0 (Tournament Rules 3.0.2)Document8 pagesMWL 1.0 (Tournament Rules 3.0.2)peterNo ratings yet

























































































Download as pdf or txt
You might also like
- Wickes UnderlayDocument2 pagesWickes UnderlayfloodanddrainageNo ratings yet
- AOTA Exam PrepDocument2 pagesAOTA Exam PrepKenny ClayNo ratings yet
- Assessing Childhood Depression From Multiple Perspectives Via The CDI 2 ToolkitDocument53 pagesAssessing Childhood Depression From Multiple Perspectives Via The CDI 2 ToolkitSamar DakkakNo ratings yet
- OARS Adl IadlDocument5 pagesOARS Adl IadlSamuelNo ratings yet
- SLD GuidelinesDocument231 pagesSLD Guidelinesgryphon688No ratings yet
- RCI - Book On LD PDFDocument49 pagesRCI - Book On LD PDFNikhil Kumar DasNo ratings yet
- Helping You To Assess Cognition: A Practical Toolkit For CliniciansDocument45 pagesHelping You To Assess Cognition: A Practical Toolkit For Cliniciansdaniel serraniNo ratings yet
- Wolf Motor Function Test PDFDocument31 pagesWolf Motor Function Test PDFLydia MartínNo ratings yet
- Membership List: Russell 3000® IndexDocument33 pagesMembership List: Russell 3000® IndexJordi Oller SánchezNo ratings yet
- Functional Capacity Evaluation TemplateDocument11 pagesFunctional Capacity Evaluation TemplateMalik Muhammad Bilal Ali NissoanaNo ratings yet
- Modified Interest Checklist PDFDocument2 pagesModified Interest Checklist PDFMas EdoNo ratings yet
- Wee FimDocument9 pagesWee FimdeffyNo ratings yet
- Examiner's Manual & Technical Report: The Early Learning Accomplishment Profile EditionDocument48 pagesExaminer's Manual & Technical Report: The Early Learning Accomplishment Profile EditionRocioNo ratings yet
- Mini-Mental State Exam: 1 Orientation Questions ScoreDocument1 pageMini-Mental State Exam: 1 Orientation Questions ScoreAbegail GallardoNo ratings yet
- Functional AssesmentDocument22 pagesFunctional AssesmentHeri WibisonoNo ratings yet
- Global Developmental DelayDocument6 pagesGlobal Developmental DelayLiza Perlas Policarpio CarpioNo ratings yet
- Spinal Cord Assesment Form PTDocument8 pagesSpinal Cord Assesment Form PTSureaka PonnusamyNo ratings yet
- WeeFIM Clinical ReviewDocument10 pagesWeeFIM Clinical Reviewsss_sarzzzNo ratings yet
- Activity Analysis, Creativity and Playfulness in Pediatric Occupational TherapyDocument16 pagesActivity Analysis, Creativity and Playfulness in Pediatric Occupational TherapySofia VieiraNo ratings yet
- DyslexiaDocument19 pagesDyslexiaJubie MathewNo ratings yet
- f.02 Intellectual Disabilities (Dr. Rebucal) 04-11-2019Document4 pagesf.02 Intellectual Disabilities (Dr. Rebucal) 04-11-2019Dasha VeeNo ratings yet
- Guidelines Down Syndrome Assessment and Intervention PDFDocument292 pagesGuidelines Down Syndrome Assessment and Intervention PDFZenithaMeidaNo ratings yet
- Cognitive DisordersDocument3 pagesCognitive DisordersKayze UbaldoNo ratings yet
- Parenting - AsdDocument9 pagesParenting - Asdapi-391945267No ratings yet
- The Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsDocument8 pagesThe Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsCarol AlvaradoNo ratings yet
- Late Onset SchizophreniaDocument6 pagesLate Onset SchizophreniaVijay MgNo ratings yet
- AutismMotorSkillEvaluationFINALBESt028.8 27 09Document6 pagesAutismMotorSkillEvaluationFINALBESt028.8 27 09Shayne Tee-MelegritoNo ratings yet
- Group Process: Occupational Therapy Tool of PracticeDocument25 pagesGroup Process: Occupational Therapy Tool of Practiceemesep18No ratings yet
- Kaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationDocument7 pagesKaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationJhudith De Julio BuhayNo ratings yet
- Kaplan & Sadocks Synopsis of Psychiatry, 11th Edition (2015) - 634-711!53!78Document26 pagesKaplan & Sadocks Synopsis of Psychiatry, 11th Edition (2015) - 634-711!53!78Priyanka KrishnaNo ratings yet
- General Self-Efficacy Scale (GSE)Document2 pagesGeneral Self-Efficacy Scale (GSE)Angelus MoreNo ratings yet
- Adults With Autism Spectrum DisorderDocument9 pagesAdults With Autism Spectrum DisorderAnaLaura JulcahuancaNo ratings yet
- Australian Cerbral Palsy PDFDocument148 pagesAustralian Cerbral Palsy PDFnewhaberNo ratings yet
- Short Course 360 Wcpa Aota 2018Document46 pagesShort Course 360 Wcpa Aota 2018api-405162391100% (1)
- SPM IntroduccionDocument20 pagesSPM IntroduccionConstanzaNo ratings yet
- MOHO Intervention Implementation - GUADALQUIVERDocument3 pagesMOHO Intervention Implementation - GUADALQUIVERKoyceNo ratings yet
- CatDocument12 pagesCatnini345No ratings yet
- Development Assessment Scales: Chair Person: DR - Ami Patel Speaker:Dr - YogeshDocument24 pagesDevelopment Assessment Scales: Chair Person: DR - Ami Patel Speaker:Dr - YogeshTharindu WewaldeniyaNo ratings yet
- Handwriting PortfolioDocument8 pagesHandwriting Portfolioapi-254940946No ratings yet
- Aphasia ADocument305 pagesAphasia ANinoska OrtizNo ratings yet
- Atik Indryani, Corina Lisa, Eggy Argumi, SurivianaDocument13 pagesAtik Indryani, Corina Lisa, Eggy Argumi, SurivianapediatricaugmNo ratings yet
- Interpretative Considerations IN THE DRAW A Person TEST Interpretative Considerations IN THE DRAW A Person TESTDocument13 pagesInterpretative Considerations IN THE DRAW A Person TEST Interpretative Considerations IN THE DRAW A Person TESTSuresh LukoseNo ratings yet
- Intervention & Goal Update For Annalise (SP Lab) Taylor StamperDocument3 pagesIntervention & Goal Update For Annalise (SP Lab) Taylor Stamperapi-547889945No ratings yet
- Toilet Training AafpDocument6 pagesToilet Training AafpyusditaoNo ratings yet
- Functional Capacity EvaluationDocument17 pagesFunctional Capacity EvaluationNigel Z NyambuyaNo ratings yet
- Contoh Ot ReportDocument10 pagesContoh Ot ReportHanum HamkaNo ratings yet
- AUTISM 101: A Psychoeducational Intervention For Parents of Newly Diagnosed Children With Autism Spectrum DisorderDocument1 pageAUTISM 101: A Psychoeducational Intervention For Parents of Newly Diagnosed Children With Autism Spectrum DisorderAUCDNo ratings yet
- Screening MMSE PaediatricsDocument14 pagesScreening MMSE PaediatricsFrancisco J. RapelaNo ratings yet
- OT - Milestone RetypedDocument6 pagesOT - Milestone RetypedAubrey Vale SagunNo ratings yet
- FIM ManualDocument24 pagesFIM ManualAnshuman MihirNo ratings yet
- Beery Vmi Performance in Autism Spectrum DisorderDocument33 pagesBeery Vmi Performance in Autism Spectrum DisorderJayminertri Minorous100% (1)
- Case ReportDocument9 pagesCase ReportsadiaNo ratings yet
- Dads and AutismDocument50 pagesDads and AutismcirclestretchNo ratings yet
- Canadian Occupational Performance Measure NOC LinkDocument3 pagesCanadian Occupational Performance Measure NOC LinkRatna Sulistya DewiNo ratings yet
- JoDD 17-1 26-37 Schroeder Et AlDocument12 pagesJoDD 17-1 26-37 Schroeder Et AlEspíritu Ciudadano100% (1)
- Functional Capacity Evaluation 1Document114 pagesFunctional Capacity Evaluation 1Bishal BistaNo ratings yet
- Quick DASHDocument4 pagesQuick DASHKennedy Hindley100% (1)
- The Children's Eating Behavior InventoryDocument14 pagesThe Children's Eating Behavior Inventoryguilherme augusto paroNo ratings yet
- Peds Soap NoteDocument4 pagesPeds Soap Noteapi-488745276No ratings yet
- Functional Assessment Checklist For Programmeing of Children With Profound Mental Retardation (Facp-Pmr)Document20 pagesFunctional Assessment Checklist For Programmeing of Children With Profound Mental Retardation (Facp-Pmr)HimaniNo ratings yet
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeFrom EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeNo ratings yet
- MEETING 5 - Describing PeopleDocument6 pagesMEETING 5 - Describing Peoplerizky.ameliaNo ratings yet
- Uruguay The Owners Manual 5th EdDocument240 pagesUruguay The Owners Manual 5th EdlinkgineerNo ratings yet
- Note On Comparison On IFRS 17 and IAS 19Document2 pagesNote On Comparison On IFRS 17 and IAS 19xinaxulaNo ratings yet
- Statistics Final Pre TestDocument4 pagesStatistics Final Pre TestLorienelNo ratings yet
- PCG 30 September 2023 Quarterly Bursa AnnouncementDocument24 pagesPCG 30 September 2023 Quarterly Bursa AnnouncementoodidayooNo ratings yet
- Schematic For Tank Wagon Decanting Project PDFDocument1 pageSchematic For Tank Wagon Decanting Project PDFlataNo ratings yet
- 9 PowerPoint 2013Document23 pages9 PowerPoint 2013Justz CollectsNo ratings yet
- OsiSense XU XUK8TAE1MM12 DocumentDocument6 pagesOsiSense XU XUK8TAE1MM12 Documentحمزة صباحNo ratings yet
- Getting To Grips With FDADocument84 pagesGetting To Grips With FDATanishq VashisthNo ratings yet
- Electricity & MagnetismDocument18 pagesElectricity & MagnetismM HASIN ISHMAM JEETNo ratings yet
- Dav Gandhinagar Holiday HomeworkDocument8 pagesDav Gandhinagar Holiday Homeworkafodfexskdfrxb100% (1)
- Lecture Notes Week 3 CanonsDocument11 pagesLecture Notes Week 3 CanonsAnna Mharize TanoNo ratings yet
- JOGCan 2018 Fetal Surveillance A AntepartumDocument21 pagesJOGCan 2018 Fetal Surveillance A AntepartumMiguel Guillermo Salazar ClavijoNo ratings yet
- Different Types of Loading SchemesDocument14 pagesDifferent Types of Loading SchemesChintan100% (1)
- sr1 Cup Infopack 2016Document8 pagessr1 Cup Infopack 2016Stef PoienaruNo ratings yet
- 1 s2.0 S0959652610001368 MainDocument10 pages1 s2.0 S0959652610001368 Mainducduy55No ratings yet
- 2 Terms and Definitions SectionDocument12 pages2 Terms and Definitions SectionJawed AkhterNo ratings yet
- Light Emitting Diode PresentationDocument22 pagesLight Emitting Diode PresentationRetro GamerNo ratings yet
- JFFS3 Design Issues: Artem B. BityutskiyDocument36 pagesJFFS3 Design Issues: Artem B. Bityutskiyolena1000000No ratings yet
- WWW Interfarfacing ComDocument13 pagesWWW Interfarfacing ComspiraldaoNo ratings yet
- Analysis of IoT in Healthcare and Computer TechnologyDocument16 pagesAnalysis of IoT in Healthcare and Computer TechnologyBhamini SekarNo ratings yet
- BKM Chapter 9Document4 pagesBKM Chapter 9Ana Nives RadovićNo ratings yet
- Team EkowDocument4 pagesTeam EkowDavid Ekow NketsiahNo ratings yet
- SnsjvuDocument112 pagesSnsjvudocwavy9481No ratings yet
- FAMY Brief Profile (2012)Document18 pagesFAMY Brief Profile (2012)Arlon Ryan ChavezNo ratings yet
- Opium 160604163652Document14 pagesOpium 160604163652roberto cabungcagNo ratings yet
- Finpro FeatureDocument2 pagesFinpro FeaturesinglerakeshNo ratings yet
- MWL 1.0 (Tournament Rules 3.0.2)Document8 pagesMWL 1.0 (Tournament Rules 3.0.2)peterNo ratings yet