Download as pdf or txt
You might also like
- Anecdotal RecordsDocument21 pagesAnecdotal Recordsvanshika thukral80% (10)
- Advanced Airway Management PrintableDocument8 pagesAdvanced Airway Management PrintableMiranda PermatasariNo ratings yet
- Galbreath Treatment Ear DrainageDocument5 pagesGalbreath Treatment Ear DrainageLenEll KelleyNo ratings yet
- Mesenteric Venous Thrombosis NejmDocument6 pagesMesenteric Venous Thrombosis NejmJUAN LUIS PASAPERANo ratings yet
- Grommets (Ventilation Tubes) For Recurrent Acute Otitis Media in Children (Review)Document60 pagesGrommets (Ventilation Tubes) For Recurrent Acute Otitis Media in Children (Review)yenny handayani sihiteNo ratings yet
- Pediatric Hemophilia: A Review: Roshni Kulkarni, M.D., and J. Michael Soucie, PH.DDocument8 pagesPediatric Hemophilia: A Review: Roshni Kulkarni, M.D., and J. Michael Soucie, PH.Ddwifitri_hfNo ratings yet
- Approaches To Manual Ventilation: John D Davies MA RRT FAARC, Brian K Costa RRT, and Anthony J Asciutto RRTDocument15 pagesApproaches To Manual Ventilation: John D Davies MA RRT FAARC, Brian K Costa RRT, and Anthony J Asciutto RRTAisyah ZahraNo ratings yet
- ATLS Dan Fraktur Coret2Document58 pagesATLS Dan Fraktur Coret2dessyNo ratings yet
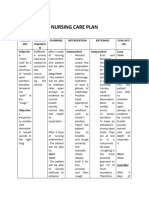
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationDanilo Clerigo Sr.No ratings yet
- BLS ACLS ComplilationDocument218 pagesBLS ACLS ComplilationJannen Casas100% (1)
- Perry2008 2Document12 pagesPerry2008 2luis castroNo ratings yet
- Resuscitation: Pediatric Basic and Advanced Life SupportDocument51 pagesResuscitation: Pediatric Basic and Advanced Life SupportHeru SetiawanNo ratings yet
- NCM 112 Lab (Prelims)Document14 pagesNCM 112 Lab (Prelims)Erica Mei CapiliNo ratings yet
- Approach To Trauma PatientsDocument45 pagesApproach To Trauma PatientsSarahNo ratings yet
- Management of The Unconscious PatientDocument9 pagesManagement of The Unconscious PatientDaramola JuwonNo ratings yet
- 2.1. Trauma and Critical CareDocument13 pages2.1. Trauma and Critical CareMiguel C. DolotNo ratings yet
- Airway and Ventilatory ManagementDocument8 pagesAirway and Ventilatory ManagementAshen DissanayakaNo ratings yet
- Uniform Care of ResuscitationDocument48 pagesUniform Care of ResuscitationKIMS qualityNo ratings yet
- 2.1. Trauma and Critical Care (Jerome Villacorta's Conflicted Copy 2013-08-24)Document12 pages2.1. Trauma and Critical Care (Jerome Villacorta's Conflicted Copy 2013-08-24)Miguel C. DolotNo ratings yet
- (Sep. 6) CPR RationalizationDocument21 pages(Sep. 6) CPR RationalizationJamaica Leslie NovenoNo ratings yet
- Airway Management in The Trauma PatientDocument17 pagesAirway Management in The Trauma PatientFelipe Paulo de AssisNo ratings yet
- Cardio Pulmonary ResuscitationDocument5 pagesCardio Pulmonary ResuscitationRenee RoSeNo ratings yet
- Basic Life Support: Group 1Document40 pagesBasic Life Support: Group 1Patricia CaladoNo ratings yet
- BLS Provider ManualDocument12 pagesBLS Provider Manualshreyanand005No ratings yet
- Adult Cardiopulmonary ResuscitationDocument3 pagesAdult Cardiopulmonary ResuscitationSerious LeoNo ratings yet
- New Update 35 Laryngospasm PDFDocument4 pagesNew Update 35 Laryngospasm PDFRobertaNo ratings yet
- ANZCOR Guideline 4 - Airway: Who Does This Guideline Apply To?Document9 pagesANZCOR Guideline 4 - Airway: Who Does This Guideline Apply To?CatNo ratings yet
- Airway ManagementDocument11 pagesAirway Managementmegayani santosoNo ratings yet
- NCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsDocument7 pagesNCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsViviene Faye FombuenaNo ratings yet
- Physiological Overview in Relation To PracticeDocument52 pagesPhysiological Overview in Relation To PracticedrkhaledassemNo ratings yet
- Nursing Care Plan: Assessm ENT Nursing Diagnos IS Planning Intervention Rationale Evaluati ON Subjectiv eDocument4 pagesNursing Care Plan: Assessm ENT Nursing Diagnos IS Planning Intervention Rationale Evaluati ON Subjectiv eJ. TSNo ratings yet
- Risk For Aspiration Related To Impaired Swallowing Secondary To Cerebrovascular AccidentDocument3 pagesRisk For Aspiration Related To Impaired Swallowing Secondary To Cerebrovascular AccidentChenee MabulayNo ratings yet
- Manual Defibrillation - Information SheetDocument6 pagesManual Defibrillation - Information SheetNurul Juan PratamaNo ratings yet
- Cardiopulmonary Resuscitation (CPR) Is A Lifesaving Technique Useful in Many Emergencies, Including A Heart Attack or Near Drowning, in Which Someone's Breathing or Heartbeat Has StoppedDocument5 pagesCardiopulmonary Resuscitation (CPR) Is A Lifesaving Technique Useful in Many Emergencies, Including A Heart Attack or Near Drowning, in Which Someone's Breathing or Heartbeat Has StoppedMukesh KumarNo ratings yet
- Cardiopulmonary ResuscitationDocument6 pagesCardiopulmonary ResuscitationImongheartNo ratings yet
- The Upper Airway During Anaesthesia: D. R. Hillman, P. R. Platt and P. R. EastwoodDocument9 pagesThe Upper Airway During Anaesthesia: D. R. Hillman, P. R. Platt and P. R. EastwoodFendy PrasetyoNo ratings yet
- Disaster and Military Medicine Department Guzar, 2 "Premedical Aid in Extreme Situations"Document27 pagesDisaster and Military Medicine Department Guzar, 2 "Premedical Aid in Extreme Situations"nirav patelNo ratings yet
- Structured Approach To Managing Emergencies in Pregnancy and ChildhoodDocument10 pagesStructured Approach To Managing Emergencies in Pregnancy and ChildhoodrebeccaNo ratings yet
- Alur Resusitasi NeonatusDocument5 pagesAlur Resusitasi NeonatusNova SibueaNo ratings yet
- Ex TurbaciónDocument4 pagesEx TurbaciónAlberto EscotoNo ratings yet
- SK Tim Manajemen KomplainDocument33 pagesSK Tim Manajemen KomplainSanny GondowardojoNo ratings yet
- Management Airway: ABC of Major Trauma of The UpperDocument4 pagesManagement Airway: ABC of Major Trauma of The UpperJuana RosalesNo ratings yet
- The Primary SurveyDocument18 pagesThe Primary SurveyvhiraNo ratings yet
- HN9 Pharynx 03Document12 pagesHN9 Pharynx 03Farhan HasbiNo ratings yet
- Jurnal Laryngeal TraumaDocument7 pagesJurnal Laryngeal TraumaadindaNo ratings yet
- Basic Life Support - Adult: First Issued By/date Issue Planned Review DateDocument15 pagesBasic Life Support - Adult: First Issued By/date Issue Planned Review DateyvesramosNo ratings yet
- 2.bases Fisiologicas de Los Sint y Signnos Resp PDFDocument5 pages2.bases Fisiologicas de Los Sint y Signnos Resp PDFKatherine CabezasNo ratings yet
- First Aid For Dive Accidents: Know and Understand Basic Cardiopulmonary Resuscitation (CPR)Document2 pagesFirst Aid For Dive Accidents: Know and Understand Basic Cardiopulmonary Resuscitation (CPR)wyma01No ratings yet
- Checklist On CPR (Cardio Pulmonary Resuscitation) : Action Rationale RemarksDocument3 pagesChecklist On CPR (Cardio Pulmonary Resuscitation) : Action Rationale RemarksRuchika Kaushal0% (2)
- Endotracheal Tube IntubationDocument5 pagesEndotracheal Tube IntubationKim Kristine D. GuillenNo ratings yet
- Continued: Using A Manual Resuscitation Bag, With Mask (Left) or Connected To An Artificial Airway (Right)Document2 pagesContinued: Using A Manual Resuscitation Bag, With Mask (Left) or Connected To An Artificial Airway (Right)Ian TuNo ratings yet
- Basic Concepts To Basic Life SupportDocument8 pagesBasic Concepts To Basic Life SupportHynne Jhea EchavezNo ratings yet
- Clinical SkilllllllllllllllDocument12 pagesClinical SkilllllllllllllllAlmira Putri100% (1)
- 170-VDR JRC JCY-1900 Instruct Manual 1-2-2021Document171 pages170-VDR JRC JCY-1900 Instruct Manual 1-2-2021Komar ElectricNo ratings yet
- Guideline 4 Airway 220Document9 pagesGuideline 4 Airway 220Nivaldo SantosNo ratings yet
- Basic Life SupportDocument2 pagesBasic Life SupportAhmad Khair Ahmad BazliNo ratings yet
- First Aid Cardio Pulmonary Resuscitation: Presented By, Mrs. Shini Nursing Tutor PNSDocument43 pagesFirst Aid Cardio Pulmonary Resuscitation: Presented By, Mrs. Shini Nursing Tutor PNSShini SimonNo ratings yet
- The General Method For Airway ObstructionDocument6 pagesThe General Method For Airway ObstructionNila SariNo ratings yet
- Skills Training Manual BookDocument19 pagesSkills Training Manual BookMuhammad SawalNo ratings yet
- ABCDE ApproachDocument7 pagesABCDE ApproachmariamNo ratings yet
- Approach To A Trauma PatientDocument48 pagesApproach To A Trauma PatientSocial Media workingNo ratings yet
- Pe BLSDocument4 pagesPe BLSchn pastranaNo ratings yet
- Obat - Obatan Di Bedah SarafDocument16 pagesObat - Obatan Di Bedah Sarafditya_madridistasNo ratings yet
- Spine Emergencies: Spinal Cord Injury (SCI) - The BasicsDocument67 pagesSpine Emergencies: Spinal Cord Injury (SCI) - The Basicsditya_madridistasNo ratings yet
- Cedera Saraf Spinal Cervical DR FAZDocument52 pagesCedera Saraf Spinal Cervical DR FAZditya_madridistasNo ratings yet
- Pengaruh Minuman Kopi Terhadap MahasiswaDocument4 pagesPengaruh Minuman Kopi Terhadap Mahasiswaditya_madridistasNo ratings yet
- اجازة مرضية وليد علاقيDocument1 pageاجازة مرضية وليد علاقيابو محمد ابومحمدNo ratings yet
- Newer Formulations of The Triptans: Advances in Migraine ManagementDocument21 pagesNewer Formulations of The Triptans: Advances in Migraine ManagementShivam BhadauriaNo ratings yet
- English ExamsDocument5 pagesEnglish Examskarina_gillaNo ratings yet
- Phoenix Sepsis ScoreDocument3 pagesPhoenix Sepsis ScoreNur Amaliah idrusNo ratings yet
- Lecture 01 Overview RP in DR and IR RTC Accra 2011Document30 pagesLecture 01 Overview RP in DR and IR RTC Accra 2011pramoth_cm1194No ratings yet
- CovidDocument6 pagesCovidMahmoud ElmahdyNo ratings yet
- 40 The Manual Diaphragm Release Technique Improves Diaphragmatic MobilityDocument8 pages40 The Manual Diaphragm Release Technique Improves Diaphragmatic MobilityRenan O. Pravatta PivettaNo ratings yet
- A Guide To What Works For DepressionDocument96 pagesA Guide To What Works For DepressionLynda HernandezNo ratings yet
- Antibiotic Class Summary TableDocument6 pagesAntibiotic Class Summary TableuserherwwweNo ratings yet
- Morphologic and Immunologic Characterization of A Canine Isthmus Mural Folliculitis Resembling Pseudopelade of Humans (Pages 17-24)Document8 pagesMorphologic and Immunologic Characterization of A Canine Isthmus Mural Folliculitis Resembling Pseudopelade of Humans (Pages 17-24)jenNo ratings yet
- Ptosis (Emedicine)Document18 pagesPtosis (Emedicine)lochnezNo ratings yet
- Disturbed Thought Process NCP Gallano May 22 2018Document3 pagesDisturbed Thought Process NCP Gallano May 22 2018Charles Mallari ValdezNo ratings yet
- FIrst Aid For Crush InjuriesDocument14 pagesFIrst Aid For Crush InjuriesGoldenMaidenNo ratings yet
- Health AssessmentDocument18 pagesHealth AssessmentSavita Hanamsagar100% (1)
- Self Declaration Form Details For International Arriving PassengersDocument2 pagesSelf Declaration Form Details For International Arriving PassengersSharafat AliNo ratings yet
- DDE BrochureDocument15 pagesDDE BrochurePritamNo ratings yet
- Pediatric HerniaDocument4 pagesPediatric HerniaRudi haris munandar0% (1)
- Sexualization Doctor PatientDocument5 pagesSexualization Doctor PatientMelvyn Carlo BarroaNo ratings yet
- Jock ItchDocument4 pagesJock ItchFranzelle Estrella ÜNo ratings yet
- Full Chapter Talking Points On Deprescribing in Hospice Care 1St Edition Shrivastava PDFDocument53 pagesFull Chapter Talking Points On Deprescribing in Hospice Care 1St Edition Shrivastava PDFcoral.schaffner27683% (6)
- NCP RequirementsDocument3 pagesNCP RequirementsJasmine JarapNo ratings yet
- Essential Health Care Package For SwazilandDocument75 pagesEssential Health Care Package For SwazilandRae Manar100% (1)
- PCD Commercially Available Devices and Systems 2014 AprilDocument3 pagesPCD Commercially Available Devices and Systems 2014 AprilPedro de LaraNo ratings yet
- PDF Cphims Review Guide Preparing For Success in Healthcare Information and Management Systems 3Rd Edition Healthcare Information and Management Systems Society Himss Ebook Full ChapterDocument54 pagesPDF Cphims Review Guide Preparing For Success in Healthcare Information and Management Systems 3Rd Edition Healthcare Information and Management Systems Society Himss Ebook Full Chapterjose.bailey983100% (3)
- Naukri MansiGirdhar (2y 6m)Document1 pageNaukri MansiGirdhar (2y 6m)Lokesh MaariNo ratings yet
- Mechanical VentilationDocument40 pagesMechanical VentilationPratik SahooNo ratings yet