Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Precalculus Functions and Graphs 13th Edition Swokowski Test BankDocument6 pagesPrecalculus Functions and Graphs 13th Edition Swokowski Test Bankjohnboonepieqngfrdx100% (14)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Acronis #CyberFit Cloud Tech Fundamentals 2022-Comprimido (1) - 1-150Document150 pagesAcronis #CyberFit Cloud Tech Fundamentals 2022-Comprimido (1) - 1-150Soportech RDNo ratings yet
- Prestige Medical Classic 2100 ManualDocument72 pagesPrestige Medical Classic 2100 Manualwael26724734083No ratings yet
- 1 s2.0 S1388245717311641 PDFDocument14 pages1 s2.0 S1388245717311641 PDFStephii AguirreNo ratings yet
- 3 s2.0 B9780702073373000080 PDFDocument66 pages3 s2.0 B9780702073373000080 PDFStephii AguirreNo ratings yet
- Hearing and Equilibrium: Disorders of The Auditory SystemDocument11 pagesHearing and Equilibrium: Disorders of The Auditory SystemStephii AguirreNo ratings yet
- Potencialesevocadosdermatmicos PDFDocument8 pagesPotencialesevocadosdermatmicos PDFStephii AguirreNo ratings yet
- Prognostic Factors and Outcome of Treatment in Perthes' DiseaseDocument8 pagesPrognostic Factors and Outcome of Treatment in Perthes' DiseaseStephii AguirreNo ratings yet
- Afd 021019 1 1B 50Document100 pagesAfd 021019 1 1B 50Sab-Win DamadNo ratings yet
- Hearts of Care Community Hospital Project ProposalDocument33 pagesHearts of Care Community Hospital Project ProposalWALGEN TRADINGNo ratings yet
- Avoiding Sentence ErrorsDocument26 pagesAvoiding Sentence Errorsapi-327193447No ratings yet
- PatentDocument14 pagesPatentTuvshinjargal MoyorNo ratings yet
- Polymer Degradation and Stability: Long Yan, Zhisheng Xu, Nan DengDocument13 pagesPolymer Degradation and Stability: Long Yan, Zhisheng Xu, Nan DengEkansh ChoudharyNo ratings yet
- Liquid in Glass ThermometerDocument21 pagesLiquid in Glass Thermometerkamyar farsNo ratings yet
- Applying Theorems On Triangle Inequalities (Exterior Angle Inequality Theorem)Document3 pagesApplying Theorems On Triangle Inequalities (Exterior Angle Inequality Theorem)leonardoalbor05No ratings yet
- Social Capital, Civil Society and Development: Francis FukuyamaDocument14 pagesSocial Capital, Civil Society and Development: Francis FukuyamaBruno NeneNo ratings yet
- 55pfl8007k 12 Dfu EngDocument30 pages55pfl8007k 12 Dfu EngHEMANTH BATTULANo ratings yet
- An Overview of The Research of Psychological Entitlement. Definitions and Conceptual CharacteristicsDocument13 pagesAn Overview of The Research of Psychological Entitlement. Definitions and Conceptual CharacteristicsFarah AniaNo ratings yet
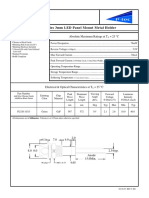
- PL320 Series 3mm LED Panel Mount Metal Holder: Features Absolute Maximum Ratings at T 25 °CDocument1 pagePL320 Series 3mm LED Panel Mount Metal Holder: Features Absolute Maximum Ratings at T 25 °CJajang JajaNo ratings yet
- Sprinkler System Design GuidelinesDocument2 pagesSprinkler System Design GuidelinesaneeshNo ratings yet
- Determination of Molecular Weight Through Boiling Point ElevationDocument1 pageDetermination of Molecular Weight Through Boiling Point ElevationremNo ratings yet
- 25 191 1 PB PDFDocument11 pages25 191 1 PB PDFRaihatil UmmiNo ratings yet
- Object Detection Using Ryze Tello Drone With Help of Mask-RCNNDocument7 pagesObject Detection Using Ryze Tello Drone With Help of Mask-RCNNAadith Thillai Arasu SNo ratings yet
- Software ListingDocument5 pagesSoftware ListingStefan RadaNo ratings yet
- The Cell As An Open SystemDocument2 pagesThe Cell As An Open SystemmunawarNo ratings yet
- The Impact of Psak 73 Implementation On Leases in Indonesia Telecommunication CompaniesDocument17 pagesThe Impact of Psak 73 Implementation On Leases in Indonesia Telecommunication CompaniesAnin YusufNo ratings yet
- Persuasive Essay Stem Cell ResearchDocument5 pagesPersuasive Essay Stem Cell Researchhqovwpaeg100% (2)
- Donau CarbonDocument2 pagesDonau CarbonLim Chee SiangNo ratings yet
- Jestine Seva - PEModuleWeek5&6Document5 pagesJestine Seva - PEModuleWeek5&6Mike AlbaNo ratings yet
- 170989-Article Text-439183-1-10-20180515Document6 pages170989-Article Text-439183-1-10-20180515mehwish maqboolNo ratings yet
- Janus MV FM200 BrochureDocument22 pagesJanus MV FM200 BrochurenoisNo ratings yet
- Botanical Inks Plant-to-Print DyesDocument276 pagesBotanical Inks Plant-to-Print DyesNoémi Gyimóthy100% (3)
- Election New PPT - 231125 - 174550.pdf - 20231125 - 174959 - 0000Document12 pagesElection New PPT - 231125 - 174550.pdf - 20231125 - 174959 - 0000T SERIESNo ratings yet
- Comprehensive Analysis of Software Development Life Cycle ModelsDocument6 pagesComprehensive Analysis of Software Development Life Cycle ModelsWiddy AmandaNo ratings yet
- Butts Spatial DiDDocument35 pagesButts Spatial DiDpvaibhyNo ratings yet