Professional Documents
Culture Documents
Escala de Apatia de Starkstein
Escala de Apatia de Starkstein
Uploaded by
Vanessa HernandezOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Escala de Apatia de Starkstein
Escala de Apatia de Starkstein
Uploaded by
Vanessa HernandezCopyright:
Available Formats
Reliability, Validity, and Clinical
Correlates of Apathy in
Parkinson’s Disease
Sergio E. Starkstein, M.D., Ph.D.
Helen S. Mayberg, M.D.
ThomasJ. Preziosi, M.D.
Paula Andrezejewski, M.A.
R2mOn Leiguarda, M.D.
Robert G. Robinson, M.D.
The authors examined a consecutive series of 50 D epression and cognitive impairments are well-
known findings in Parkinson’s disease (PD) and
patients for the presence of apathy, depression,
have been the focus of a large number of studies.12 On
anxiety, and neuropsychological deficits using a
the other hand, although apathy has been consistently
neuropsychological battery that included a re- recognized as a frequent psychiatric complication of PD,3
cently designed apathy scale. This scale was found no empirical studies on its frequency and clinical corre-
to be reliable and valid in the diagnosis of apathy lates have been carried out. The lack of an apathy scale
in patients with PD. Of patients in the study, with proven reliability and validity may be one of the
12% showed apathy as their primary psychiatric reasons underlying the scant research in this area, and up
to now the diagnosis of apathy has relied only on subjec-
problem, and 30% were both apathetic and de-
tive clinical impressions.
pressed. Patients with apathy (with or without The present study had three aims: first, to examine the
depression), showed significantly more deficits in reliability and validity of an apathy scale in patients with
both tasks of verbal memory and time-dependent PD; second, to examine the demographic, clinical, and
tasks. Results suggest that apathy is a frequent cognitive correlates of apathy in patients with PD; and
finding in PD, is significantly associated with third, to determine whether apathy could be disassoci-
ated from the presence of depression in patients with PD.
specific cognitive impairments, and may have a
different mechanism than depression.
(The Journal of Neuropsychiatry and Clinical
Neurosciences 1992; 4:134-139)
METHODS
Patients
We examined a consecutive series of 50 patients with
idiopathic PD who attended the neurology clinic at the
Received December 14, 1990; revised June 27, 1991; accepted July 11,
1991. From the Departments of Psychiatry, Neurology, and Nuclear
Medicine, The Johns Hopkins University School of Medicine, Baltimore,
Maryland; Department of Psychiatry, University of Iowa, Iowa City;
and Institute of Neurological Research “Dr. Rau! Carrea,” Buenos Aires,
Argentina. Address reprint requests to Dr. Starkstein, Institute of Neu-
rological Investigation, Ayacucho 2166/68,1112 Buenos Aires, Argen-
tina.
Copyright © 1992 American Psychiatric Press, Inc.
134 VOLUME 4 NUMBER
#{149} 2 SPRING
#{149} 1992
STARKSTEIN et al.
Johns Hopkins Hospital as part of a longitudinal study iner, by a related-other, and by the patient, respectively-
on depression in PD.4 Patients attending the clinic were we felt it might be too demanding for patients with PD.
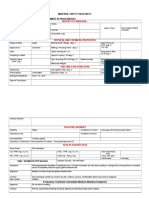
seen for neurological evaluation or management of their In the AS (see Figure 1), each question is read by the
disorder at regular follow-up visits. Our sample was not examiner, and the patient is provided with four
possible
biased toward more severe cases of PD, who are usually answers: “not at all,” “slightly,” “some,” or “a lot.” The
referred to more specialized movement disorder clinics. same scale was piloted in patients with Alzheimer’s dis-
A detailed description of our population is provided ease, Huntington’s disease, and stroke (C. Peyser, M.D.,
elsewhere.4 and P. Fedoroff, M.D., personal communication) and was
found to have very high intra- and interrater reliability.
Neurological Examination Scores range from 0 to 42; higher scores indicate more
The neurological examination was carried out by one of severe apathy.
us (T.J.P.) who was blind to the neuropsychiatric and
neuropsychological data. The evaluation consisted of a Neuropsychological Examination
comprehensive neurological examination and adminis- Mini-Mental State Exam (MMSE): The MMSE’4 is an 11-
tration of a rating scale for symptoms of PD. The rating item examination that has been found to be reliable and
scale measured the presence and severity of tremor, ri- valid in assessing a limited range of cognitive functions.
gidity, and akinesia in the left and right limbs.4 Activities
of daily living were quantified using the Northwestern Wisconsin Card Sorting Test (WCST): The WCST’5 mea-
Disability Scale5 (NWDS). Based on clinical findings, the sures the ability to develop new concepts and to shift sets,
stage of illness was determined using the Hoehn and and it also requires the subject to suppress a previously
Yahr stages.6 correct response and produce a new one. Assessment of
overall proficiency on the test was judged by the number
Psychiatric Examination of categories achieved.
After giving informed consent, patients were adminis-
tered a series of standardized quantitative measures of Controlled Word Association Test (FAS): The FAS’6 ex-
mood, cognitive function, and social connectedness. Ex- amines access to semantic information under time con-
aminations were administered in a private room between straint. Patients were instructed to name as many words
IOAM. and 2 P.M. to minimize any possible effect of diurnal beginning with the letters F, A, and S as they could in 1
mood variation. minute each. Perseverations and intrusions were not in-
The modified Present State Examination7 (PSE), a semi- cluded in the final score.
structured psychiatric interview that elicits symptoms
related to depression and anxiety, was scored by the Trail Making Test: This test’7 examines visual, concep-
examiner. Based on the symptoms elicited using the PSE, tual, and visuomotor tracking under time constraints. In
a psychiatric diagnosis was made using DSM-1118 symp- Trails A, the patient is instructed to draw lines to connect
tom criteria for major or minor (dysthymic) depression.
The method used to convert PSE symptoms to DSM-III FIGURE 1.Apathy Scale. Scoring: For questions 1-8, not at all =
major or minor depression diagnosis was discussed in a 3 points; slightly = 2; some = 1; a lot = 0. For questions
9-14, not at all = 0; slightly = 1; some = 2; a lot = 3.
previous publication.7 We have recently demonstrated
the specificity and sensitivity of the DSM-III criteria in the 1. Are you interested in learning new things?
diagnosis of depression in PD.9 not at all slightly some a lot
The Hamilton Rating Scale for Depression’#{176} and the 2. Does anything interest you?
Hamilton Rating Scale for Anxiety,’1 measuring psycho- 3. Are you concerned about your condition?
4. Do you put much effort into things?
logical and physiological symptoms of depression and
5. Are you always looking for something to do?
anxiety, respectively, were completed by the interviewer.
6. Do you have plans and goals for the future?
Social functioning was quantified by number of social
7. Do you have motivation?
connections, using the Social Ties Checklist12 (STC).
8. Do you have the energy for daily activities?
9. Does someone have to tell you what to do each day?
Apathy in PD
10. Are you indifferent to things?
For the present study, we also used the Apathy Scale
11. Are you unconcerned with many things?
(AS), which is an abridged version of an apathy scale
12. Do you need a push to get started on things?
designed by Robert Mann.’3 Although Mann’s apathy
13. Are you neither happy nor sad, just in between?
scale is more comprehensive than the one we used-it
14. Would you consider yourself apathetic?
features three subscales, which are given by the exam-
JOURNAL OF NEUROPSYCHIATRY 135
APATHY AND PARKINSON’S DISEASE
consecutively numbered circles; in Trails B, the patient is AS scores for all 50 patients showed a bimodal distri-
instructed to connect consecutively numbered and let- bution, and a cutoff score of 14 points separated both
tered circles. modes. Validity was examined by asking a neurologist
who was blind to the AS scores to rate 12 patients as
Symbol Digit Modalities (SDM): The SDM’8 examines apathetic or nonapathetic. He rated 6 patients as apa-
visuoverbal substitution speed. Patients are presented thetic and the remaining 6 as nonapathetic. Apathetic
with a page in which the first row has nine different patients had a significantly higher AS score than non-
symbols with numbers below, followed by several lines apathetic patients (AS scores, mean±SD: apathetic =
containing only symbols. Patients are instructed to say 14.8±5.7; nonapathetic 5.5±2.2; t=3.70, df=10, P<zO.001).
the number that matches each symbol, and the number Using a cutoff score of 14 points, the sensitivity of the
is written by the examiner. scale was 66% and the specificity was 100%.
Based on the frequency distribution of AS scores, pa-
Digit Span: This test’9 examines auditory attention. In tients with AS scores <14 were considered nonapathetic;
the first part (Digits Forward), the patient is asked to those with AS scores 14 were considered apathetic.
repeat a string of numbers exactly as it is given, while in Based on DSM-III criteria, patients were also classified as
the second (Digits Backward) the patient is asked to depressed (major or minor) or nondepressed. Six of the
repeat a string of numbers in reversed order. 50 patients (12%) showed apathy in the absence of de-
pression, 15 patients (30%) had both apathy and depres-
Paired Associative Learning Test (PALT): The PALl’9 ex- sion, 13 patients (26%) had depression but no apathy, and
amines short-term memory. It consists of a series of the remaining 16 patients (32%) had neither apathy nor
paired words (some easy, such as up-down, and some depression.
difficult, such as dark-crush) that are read to the patient.
The patient is later given the first word of the pair and Demographic Findings
has to respond with the second word. No significant between-group differences were found in
any of the demographic variables examined (Table 1).
Although most of the patients underwent the full neu-
ropsychological battery, a few patients could not do some Neurological Findings
of the tests because of visual problems or fatigue. A two-way ANOVA for akinesia scores showed a signif-
icant effect for depression (F=7.65, df=1,46, P<0.01): de-
Statistical Analysis pressed patients had significantly more akinesia than
Statistical analysis was carried out with a two-way anal- nondepressed patients. No significant main effects or
ysis of variance (ANOVA) (factor 1: depression, present interactions were observed for rigidity or tremor
or absent; factor 2: apathy, present or absent) and (Table 2).
planned t-test comparisons. Frequency distributions A two-way ANOVA for NWDS scores showed a sig-
were analyzed using a chi-square test. All P-values are nificant effect for depression (F=6.70, df=1,46, P<0.05):
two-tailed. depressed patients had significantly more severe im-
pairments in activities of daily living than nondepressed
RESULTS TABLE 1. Demographic findings
Depressed +
Apathy Scale Variable Normal Depressed Apathetic Apathetic
Independent ratings of the AS were carried out in a
Numberof patients 16 13 6 15
consecutive group of 11 PD patients by two raters (S.E.S. Age,years 67±9 62± 12 69±7 69±8
and P.A.) on two different days. In a different group of Sex, % female 50 43 34 27
11 patients with PD, the AS was assessed by the same Education,years 15±3 14±4 14±4 14±3
rater on two different occasions (1 week apart). The AS Family history of
showed good interrater reliability (r=0.81, df=10, P<0.01) psychiatric
disorder, % 13 34 50 27
and test-retest reliability (r=0.90, df=10, P<0.01), as well
Personal history of
as high internal consistency, a measure of internal valid-
psychiatric
ity (Cronbach’s a=0.76). Interrater and test-retest re- disorder, % 13 69 17 67
liabilities were high even after using conservative
Note: Values are m eans ± SD for Age and Education.
nonparametnic statistics (Spearman’s p=0.8O, P<0.01, and
*P<0.05.
p=0.82, P<zO.01, respectively).
136 VOLUME 4 NUMBER
#{149} 2 SPRING
#{149} 1992
STARKSTEIN et at.
patients. No significant between-group differences were TABLE 2. Neurological findings
found on levodopa dosage, duration of illness, and fre-
Depressed +
quencies of abnormal involuntary movements or on-off Variable Normal Depressed Apathetic Apathetic
phenomena (Table 2).
Duration of
ilness,years 8.5±2.8 9.6±3.7 11.8±4.8 11.9±7.0
Psychiatric Findings Tremor, score 1.5 ± 1.7 2.6 ± 2.2 2.3 ± 1.9 2.6 ± 2.4
As expected, patients with depression showed signifi- Rigidity, score 2.9 ± 1.2 3.3 ± 1.4 2.8 ± 2.2 3.6 ± 1.5
cantly higher depression scores than apathetic or normal Akinesia, score 3.1 ± 1.5’ 4.7 ± 1.4’ 3.6 ± 2.2’ 4.6 ± 1.4’
patients (Table 3). No significant differences in depres- Levodopa
sion scores were found between apathetic and normal dosage, mg 521 ± 288 690 ± 396 858 ± 473 778 ± 393
patients. Similarly, no significant differences in apathy Northwestern
scores were found between depression-only and normal Disability Scale, . .
score 6.6±4.3 11.2±9.2 7.1±2.4 13.8±8.4
patients. On the other hand, anxiety scores were signif-
Abnormal
icantly higher in depressed patients (F=22.0, df=1,46,
movements, % 25 62 50 27
P<0.0001) (Table 3). No significant between-group differ-
On-off
ences were observed on SIC scores. phenomena, % 13 54 33 40
Note: Values for first 6 variables are means ± SD.
Neuropsychological Findings
.P<0.05.
A two-way ANOVA for MMSE scores showed a signifi-
cant effect for depression (F=6.03, df=1,46, P<0.05): de-
pressed patients had significantly lower MMSE scores TABLE 3. Psychiatric findings
than nondepressed patients. However, there were no Mean Score ± SD
significant effects for apathy and no significant interac-
Depressed +
tions (Table 4).
Measure Normal Depressed Apathetic Apathetic
A two-way ANOVA for FAS scores showed a signifi-
Present State Exam 2.3 ± 2.3’ 13.6 ± 5.3’ 3.0 ± 2.1’ 11.9 ± 3.3’
cant effect for apathy (F=5.44, df=1,46, P<0.05): apathetic
Hamilton Rating Scale
patients had significantly lower scores than nonapathetic
for Depression 3.3 ± 2.6 10.8 ± 3.7 3.6 ± 2.0 8.2 ± 3.5
patients.
Hamilton Rating * #{149}
A two-way ANOVA for Trails B (i.e., time to com- Scale for Anxiety 3.8 ± 4.5 13.8 ± 5.8 4.6 ± 4.0 10.4 ± 4.9
pletion) showed a significant effect for apathy (F=7.68,
Apathy Scale 7.3 ± 2.8’ 10.0 ± 2.0’ 17.1 ± 4.0’ 19.5 ± 3.3’
df=1,46, P<0.01): apathetic patients were significantly Social Ties
slower than nonapathetic patients. When only error-free Checklist 2.7±1.2 3.6±1.7 3.5±1.0 3.4±1.1
performances were considered (regardless of time to
Note: Values are means ± SD.
completion), patients who had only depression obtained
P<0.05.
significantly fewer error-free performances than normal
patients df=1, P<0.05), whereas no significant
differences in the frequency of error-free performances TABLE 4. Neuropsychological findings
were observed between patients with apathy only and
Depressed +
normal patients (2=2.14, df=1, P>0.10). Thus, results on Measure Normal Depressed Apathetic Apathetic
Trails B showed a double disassociation between depres-
Mini-Mental State 28.7 ± 1.1’ 26.3 ± 4.6’ 28.3 ± 1.2’ 25.4 ± 4.5’
sion and apathy: whereas apathy was associated with a
Wisconsin Card
significantly slower, though accurate, performance on Sort 5.2±1.7 3.7±2.5 3.8±2.5 3.5±2.3
Trails B, depression was significantly associated with
Controlled Word
inaccurate, though not slower, performances. (FAS) 41.7 ± 13.1’ 41.6 ± 12.1’ 34.1 ± 10.7’ 31.4 ± 11.9’
On the PALT, there were significant main effects for
Trails A 46.1 ± 18.5 62.9 ± 58.8 63.1 ± 24.8 112.0 ± 82.8
both depression (F=6.55, df=1 ,46, P<0.01) and apathy
TrailsB 116±65’ 203±104’ 229±54’ 235±91’
(F=5.60, df=1,46, P<0.05).
Symbol Digit 38.8 ± 10.0 35.0 ± 12.2 35.0 ± 9.5 30.0 ± 13.2
Although a two-way ANOVA for WCST scores did not
show significant main effects or interactions, when pa- DigitsForward 1.7±1.2 1.8±1.2 1.6±1.0 1.7±1.3
tients were divided into those with normal (6 categories), Digits Backward 2.3 ± 1.1 2.3 ± 1.2 2.0 ± 0.8 2.9 ± 1.2
or abnormal (<6 categories) performances, significantly
Note: Values are means ± SD.
fewer patients with depression only obtained a normal ‘P <0.05.
score as compared with normal patients (x2=S.03, df=1,
JOURNAL OF NEUROPSYCHIATRY 137
APATHY AND PARKINSON’S DISEASE
P<0.05). On the other hand, no significant differences slowing, since slow cognitive processing may produce
were observed between patients with apathy only and significant encoding deficits, which may impair memory
normal patients (x2=189, df=1, P>0.10). performance.27 Mayeux et al.28 also found memory dis-
Finally, no significant between-group differences were turbances in their group of bradyphrenic patients, and
observed on the remaining neuropsychological tasks they suggested that the memory deficit may be related to
(SDN, Trails A, and Digit Span). the defect in vigilance and attention, which subsequently
interferes with the acquisition process of memory.
Although cognitive slowing may be related to motor
DISCUSSION slowing as well, a significant association between brady-
phrenia and motor slowing has never been reported,’28’29
This study, the first to examine empirically the frequency and in the present study there was no significant associ-
and correlates of apathy in PD, showed three main find- ation between apathy and either akinesia or rigidity.
ings. First, we showed the reliability, internal consis- Rogers et al.25 also found a significant association
tency, and validity of an apathy scale in PD. Second, we between bradyphrenia and depression, which may be
found that 12% of a consecutive series of patients with related to our finding that depression and apathy fre-
PD were apathetic and that an additional 30% of patients quently coexist. As a matter of fact, patients with both
had apathy together with depression. Third, we found apathy and depression were the most impaired in all the
that the presence of apathy was significantly associated cognitive tasks with time constraints.
with impairments on neuropsychological tests with time On the other hand, the presence of depression in PD
constraints as well as on verbal memory tasks. was associated with cognitive deficits even in the absence
The correlates of depression in PD have been exten- of apathy. The present study as well as a previous report
sively examined.1 It has been demonstrated that about demonstrate that patients with PD and depression have
40% of a cross-sectional sample of patients with PD have impairments on neuropsychological tasks with no time
major or minor depression,4 and depression was consis- constraints, such as the WCST.
tently found to be more frequent in patients with an early The question that arises from these findings is: what
age of onset of the disease.202’ Moreover, patients with mechanism leads to apathy in PD? One important find-
PD and major depression may show a dementia of de- ing of this study was that some patients had severe
pression, a faster cognitive decline, and metabolic apathy in the absence of depression, suggesting that the
deficits in the inferior frontal cortex.24 mechanism underlying the presence of apathy in PD may
The fact that patients with apathy were similar to PD be independent from the mechanism underlying the
patients without psychiatric problems in terms of demo- presence of depression. That is, depression may not be
graphic variables, duration of illness, and severity of sufficient or necessary to produce apathy in PD.
symptoms of PD suggests that apathy may not be simply Depression in PD has been related to either low
related to the progression of the disease (i.e., more apathy cerebrospinal fluid levels of 5-HIAA (a metabolite of
in later stages). Our finding that patients with apathy and serotonin),27 dysfunction of the meso-cortico-limbic do-
PD had significant deficits in time-dependent cognitive paminergic system,3#{176}or dysfunction of the inferior fron-
tasks (e.g., they produced significantly fewer words start- tal lobe.24 Although the biological basis of apathy in PD
ing with a given letter in 1 minute, and they were signif- has never been systematically examined, Mayeux et al.28
icantly slower, though not less accurate, on Trails B) may recently described a significant correlation between nor-
relate apathy to the concept of bradyphrenia. epinephrine metabolites and cognitive measures of bra-
Rogers et al.25 defined bradyphrenia as a “slowing of dyphrema. They suggested that bradyphrenia may be
cognitive processing associated with impairment of con- secondary to neuronal depletion in the locus ceruleus.
centration and apathy.” Another description of brady- Thus, apathy may be secondary to dysfunction in cate-
phrema that shows its phenomenological similarity to cholaminergic pathways, whereas depression may occur
apathy was provided by Wilson.26 He defined brady- after additional dysfunction of serotonergic and/or infe-
phrenia as “a lethargy of the mind distinguished by a lack rior frontal circuits. On the other hand, depression with-
of interest, initiative, attention, concentration; by fatigue out apathy may be related to the presence of serotonergic
and slow reactions; incommunicative and wishing to be and / or inferior frontal dysfunction in the absence of
left alone, the patient sits and does nothing unless ex- noradrenergic dysfunction.
horted to rouse himself.” Thus, the cognitive slowing so Although much work remains to be done in elucidat-
frequent in patients with PD may be related to the pres- ing the clinical correlates, course, and mechanism of
ence of apathy. The verbal memory deficit shown by apathy in PD, we have developed a scale for the study of
patients with apathy may also be related to cognitive apathy in PD and have demonstrated its reliability, inter-
138 VOLUME 4 NUMBER
#{149} 2 SPRING
#{149} 1992
STARKSTEIN et al.
nal consistency, and validity. We found apathy, with or We thank Robert Mann, M.D., for allowing us to modify his
without depression, to be a frequent finding in patients apathy scale for the present study. This work was supported in
with PD, and to be associated with deficits in specific part by the following National Institutes of Health grants:
neuropsychological tasks. Future studies may demon- Research Scientist Award M1-100163 (R.G.R.), NS15080, and
strate whether patients with apathy develop depression MH40355; and by a gra nt from the University of Buenos Aires
with the progression of the illness and whether changes (S.E.S.), a grant from the Instituto di Tella (S.E.S.), and a
in brain chemistry are specifically associated with apathy National Alliance for Research on Schizophrenia and Depres-
in PD. sion Young Investigator Award (S.E.S.).
References
1. Mayeux R, Williams JBW, Stern Y, et al: Depression and Parkinson’s 16. Benton AL: Differential behavioral effects in frontal lobe disease.
disease. Adv Neurol 1984; 40:241-250 Neuropsychologia 1968; 6:53-60
2. Stern Y, Mayeux R: Intellectual impairments in Parkinson’s disease, 17. Reitan RM: Validity of the Trail Making Test as an indicator of
in Parkinson’s Disease, edited by Yahr MD, Bergmann KJ. New organic brain damage. Percept Mot Skills 1958; 8:271-276
York, Raven, 1986, pp 405-408 18. Smith A: Symbol Digit Modalities Test Manual. Los Angeles, West-
3. Taylor AE, Saint-Cyr JA: Depression in Parkinson’s disease: recon- ern Psychological Services, 1973
ciling physiological and psychological perspectives. Journal of Neu- 19. Wechsler D: A standardized memory scale for clinical use. I Psychol
ropsychiatry and Clinical Neurosciences 1990; 2:92-98 1945; 19:87-95
4. Starkstein SE, Preziosi ‘IJ, Bolduc PL, et al: Depression in Parkinson’s 20. Santamaria J, Tolosa E, Valles A: Parkinson’s disease with depres-
disease. J Nerv Ment Dis 1990; 178:27-31 sion: a possible subgroup of idiopathic parkinsonism. Neurology
5. Canter GJ, De La Torre D, Mier M: A method for evaluating disabil- 1986; 36:1130-1133
ity in patients with Parkinson’s disease. J Neurol Neurosurg Psychi- 21. Starkstein SE, Berthier ML, Bolduc PL, et al: Depression in patients
atry 1961; 133:143-147 with early versus late onset of Parkinson’s disease. Neurology 1989;
6. Hoehn MM, Yahr MD: Parkinson’s disease: onset, progression and 39:1441-1445
mortality. Neurology 1967; 17:427-442 22. Starkstein SE, Preziosi TJ, Berthier ML, et al: Depression and cogni-
7. Robinson RG, Kubos KL, Starr LB. et al: Mood changes in stroke tive impairment in Parkinson’s disease. Brain 1989; 112:1141-1153
patients: relationship to lesion location. Compr Psychiatry 1983; 23. Starkstein SE, Bolduc PL, Mayberg HS, et al: Cognitive impairments
24:555-566 and depression in Parkinson’s disease: a follow-up study. I Neurol
8. American Psychiatric Association: Diagnostic and Statistical Man- Neurosurg Psychiatry 1990; 53:597-602
ual of Mental Disorders, 3rd edition. Washington, DC, American 24. Mayberg HS, Starkstein SE, Sadzot B, et al: Selective inferior frontal
Psychiatric Association, 1980 lobe hypometabolism in depressed patients with Parkinson’s dis-
9. Starkstein SE, Preziosi TI, Forrester AW, et al: Specificity of affective ease. Ann Neurol 1990; 28:57-64
and autonomic symptoms of depression in Parkinson’s disease. 25. Rogers D, Lees AJ, Smith E, et al: Bradyphrenia in Parkinson’s
Neurol Neurosurg Psychiatry 1990; 53:869-873 disease and psychomotor retardation in depressive illness: an exper-
10. Hamilton MA: A rating scale for depression. J Neurol Neurosurg imental study. Brain 1987; 110:761-776
Psychiatry 1960; 23:56-62 26. Wilson SAK: Neurology, vol 1. London, Arnold, 1940.
11. Hamilton MA: The assessment of anxiety states by rating. Br J Med 27. Mayeux R, Stern Y, Williams JBW, et a!: Clinical and biochemical
Psychol 1959; 32:50-55 features of depression in Parkinson’s disease. Am J Psychiatry 1986;
12. Starr LB, Robinson RG, Price TR: Reliability, validity, and clinical 143:756-759
utility of the social functioning exam in the assessment of stroke 28. Mayeux R, Stern Y, Sano M, et al: Clinical and biochemical correlates
patients. Exp Aging Res 1983; 9:101-106 of bradyphrenia in Parkinson’s disease. Neurology 1987; 37:1130-
13. Marin RS: Differential diagnosis and classification of apathy. Am 1134
Psychiatry 1990; 147:22-30 29. Rafal RD, Posner MI, Walker JA, et al: Cognition and the basal
14. Folstein MF, Folstein SE, McHugh PR: “Mini-Mental State”: a prac- ganglia. Brain 1984; 107:1083-1094
tical method for grading the cognitive state of patients for the 30. Cools AR, Van Den Bercken JHL, Horstinick MWI, et a!: Cognitive
clinician. J Psychiatr Res 1975; 12:189-198 and motor shifting aptitude disorder in Parkinson’s disease. J Neu-
15. Nelson HE: A modified card sorting test sensitive to frontal lobe rol Neurosurg Psychiatry 1984; 47:443-453
defects. Cortex 1976; 12:313-324
JOURNAL OF NEUROPSYCHIATRY 139
You might also like
- Akt Notes VtsDocument50 pagesAkt Notes VtsMin Maw100% (1)
- Diabetic Nephropathy BaruDocument24 pagesDiabetic Nephropathy BaruRobiyanti Nur Chalifah HattaNo ratings yet
- The Neuropsychiatry of Parkinson Disease: A Perfect Storm: SciencedirectDocument21 pagesThe Neuropsychiatry of Parkinson Disease: A Perfect Storm: SciencedirectroxanaNo ratings yet
- NIH Public Access: Delirium in Elderly PeopleDocument32 pagesNIH Public Access: Delirium in Elderly PeopleMonika Diaz KristyanindaNo ratings yet
- jnrp.jnrp_203_17 (2)Document2 pagesjnrp.jnrp_203_17 (2)yennyNo ratings yet
- Tab VS DFTDocument15 pagesTab VS DFTAntu NandaNo ratings yet
- Dementia Associated With Parkinson's Disease: ReviewDocument9 pagesDementia Associated With Parkinson's Disease: ReviewMónica ReisNo ratings yet
- Pluim Et Al. (2020) : Changes in Self and Informant Reported Frontal Behaviors in Parkinsons DiseaseDocument13 pagesPluim Et Al. (2020) : Changes in Self and Informant Reported Frontal Behaviors in Parkinsons DiseaseFie LarsenNo ratings yet
- Course of Psychiatric Symptoms and GlobalDocument8 pagesCourse of Psychiatric Symptoms and GloballoloasbNo ratings yet
- Service Users' Experiences of Receiving A Diagnosis of Borderline Personality Disorder: A Systematic ReviewDocument21 pagesService Users' Experiences of Receiving A Diagnosis of Borderline Personality Disorder: A Systematic ReviewMaria Jesus ZaldivarNo ratings yet
- Trastornos Bipolares y Depresivos MayoresDocument10 pagesTrastornos Bipolares y Depresivos MayoresDORIS JANETHNo ratings yet
- Arsland, 2010 Estudio Multicentrico Mil PacientesDocument8 pagesArsland, 2010 Estudio Multicentrico Mil PacientesRicardo Jose De LeonNo ratings yet
- Estudo. Espectro BipolarDocument9 pagesEstudo. Espectro BipolarGabriel LemosNo ratings yet
- Picion For Depression: Physical Examination For Brain InjuryDocument3 pagesPicion For Depression: Physical Examination For Brain InjuryShinohara YuusukeNo ratings yet
- Mds 21803Document7 pagesMds 21803Elisa FioraNo ratings yet
- Cohort Study On Somatoform Disorders in Parkinson Disease and Dementia With Lewy BodiesDocument9 pagesCohort Study On Somatoform Disorders in Parkinson Disease and Dementia With Lewy BodiesHelena AlessiNo ratings yet
- Anhedonia in Parkinson 'S Disease: An OverviewDocument8 pagesAnhedonia in Parkinson 'S Disease: An OverviewCitra AuraNo ratings yet
- Toys and Gadgets: Construct Validity of Apathy in Parkinson 'S DiseaseDocument9 pagesToys and Gadgets: Construct Validity of Apathy in Parkinson 'S DiseaseCitra AuraNo ratings yet
- Ranasinghe 2016Document12 pagesRanasinghe 2016Luciana CassimiroNo ratings yet
- Van Dijk 2014Document7 pagesVan Dijk 2014Nati Pardo PalenzuelaNo ratings yet
- giomi2021Document7 pagesgiomi20212010035No ratings yet
- Jamapsychiatry Lewis 2019 Oi 190089Document8 pagesJamapsychiatry Lewis 2019 Oi 190089Cristina PernasNo ratings yet
- Apatia y Riesdo de PDD CIDDocument15 pagesApatia y Riesdo de PDD CIDGustavo PestanaNo ratings yet
- A Case of Dissociative Identity Disorder and AttenDocument1 pageA Case of Dissociative Identity Disorder and AttenDoina MafteiuNo ratings yet
- Jamapsychiatry Devanand 2022 Oi 210088 1648226520.73569Document9 pagesJamapsychiatry Devanand 2022 Oi 210088 1648226520.73569Juan Carlos Perez ParadaNo ratings yet
- Nonmotor Symptoms of Parkinson's DiseaseDocument18 pagesNonmotor Symptoms of Parkinson's Diseaseelenac67No ratings yet
- AwalDocument5 pagesAwal0625Adinda Salsa AmiraNo ratings yet
- 15Document29 pages15yeremias setyawanNo ratings yet
- Specific and Generalized Neuropsychological DeficiDocument9 pagesSpecific and Generalized Neuropsychological DeficiDanielaNo ratings yet
- Evidence-Based Pharmacotherapy For Personality DisordersDocument32 pagesEvidence-Based Pharmacotherapy For Personality Disordersibn SalamaNo ratings yet
- Prevalence Obsessive Compulsive Disorder PatientsDocument6 pagesPrevalence Obsessive Compulsive Disorder PatientsKrasimir KostadinovNo ratings yet
- Torgersen 2001Document7 pagesTorgersen 2001Ekatterina DavilaNo ratings yet
- De Fining Atypical Anxiety in Parkinson's Disease: Clinical PracticeDocument11 pagesDe Fining Atypical Anxiety in Parkinson's Disease: Clinical PracticeketevanNo ratings yet
- 4-Treatment of Advanced Parkinson Ds - Continuum (2016)Document13 pages4-Treatment of Advanced Parkinson Ds - Continuum (2016)bernarduswidodoNo ratings yet
- BJP 42 05 503Document7 pagesBJP 42 05 503bssNo ratings yet
- Noc120108 580 586Document7 pagesNoc120108 580 586Henrique OliveiraNo ratings yet
- Apathy EvaluastionDocument12 pagesApathy EvaluastionDiana Cintia MgdalenaNo ratings yet
- Nonepileptic Seizures - An Updated ReviewDocument9 pagesNonepileptic Seizures - An Updated ReviewCecilia FRNo ratings yet
- PDpsychosisDocument8 pagesPDpsychosismyosotysNo ratings yet
- Miller Et Al. - 2016 - Cognitive Impairment in Older Adults With Epilepsy Characterization and Risk Factor AnalysisDocument5 pagesMiller Et Al. - 2016 - Cognitive Impairment in Older Adults With Epilepsy Characterization and Risk Factor Analysisconstanza BelénNo ratings yet
- Parkinsonism and Related DisordersDocument6 pagesParkinsonism and Related DisordersJose Alonso Aguilar ValeraNo ratings yet
- Massman, 1992 Cortical y SubcorticalDocument21 pagesMassman, 1992 Cortical y SubcorticalRicardo Jose De LeonNo ratings yet
- 2018 Transdiagnostic vs. Disorder-Focused Perspective in Children and Adolescents With Eating DisordersDocument13 pages2018 Transdiagnostic vs. Disorder-Focused Perspective in Children and Adolescents With Eating DisordersDiego HormacheaNo ratings yet
- Epidemiology of Psychotic Depression - Systematic Review and Meta-AnalysisDocument14 pagesEpidemiology of Psychotic Depression - Systematic Review and Meta-AnalysisVIA RUSTIANINo ratings yet
- Relation Between Clinical and Social Variables and Duration of Untreated Psychosis in First Episode PsychosisDocument7 pagesRelation Between Clinical and Social Variables and Duration of Untreated Psychosis in First Episode Psychosisgion.nandNo ratings yet
- Cognitive-Behavioural Features of Progressive Supranuclear Palsy Syndrome Overlap With Frontotemporal DementiaDocument7 pagesCognitive-Behavioural Features of Progressive Supranuclear Palsy Syndrome Overlap With Frontotemporal DementiaAlexandra CastellanosNo ratings yet
- HHS Public Access: Mistrustful and Misunderstood: A Review of Paranoid Personality DisorderDocument28 pagesHHS Public Access: Mistrustful and Misunderstood: A Review of Paranoid Personality DisorderLolitha JuliawandaniNo ratings yet
- Rosso Intervención 2020Document9 pagesRosso Intervención 2020Par DoNo ratings yet
- JNeurosciRuralPract6165-7834297 214542Document12 pagesJNeurosciRuralPract6165-7834297 214542Edu SajquimNo ratings yet
- Classification and Pathology of Primary Progressive AphasiaDocument8 pagesClassification and Pathology of Primary Progressive AphasiaDranmar AhmedNo ratings yet
- Jamainternal Van Vliet 2021 Oi 210051 1635441073.72519Document11 pagesJamainternal Van Vliet 2021 Oi 210051 1635441073.725192pr6ztzzbwNo ratings yet
- CH 42Document13 pagesCH 42HaleyNo ratings yet
- 1 s2.0 S1059131119305783 MainDocument8 pages1 s2.0 S1059131119305783 MainHappy PramandaNo ratings yet
- Depersonalization Disorder and Anxiety - A Special RelationshipDocument5 pagesDepersonalization Disorder and Anxiety - A Special RelationshipΙωάννης ΠαπαδόπουλοςNo ratings yet
- The Neurobiology of 2018Document18 pagesThe Neurobiology of 2018Dhino Armand Quispe SánchezNo ratings yet
- Aphaty and Its Impact On Carer Burden and Pychological Wellbeing in Primary Progressive AphasiaDocument6 pagesAphaty and Its Impact On Carer Burden and Pychological Wellbeing in Primary Progressive AphasiaFrancisca Cid BelmarNo ratings yet
- Aggression and Violent Behavior: SciencedirectDocument21 pagesAggression and Violent Behavior: SciencedirectMónika MikeNo ratings yet
- Psychosis in Autism: Comparison of The Features of Both Conditions in A Dually Affected CohortDocument12 pagesPsychosis in Autism: Comparison of The Features of Both Conditions in A Dually Affected Cohortrais123No ratings yet
- Nihms 941439Document14 pagesNihms 941439risma dwiyantiNo ratings yet
- Surgical Therapies For Parkinson DiseaseDocument13 pagesSurgical Therapies For Parkinson DiseaseAnali Durán CorderoNo ratings yet
- Lewy Body DementiaDocument20 pagesLewy Body DementiaAbdul SadiqNo ratings yet
- Fast Facts: Psychosis in Parkinson's Disease: Finding the right therapeutic balanceFrom EverandFast Facts: Psychosis in Parkinson's Disease: Finding the right therapeutic balanceNo ratings yet
- Pembrokeshire County Living Summer 2014Document57 pagesPembrokeshire County Living Summer 2014Digital MediaNo ratings yet
- Lesson 01Document6 pagesLesson 01Anonymous tfy40ZOoTNo ratings yet
- Key Resources For Psychiatric LibrariesDocument12 pagesKey Resources For Psychiatric LibrariesKaram Ali ShahNo ratings yet
- Iris Conjugation PEGYLATIONDocument8 pagesIris Conjugation PEGYLATIONidownloadbooks3133No ratings yet
- Regulations For The Degree of Master of Medical Sciences (Mmedsc)Document30 pagesRegulations For The Degree of Master of Medical Sciences (Mmedsc)Shuaib100% (1)
- Staph Infection & HIV (GP B1)Document48 pagesStaph Infection & HIV (GP B1)Jared Khoo Er HauNo ratings yet
- Imple Remedies (Totkas) For Success, Growth and ProsperityDocument5 pagesImple Remedies (Totkas) For Success, Growth and ProsperityDmmi Fzco100% (3)
- Theories of AgingDocument4 pagesTheories of AgingEmkhei Gonzales100% (2)
- Nishant Respiratory SecondDocument10 pagesNishant Respiratory SecondNishantNo ratings yet
- My Wellness Book: Jesica CerdaDocument21 pagesMy Wellness Book: Jesica CerdaJamie PetersonNo ratings yet
- 1Document24 pages1mhsupriNo ratings yet
- Full Ebook of Small Animal Soft Tissue Surgery 2Nd 2Nd Edition Eric Monnet Ed Online PDF All ChapterDocument69 pagesFull Ebook of Small Animal Soft Tissue Surgery 2Nd 2Nd Edition Eric Monnet Ed Online PDF All Chapterdeborahconlon906057100% (5)
- Basic First Aid For Medical EmergenciesDocument43 pagesBasic First Aid For Medical EmergenciesGissele AbolucionNo ratings yet
- MurmursDocument10 pagesMurmursAlina KievskyNo ratings yet
- Anatomy of The Endocrine System IIDocument129 pagesAnatomy of The Endocrine System IIShauie CayabyabNo ratings yet
- Table of Specification in 1GEN BIO 1STDocument3 pagesTable of Specification in 1GEN BIO 1STLouie DenostaNo ratings yet
- Hindko. Likhtaan Magazine 1.Document64 pagesHindko. Likhtaan Magazine 1.Near N DearNo ratings yet
- Drug Educ Long Term Effects of AlcoholDocument7 pagesDrug Educ Long Term Effects of Alcoholmary rose ombrogNo ratings yet
- Subcortical Ischemic Vascular Dementia: Helena C. Chui, MDDocument24 pagesSubcortical Ischemic Vascular Dementia: Helena C. Chui, MDEugenia FiginiNo ratings yet
- Aromat 1Document4 pagesAromat 1ManoharChintaNo ratings yet
- PostureDocument2 pagesPostureNader MorrisNo ratings yet
- MicroalbuminuriaDocument74 pagesMicroalbuminuriaMohamed AlaminNo ratings yet
- 2020 Focused Transesophageal Echocardiography During Cardiac Arrest ResuscitationDocument10 pages2020 Focused Transesophageal Echocardiography During Cardiac Arrest Resuscitationbogeg74816No ratings yet
- All India Institute of Medical Sciences Jodhpur College of Nursing Practice TeachingDocument11 pagesAll India Institute of Medical Sciences Jodhpur College of Nursing Practice Teachingmaneesh senNo ratings yet
- Blastocystis SPDocument10 pagesBlastocystis SPAhmad ShaukyNo ratings yet
- BEmONC - Facilitator's Handbook - 2013 April - FinalDocument286 pagesBEmONC - Facilitator's Handbook - 2013 April - FinalElizabeth Nionzima100% (2)
- Anatomy of Hepatobiliary SystemDocument46 pagesAnatomy of Hepatobiliary SystemAyu Tiara FitriNo ratings yet
- Presbycusis: J. R. Kearns, MDDocument5 pagesPresbycusis: J. R. Kearns, MDnick_mdNo ratings yet