Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- School Health NursingDocument11 pagesSchool Health NursingCeelin Robles100% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- IEC 60950 Rev1Document3 pagesIEC 60950 Rev1Rip_BarNo ratings yet
- Introduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesDocument8 pagesIntroduction To Fluorescence Techniques: Fluorophores and Their Amine-Reactive DerivativesManoj Kumar ChaurasiaNo ratings yet
- Nebosh Igc 2Document27 pagesNebosh Igc 2narendra16118890% (40)
- Prelim ExamDocument17 pagesPrelim Examsaci PTNo ratings yet
- Infectious Disease Naplex QuestionsDocument3 pagesInfectious Disease Naplex QuestionsSARANYA0% (1)
- Gantt ChartDocument2 pagesGantt ChartCeelin RoblesNo ratings yet
- Personal Protective EquipmentDocument3 pagesPersonal Protective EquipmentCeelin RoblesNo ratings yet
- Diarrhea Drug StudyDocument12 pagesDiarrhea Drug StudyCeelin Robles0% (1)
- Universidad de Manila: (Formerly City College of Manila) Mehan Garden, ManilaDocument24 pagesUniversidad de Manila: (Formerly City College of Manila) Mehan Garden, ManilaCeelin RoblesNo ratings yet
- COM FinalDocument10 pagesCOM FinalCeelin RoblesNo ratings yet
- School Health Nursing - COPARDocument33 pagesSchool Health Nursing - COPARCeelin Robles50% (2)
- Function of Endocrine SystemDocument7 pagesFunction of Endocrine SystemCeelin RoblesNo ratings yet
- Drug Name Dosage Mechanism of Action Specific Interactions Contraindications and Cautions Adverse Reaction Nursing ConsiderationsDocument4 pagesDrug Name Dosage Mechanism of Action Specific Interactions Contraindications and Cautions Adverse Reaction Nursing ConsiderationsCeelin RoblesNo ratings yet
- Long Quiz Earth Sci 11Document2 pagesLong Quiz Earth Sci 11Jesha mae MagnoNo ratings yet
- Codes Standards RegulationsDocument11 pagesCodes Standards RegulationsEslNo ratings yet
- OlanzapineDocument1 pageOlanzapineKallie ChartrandNo ratings yet
- SPS Plans PDFDocument7 pagesSPS Plans PDFSalin ShresthaNo ratings yet
- Welding Procedure Specification Joint Venture: Azzawiya Control System Modernization ProjectDocument4 pagesWelding Procedure Specification Joint Venture: Azzawiya Control System Modernization ProjectwentropremNo ratings yet
- 04 - Protection GeneralDocument52 pages04 - Protection GeneralRK KNo ratings yet
- Background of The StudyDocument13 pagesBackground of The Studyjeffrey rodriguezNo ratings yet
- MPT ProjectDocument10 pagesMPT ProjectTina SanghaviNo ratings yet
- Learning Activity Sheet Electronics G10 Q3 W1Document5 pagesLearning Activity Sheet Electronics G10 Q3 W1Mark Anthony Discarga JetajobeNo ratings yet
- India Bulls Housing Finance LimitedDocument67 pagesIndia Bulls Housing Finance LimitedslohariNo ratings yet
- Microbiology 101: Laboratory Exercise #22: Carbohydrate MetabolismDocument16 pagesMicrobiology 101: Laboratory Exercise #22: Carbohydrate Metabolismmaraki998No ratings yet
- Obat Kausatif Infeksi: 6ggpo, 0shqwlget Grad Corporis Ult Hui Form 3DDocument5 pagesObat Kausatif Infeksi: 6ggpo, 0shqwlget Grad Corporis Ult Hui Form 3DMaulana Malik IbrahimNo ratings yet
- American FoodDocument10 pagesAmerican FoodEvan BanksNo ratings yet
- Chicken BellagioDocument4 pagesChicken BellagioJagr MaddoxNo ratings yet
- Natural Rubber WikiDocument9 pagesNatural Rubber WikiMyra Wardati SNo ratings yet
- 2nd Quarter PHILO ReviewerDocument1 page2nd Quarter PHILO ReviewerTrisha Joy Dela Cruz80% (5)
- II 2015 4Document283 pagesII 2015 4tuni santeNo ratings yet
- Altitude, Cloud Cover and LatitudeDocument64 pagesAltitude, Cloud Cover and LatitudeIsarra AmsaluNo ratings yet
- Carbon & Its CompoundDocument13 pagesCarbon & Its CompoundNeeraj PoddarNo ratings yet
- Mina NEGRA HUANUSHA 2 ParteDocument23 pagesMina NEGRA HUANUSHA 2 ParteRoberto VillegasNo ratings yet
- 793-P-1C Relay Data SheetDocument6 pages793-P-1C Relay Data SheetsendmebooksNo ratings yet
- Board Question Paper - March 2023 - For Reprint Update - 641b040f4992cDocument4 pagesBoard Question Paper - March 2023 - For Reprint Update - 641b040f4992cSushan BhagatNo ratings yet
- Blue Bead McqsDocument11 pagesBlue Bead Mcqsanu minochaNo ratings yet
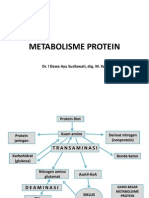
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- OSH SeminarDocument2 pagesOSH SeminarSahar Ulu JeruasNo ratings yet