Download as pdf or txt
You might also like
- Freud Bose CorrespondenceDocument17 pagesFreud Bose CorrespondenceSiddhi JangidNo ratings yet
- Kris Gethin Shred-KM-4WRK2LEAN-FINAL PDFDocument57 pagesKris Gethin Shred-KM-4WRK2LEAN-FINAL PDFSarmad Sultan67% (3)
- Diagnosis and Management of PrediabetesDocument11 pagesDiagnosis and Management of PrediabetesNadir MonteroNo ratings yet
- Glycemic Targets Standards of Care in Diabetes-2023Document14 pagesGlycemic Targets Standards of Care in Diabetes-2023ÁngelesNo ratings yet
- Reading: Healthy Lifestyle Role For All Society'Document4 pagesReading: Healthy Lifestyle Role For All Society'Tore CusimanoNo ratings yet
- Ebin Belderol TB and WorksheetDocument11 pagesEbin Belderol TB and WorksheetMarielle Ebin100% (3)
- Standards of Care in Diabetes - 2023: 6. Glycemic TargetsDocument14 pagesStandards of Care in Diabetes - 2023: 6. Glycemic TargetsMenethil Terenas ElijiahNo ratings yet
- Effect of Semaglutide and Liraglutide in Individuals With Obesity or Overweight Without Diabetes-A Systematic ReviewDocument14 pagesEffect of Semaglutide and Liraglutide in Individuals With Obesity or Overweight Without Diabetes-A Systematic ReviewNewtonRibeiroNo ratings yet
- Clinical Pharmacy Therapeu - 2022 - Phillips - Clinical Review of Subcutaneous Semaglutide For ObesityDocument10 pagesClinical Pharmacy Therapeu - 2022 - Phillips - Clinical Review of Subcutaneous Semaglutide For ObesityArtyy ArtyyNo ratings yet
- Clinical Review of Subcutaneous Semaglutide For ObesityDocument10 pagesClinical Review of Subcutaneous Semaglutide For ObesityGhygggNo ratings yet
- 212 812 1 PBDocument6 pages212 812 1 PBnindi jemmyNo ratings yet
- 3 DMDocument8 pages3 DMAna MaríaNo ratings yet
- Prevention or Delay of Type 2Document8 pagesPrevention or Delay of Type 2Paulina CuevaNo ratings yet
- ADA DiabetesDocument8 pagesADA DiabetesMaria MagdalenaNo ratings yet
- Standards of Care in Diabetes - 2023Document12 pagesStandards of Care in Diabetes - 2023Menethil Terenas ElijiahNo ratings yet
- ระบาด3-mainDocument6 pagesระบาด3-mainArkaNay PraPanNo ratings yet
- Do Toe Blood Pressures Predict Healing After Minor Lower Limb Amputation in People With Diabetes? A Systematic Review and Meta-AnalysisDocument10 pagesDo Toe Blood Pressures Predict Healing After Minor Lower Limb Amputation in People With Diabetes? A Systematic Review and Meta-AnalysisNathaniel Gilbert DysonNo ratings yet
- Efficacy of Value Added Foxtail Millet Therapeutic Food in The Management of Diabetes and Dyslipidamea in Type 2 Diabetic PatientsDocument3 pagesEfficacy of Value Added Foxtail Millet Therapeutic Food in The Management of Diabetes and Dyslipidamea in Type 2 Diabetic PatientsFauziah AmrullahNo ratings yet
- Effect of Eating Even or Odd Number of Dates, On Blood Glucose LevelDocument5 pagesEffect of Eating Even or Odd Number of Dates, On Blood Glucose LevelAlaaGaballaNo ratings yet
- Guideline Perkeni 2019 - 4Document36 pagesGuideline Perkeni 2019 - 4jktrlsNo ratings yet
- Nutrition Therapy For Diabetes Effectiveness Carbohydrates and AlcoholDocument12 pagesNutrition Therapy For Diabetes Effectiveness Carbohydrates and Alcoholscience lulNo ratings yet
- Diabetes and Clinical Research: ClinmedDocument4 pagesDiabetes and Clinical Research: ClinmedHerybert KiiNo ratings yet
- JDM 2017110814284359Document8 pagesJDM 2017110814284359Mochamad BilalNo ratings yet
- Artikel Bu RashnahDocument7 pagesArtikel Bu RashnahSitti Rosdiana YahyaNo ratings yet
- Analysis of Balance Dysfuntion and Fall PDFDocument6 pagesAnalysis of Balance Dysfuntion and Fall PDFJulenda CintarinovaNo ratings yet
- 5 Assessment of KnowledgeDocument14 pages5 Assessment of KnowledgeNejash Abdo IssaNo ratings yet
- Prevencion DM 2023Document8 pagesPrevencion DM 2023Samuel CaballeroNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument5 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsRizaldi FirdausNo ratings yet
- Obesity and WeightDocument12 pagesObesity and WeightMarianaNo ratings yet
- Tan, 2022Document8 pagesTan, 2022Mirilláiny AnacletoNo ratings yet
- A Study To Assess The Effectiveness of Yoga On HbA1C Level Among Patients With Type 2 Diabetes MellitusDocument5 pagesA Study To Assess The Effectiveness of Yoga On HbA1C Level Among Patients With Type 2 Diabetes MellitusEditor IJTSRDNo ratings yet
- Journal of Applied Health Management and TechnologyDocument12 pagesJournal of Applied Health Management and TechnologyMhd Azland FikryNo ratings yet
- 1 s2.0 S2212267224001928 MainDocument9 pages1 s2.0 S2212267224001928 MainYULISSA FLORES RONDONNo ratings yet
- FCDHC 02 823046Document16 pagesFCDHC 02 823046ezazpsychologistNo ratings yet
- S32 Full PDFDocument5 pagesS32 Full PDFCarolina MibielliNo ratings yet
- Fracture Healing in Elderly Distal Radius Fracture With Type II Diabetes MellitusDocument7 pagesFracture Healing in Elderly Distal Radius Fracture With Type II Diabetes MellitusAthenaeum Scientific PublishersNo ratings yet
- Diabetes and Clinical ResearchDocument7 pagesDiabetes and Clinical ResearchAde PahrunNo ratings yet
- Diabetes Care 2018Document8 pagesDiabetes Care 2018Febryan Leonardo GultomNo ratings yet
- 823 FullDocument5 pages823 FullPencari IlmuNo ratings yet
- Jama Echouffotcheugui 2023 RV 230007 1680895578.04302Document11 pagesJama Echouffotcheugui 2023 RV 230007 1680895578.04302Buton InspirasiNo ratings yet
- Pathiraja Wijebandara-ExperienceDocument48 pagesPathiraja Wijebandara-ExperienceTengku EltrikanawatiNo ratings yet
- 05 Iajps05062017Document6 pages05 Iajps05062017Baru Chandrasekhar RaoNo ratings yet
- A Study To Determine The Quality of Life and To Assess The Effectiveness of Nurse Directed Intervention in Knowledge and Health Promotion Behavior of Type 2 Diabetes Mellitus Among Ubran AreaDocument5 pagesA Study To Determine The Quality of Life and To Assess The Effectiveness of Nurse Directed Intervention in Knowledge and Health Promotion Behavior of Type 2 Diabetes Mellitus Among Ubran AreaEditor IJTSRDNo ratings yet
- Journal Ke 5Document5 pagesJournal Ke 5StrangersNo ratings yet
- Prolanis Implementation Effective To Control Fasting Blood Sugar, Hba1C and Total Cholesterol Levels in Patients With Type 2 DiabetesDocument12 pagesProlanis Implementation Effective To Control Fasting Blood Sugar, Hba1C and Total Cholesterol Levels in Patients With Type 2 Diabetesindah sundariNo ratings yet
- A Review of Nutrition and Dietary Interventions in OncologyDocument16 pagesA Review of Nutrition and Dietary Interventions in OncologyAgustin LopezNo ratings yet
- Study of Some Biochemical Parameters For Patients Withtype II Diabetes Mellitus in Al Rifai DistrictDocument8 pagesStudy of Some Biochemical Parameters For Patients Withtype II Diabetes Mellitus in Al Rifai DistrictCentral Asian StudiesNo ratings yet
- Agra Wal 2007Document7 pagesAgra Wal 2007arib syedNo ratings yet
- Burger Allen ExercisesDocument6 pagesBurger Allen Exerciseslucky 116No ratings yet
- Consumption of Purple Sweet Potato Snack Bar and Self Help Group For Blood Glucose Levels in Patients Diabetes Mellitus Type 2Document7 pagesConsumption of Purple Sweet Potato Snack Bar and Self Help Group For Blood Glucose Levels in Patients Diabetes Mellitus Type 2International Journal of Innovative Science and Research TechnologyNo ratings yet
- Effectiveness For Self-Monitoring of Blood Sugar oDocument8 pagesEffectiveness For Self-Monitoring of Blood Sugar onico7christianNo ratings yet
- Standards of Care in Diabetes - 2024: 6. Glycemic Goals and HypoglycemiaDocument15 pagesStandards of Care in Diabetes - 2024: 6. Glycemic Goals and HypoglycemiaGustavo DelgadoNo ratings yet
- Membuat KuesionerDocument9 pagesMembuat KuesionerAGXfariNo ratings yet
- Adultos Mayores y DiabetesDocument14 pagesAdultos Mayores y DiabetesValentina GonzalezNo ratings yet
- HbA1C AS AN INDEX OF GLYCEMIC STATUS IN OBESE TYPE 2 DIABETICSDocument6 pagesHbA1C AS AN INDEX OF GLYCEMIC STATUS IN OBESE TYPE 2 DIABETICSInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Treatment of Type 2 Diabetes: From "Guidelines" To "Position Statements" and BackDocument8 pagesTreatment of Type 2 Diabetes: From "Guidelines" To "Position Statements" and BackgabbynengNo ratings yet
- Guideline Perkeni 2019 PDFDocument36 pagesGuideline Perkeni 2019 PDFCut Aulia MaulizaNo ratings yet
- Assessing Gap in Food Habits of Diabetic Population in Field Practice Areas of Kims HubballiDocument12 pagesAssessing Gap in Food Habits of Diabetic Population in Field Practice Areas of Kims HubballiInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S1319562X21010007 MainDocument5 pages1 s2.0 S1319562X21010007 MainmerlinakisNo ratings yet
- PrediabetesDocument11 pagesPrediabetesAna MayNo ratings yet
- Effect of Vitamin C On Blood Glucose, Serum Lipids & Serum Insulin in Type 2 Diabetes PatientsDocument5 pagesEffect of Vitamin C On Blood Glucose, Serum Lipids & Serum Insulin in Type 2 Diabetes Patientssahama2508No ratings yet
- Diabetes Reversal by Plant-Based Diet: January 2017Document9 pagesDiabetes Reversal by Plant-Based Diet: January 2017Srinivas ZannuNo ratings yet
- Semaglutide Unveiled: A Comprehensive Guide to Diabetes Treatment and Weight ManagementFrom EverandSemaglutide Unveiled: A Comprehensive Guide to Diabetes Treatment and Weight ManagementNo ratings yet
- Kelly 2001Document7 pagesKelly 2001senkonenNo ratings yet
- Journal EndoDocument13 pagesJournal EndosenkonenNo ratings yet
- JHM 2112Document4 pagesJHM 2112senkonenNo ratings yet
- Journal DoxoDocument8 pagesJournal DoxosenkonenNo ratings yet
- Guidline DVT HomDocument47 pagesGuidline DVT HomsenkonenNo ratings yet
- Pregnancy Outcomes in Familial Hypercholesterolemia: Epidemiology and PreventionDocument10 pagesPregnancy Outcomes in Familial Hypercholesterolemia: Epidemiology and PreventionsenkonenNo ratings yet
- Reference NHL ChopDocument4 pagesReference NHL ChopsenkonenNo ratings yet
- Penelitian Channa - RS Fatmawati - Final PDFDocument5 pagesPenelitian Channa - RS Fatmawati - Final PDFsenkonenNo ratings yet
- Cjog Aid1026Document11 pagesCjog Aid1026senkonenNo ratings yet
- 349 FullDocument3 pages349 FullsenkonenNo ratings yet
- Anticoagulation Resumption After Intracerebral HemorrhageDocument10 pagesAnticoagulation Resumption After Intracerebral HemorrhagesenkonenNo ratings yet
- Fitzgerald 2019Document10 pagesFitzgerald 2019senkonenNo ratings yet
- Doxorubicin, Mesenchymal Stem Cell Toxicity and Antitumour Activity: Implications For Clinical UseDocument8 pagesDoxorubicin, Mesenchymal Stem Cell Toxicity and Antitumour Activity: Implications For Clinical UsesenkonenNo ratings yet
- Reference - Obat Ca Ma PDFDocument4 pagesReference - Obat Ca Ma PDFsenkonenNo ratings yet
- Reduced Lower-Limb Muscle Strength and Volume in Patients With Type 2 Diabetes in Relation To Neuropathy, Intramuscular Fat, and Vitamin D LevelsDocument7 pagesReduced Lower-Limb Muscle Strength and Volume in Patients With Type 2 Diabetes in Relation To Neuropathy, Intramuscular Fat, and Vitamin D LevelssenkonenNo ratings yet
- Management of Chronic Diabetic Foot Ulcers Using Platelet-Rich PlasmaDocument4 pagesManagement of Chronic Diabetic Foot Ulcers Using Platelet-Rich PlasmasenkonenNo ratings yet
- Keeling 2019Document8 pagesKeeling 2019senkonenNo ratings yet
- Cognitive Dysfunction: Part and Parcel of The Diabetic FootDocument6 pagesCognitive Dysfunction: Part and Parcel of The Diabetic FootsenkonenNo ratings yet
- Accepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument10 pagesAccepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewssenkonenNo ratings yet
- α polymorphisms in Platelet Rich-Plasma (PRP)Document3 pagesα polymorphisms in Platelet Rich-Plasma (PRP)senkonenNo ratings yet
- 391 FullDocument7 pages391 FullsenkonenNo ratings yet
- 10MJMS26012019 Oa7Document8 pages10MJMS26012019 Oa7senkonenNo ratings yet
- OutbreakWksht UpdatedMay18 ADocument3 pagesOutbreakWksht UpdatedMay18 ASatya DwiparthaNo ratings yet
- SDM-v1 0Document32 pagesSDM-v1 0Franz NussmannNo ratings yet
- Sales Case Digest Assignment-2CDocument7 pagesSales Case Digest Assignment-2CVox PopuliNo ratings yet
- ISC BiotechnologyDocument6 pagesISC BiotechnologySamikshaNo ratings yet
- Combined Cellulitis - FinalDocument78 pagesCombined Cellulitis - Finalsaru_patel0% (1)
- Internet of Things Applications: Current and Future DevelopmentDocument34 pagesInternet of Things Applications: Current and Future DevelopmentNithinNo ratings yet
- 27-07-2021 HMB EnglishDocument12 pages27-07-2021 HMB EnglishGyan PrakashNo ratings yet
- Naphthenic Acid / Naphthenate Stabilized Emulsions and The Influence of Crude Oil ComponentsDocument1 pageNaphthenic Acid / Naphthenate Stabilized Emulsions and The Influence of Crude Oil ComponentsLuis Alberto ChirinosNo ratings yet
- Liabilities and EquityDocument23 pagesLiabilities and Equityadmiral spongebobNo ratings yet
- What Are The Expected Tasks You Have Successfully AccomplishedDocument1 pageWhat Are The Expected Tasks You Have Successfully AccomplishedImmortality Realm67% (18)
- Ron Arwin Nathaniel G. Palmares 10 - PAscal EngDocument7 pagesRon Arwin Nathaniel G. Palmares 10 - PAscal Engron arwin nathaniel palmaresNo ratings yet
- Genetics and EugenicsDocument518 pagesGenetics and EugenicsTapuwa ChizunzaNo ratings yet
- Luserne Tree InformationDocument26 pagesLuserne Tree Informationpierre van wykNo ratings yet
- Exercise 1. You Have Been Given A Form Which Shows The Details of Technical Jobs Carried OutDocument2 pagesExercise 1. You Have Been Given A Form Which Shows The Details of Technical Jobs Carried OutNgo Gia Huy (K15 HCM)No ratings yet
- Sample ReviewDocument5 pagesSample Reviewdawit gebreyohansNo ratings yet
- Prime MX FIRA 6250 2018Document4 pagesPrime MX FIRA 6250 2018hodlab designcoNo ratings yet
- Certificate of Compliance CSA For Fluke 113 - 114 - 115-116-117Document2 pagesCertificate of Compliance CSA For Fluke 113 - 114 - 115-116-117CHARLES BARRAZA100% (1)
- DRRR2324 Q4 DRRDocument7 pagesDRRR2324 Q4 DRRh4gtg7n55gNo ratings yet
- Caring For Your African American/Biracial Child's HairDocument32 pagesCaring For Your African American/Biracial Child's Hair4kidslikemeNo ratings yet
- Activity 1: Measuring The Volume of Irregularly Shaped ObjectsDocument4 pagesActivity 1: Measuring The Volume of Irregularly Shaped ObjectsBamPanggatNo ratings yet
- MIL-I-17563C - Impregnation StdsDocument18 pagesMIL-I-17563C - Impregnation StdsMohanrajMJNo ratings yet
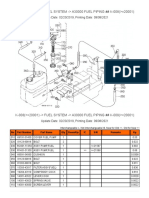
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- SZ Sales ProgramDocument28 pagesSZ Sales ProgramrossifrancescoNo ratings yet
- Basic Facts About ESOPs2Document20 pagesBasic Facts About ESOPs2Quant TradingNo ratings yet
- 2-BP-3.5K-5K 220v ManualDocument42 pages2-BP-3.5K-5K 220v ManualEcosenseTechnologies GreenenergyNo ratings yet
- Orthopaedic Study Guide 2014Document126 pagesOrthopaedic Study Guide 2014Yip Kar Jun100% (1)