
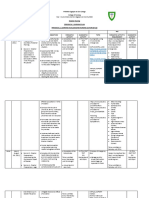
Personal Data of Patient: Intensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 5: Pediatric Oncology
Personal Data of Patient: Intensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 5: Pediatric Oncology
You might also like
- Acute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsromelynNo ratings yet
- CASE3Document5 pagesCASE3romelynNo ratings yet
- Hygiene (NCLEX) Flashcards - QuizletDocument5 pagesHygiene (NCLEX) Flashcards - QuizletA.No ratings yet
- SOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticDocument5 pagesSOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticvidyahamzahNo ratings yet
- PnclexDocument3 pagesPnclexPaul Michael BaguhinNo ratings yet
- HIV Practice TestDocument2 pagesHIV Practice TestJoslyn GrossNo ratings yet
- Complete Question Bank - Entrepreneurship DevelopmentDocument3 pagesComplete Question Bank - Entrepreneurship DevelopmentUday Gowda100% (1)
- Columbus - Hero or VillainDocument4 pagesColumbus - Hero or Villainapi-264258719No ratings yet
- OB2 - Renal and Urinary Tract Disorders in Pregnancy - Dr. TanDocument6 pagesOB2 - Renal and Urinary Tract Disorders in Pregnancy - Dr. TanHazel Fernandez VillarNo ratings yet
- Initiating A Blood TransfusionDocument5 pagesInitiating A Blood TransfusionJoyce Kathreen Ebio LopezNo ratings yet
- NCP (Burn)Document2 pagesNCP (Burn)Maricel R. ManabatNo ratings yet
- Disaster Nursing P1 Learning PlanDocument5 pagesDisaster Nursing P1 Learning PlanPamela GastalaNo ratings yet
- Cavite State University: I. ObjectivesDocument7 pagesCavite State University: I. ObjectivesChamy CruzNo ratings yet
- CIP-NCM-121-Disaster Nursing-TuesdaysDocument3 pagesCIP-NCM-121-Disaster Nursing-TuesdaysKhen QuiringNo ratings yet
- Foreigh Body Airway Obstruction Management July 2019Document1 pageForeigh Body Airway Obstruction Management July 2019Feliros S. SanciangcoNo ratings yet
- Course Specification Emergency NursingDocument6 pagesCourse Specification Emergency NursingWael LotfyNo ratings yet
- Congruent Care, Which Is The Primary Goal of TransculturalDocument3 pagesCongruent Care, Which Is The Primary Goal of TransculturalPrince SoletaNo ratings yet
- WK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TideDocument43 pagesWK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TidePotato PceeNo ratings yet
- Maternal and Child Health Nursing: KeepsDocument32 pagesMaternal and Child Health Nursing: Keepsshenric16No ratings yet
- Sexually Transmitted InfectionsDocument34 pagesSexually Transmitted InfectionsMariana Creciun100% (1)
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaNo ratings yet
- 08 At-Risk or High-Risk Sick NewbornDocument17 pages08 At-Risk or High-Risk Sick NewbornJAN CAMILLE LENONNo ratings yet
- TLG IV TherapyDocument10 pagesTLG IV TherapyStephanie Joy EscalaNo ratings yet
- AMOEBIASISDocument8 pagesAMOEBIASISCheska ت HortelanoNo ratings yet
- Performing Heimlich ManeuverDocument5 pagesPerforming Heimlich ManeuverAngelie PantajoNo ratings yet
- Submitted By: Bsn-Iv A Submitted To: Clinical Instructor: Cabatbat, Wyen CDocument5 pagesSubmitted By: Bsn-Iv A Submitted To: Clinical Instructor: Cabatbat, Wyen CWyen CabatbatNo ratings yet
- NCM 107 - RleDocument23 pagesNCM 107 - RleMaxinne Allyssa Cancino RoseñoNo ratings yet
- NCM 109 Rle ClinicalDocument20 pagesNCM 109 Rle ClinicalBiway RegalaNo ratings yet
- Competency Appraisal 1Document30 pagesCompetency Appraisal 1mirai desuNo ratings yet
- Making An Occupied BedDocument2 pagesMaking An Occupied BedAnonymous h2EnKyDb100% (1)
- Cesarean Section: Yusef C. Wibowo, S.ST.,M.HDocument6 pagesCesarean Section: Yusef C. Wibowo, S.ST.,M.HberlyanaNo ratings yet
- Mosquito Borne DiseasesDocument31 pagesMosquito Borne DiseasesRizna SaidNo ratings yet
- Teaching Plan 2Document10 pagesTeaching Plan 2Terma JamiriNo ratings yet
- Linear Arrangements of DR InstrumentsDocument42 pagesLinear Arrangements of DR Instrumentsxxegyzz100% (1)
- Naso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringDocument12 pagesNaso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringmeisygraniaNo ratings yet
- Availability and Utilization of Health Informatics System Among Health Workers in Niger State, NigeriaDocument8 pagesAvailability and Utilization of Health Informatics System Among Health Workers in Niger State, NigeriaEditor IJTSRDNo ratings yet
- Expanded Program On ImmunizationDocument23 pagesExpanded Program On ImmunizationKate E. GatchalianNo ratings yet
- Incontinence Case StudyDocument26 pagesIncontinence Case StudyRose AnnNo ratings yet
- NCM 118 - Lesson 7 (Pneumothorax)Document4 pagesNCM 118 - Lesson 7 (Pneumothorax)Bobby Christian DuronNo ratings yet
- Vaccination or ImmunizationDocument4 pagesVaccination or ImmunizationPrincessNo ratings yet
- In The Name of Allah, The Most Beneficent and MercifulDocument35 pagesIn The Name of Allah, The Most Beneficent and MercifulAhmedMenshawyNo ratings yet
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoNo ratings yet
- Health Assessment IntroductionDocument50 pagesHealth Assessment IntroductionEdna Uneta RoblesNo ratings yet
- 10 Golden Rules of IV TherapyDocument8 pages10 Golden Rules of IV Therapybbasya eihynaNo ratings yet
- Administering Pulse OxDocument2 pagesAdministering Pulse OxjepoiNo ratings yet
- Demo Teaching Physical Health AssessmentDocument5 pagesDemo Teaching Physical Health AssessmentJulie May SuganobNo ratings yet
- Emergency Department FlowchartDocument2 pagesEmergency Department FlowchartRaqz LopezNo ratings yet
- 2nd Sem NSG Lec NotesDocument105 pages2nd Sem NSG Lec NotesJan Crizza Dale R. FrancoNo ratings yet
- Hematologic ManagementDocument17 pagesHematologic ManagementAlyssa MontimorNo ratings yet
- Reflective Journal NCM 107 SKL (NIEGAS)Document1 pageReflective Journal NCM 107 SKL (NIEGAS)Dominic GarciaNo ratings yet
- Intensive V (Complications)Document117 pagesIntensive V (Complications)darren55No ratings yet
- Rating Scale: 0 Omitted 1 Poorly Done 2 Fairly Done 3 Well Done Indicates Critical Step Omission or Poor Performance Equates To FailureDocument3 pagesRating Scale: 0 Omitted 1 Poorly Done 2 Fairly Done 3 Well Done Indicates Critical Step Omission or Poor Performance Equates To FailureTemahlungwane100% (2)
- Chikungunya FeverDocument15 pagesChikungunya FeverAyomide AlayandeNo ratings yet
- Prepared By: Sarah Diana Rise S. Manalili, RNDocument38 pagesPrepared By: Sarah Diana Rise S. Manalili, RNSARAH DIANA ROSE S. MANALILI100% (1)
- Journal Gadar Choking-Managing The Risk of Choking GuidelinesDocument18 pagesJournal Gadar Choking-Managing The Risk of Choking GuidelinesnurulNo ratings yet
- Intracranial SurgeryDocument12 pagesIntracranial SurgerysetanpikulanNo ratings yet
- Konsep Palliative Care Pada AnakDocument48 pagesKonsep Palliative Care Pada AnakDayu Dani100% (1)
- MeaslesDocument32 pagesMeaslesYum C100% (2)
- Diphtheria in NepalDocument30 pagesDiphtheria in NepalBinaya100% (1)
- A. Setting Up B. Inserting IV Utilizing The Dummy Arm C. Changing An IV Solution D. Discontinuing An IV InfusionDocument7 pagesA. Setting Up B. Inserting IV Utilizing The Dummy Arm C. Changing An IV Solution D. Discontinuing An IV InfusionJerika Shane MañosoNo ratings yet
- Conceptual Foundation and Critical Care NursingDocument41 pagesConceptual Foundation and Critical Care NursingAbdulNo ratings yet
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- NURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYFrom EverandNURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYNo ratings yet
- SF2 - 2019 - Grade 2 D ROSE FEBDocument3 pagesSF2 - 2019 - Grade 2 D ROSE FEBromelynNo ratings yet
- School Form 2 (SF2) Daily Attendance Report of Learners: X XX X X X XX X XDocument6 pagesSchool Form 2 (SF2) Daily Attendance Report of Learners: X XX X X X XX X XromelynNo ratings yet
- SF2 - 2019 - Grade 2 D ROSE APRILDocument3 pagesSF2 - 2019 - Grade 2 D ROSE APRILromelynNo ratings yet
- Output 3 - Family Health NursingDocument9 pagesOutput 3 - Family Health Nursingromelyn100% (1)
- Mary Jesrel J. Cudia BSN Ii-A: RightsDocument3 pagesMary Jesrel J. Cudia BSN Ii-A: RightsromelynNo ratings yet
- Output 3 - Family Health NursingDocument5 pagesOutput 3 - Family Health NursingromelynNo ratings yet
- Intensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 4: Pre - School (Respiratory System)Document5 pagesIntensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 4: Pre - School (Respiratory System)romelynNo ratings yet
- Inp 402.rubics - Case.anaDocument2 pagesInp 402.rubics - Case.anaromelyn0% (1)
- Nursing Care Plan (NCP) For Acute Lymphocytic LeukemiaDocument4 pagesNursing Care Plan (NCP) For Acute Lymphocytic LeukemiaromelynNo ratings yet
- NCP 2Document3 pagesNCP 2romelyn100% (1)
- Inp Rle Pedia Ward Case7Document1 pageInp Rle Pedia Ward Case7romelynNo ratings yet
- School Forms Checking Report (SFCR) : Table 1. Learners Record Examined/ReviewedDocument1 pageSchool Forms Checking Report (SFCR) : Table 1. Learners Record Examined/ReviewedromelynNo ratings yet
- NURSING HEALTH HISTORYup.Document5 pagesNURSING HEALTH HISTORYup.romelynNo ratings yet
- Preparing To Use A Nebulizer: 1 Wash Your HandsDocument4 pagesPreparing To Use A Nebulizer: 1 Wash Your HandsromelynNo ratings yet
- ESP A.P English MTB Math Filipino MAPEH (Art) : GRADES 1 To 12 Daily Lesson LogDocument9 pagesESP A.P English MTB Math Filipino MAPEH (Art) : GRADES 1 To 12 Daily Lesson LogromelynNo ratings yet
- Health History: I. Personal DataDocument7 pagesHealth History: I. Personal DataromelynNo ratings yet
- Sf2 - 2019 - Grade 2 - D - Rose (June)Document1 pageSf2 - 2019 - Grade 2 - D - Rose (June)romelynNo ratings yet
- PhillipDocument4 pagesPhilliplucasdoriamaiaNo ratings yet
- 21 Days Prayer Fasting RiversideDocument5 pages21 Days Prayer Fasting RiversideAnaPereiraNo ratings yet
- When To Salute - Military Protocol Guide To Showing RespectDocument20 pagesWhen To Salute - Military Protocol Guide To Showing RespectGreg JohnsonNo ratings yet
- Work Function: Applications MeasurementDocument10 pagesWork Function: Applications MeasurementshiravandNo ratings yet
- Ancient Athens Brochure Assignment and RubricDocument2 pagesAncient Athens Brochure Assignment and Rubricapi-297382264No ratings yet
- LiberalismDocument3 pagesLiberalismNafis FuadNo ratings yet
- Drimzo Oil Interview FormDocument2 pagesDrimzo Oil Interview Formdmita9276No ratings yet
- A Project Report ON Recruitment and Selection Process at Big BazarDocument41 pagesA Project Report ON Recruitment and Selection Process at Big BazarGurusaran SinghNo ratings yet
- 2nd Q Tos and Test-Math3-2023-2024Document10 pages2nd Q Tos and Test-Math3-2023-2024Jessica MoranoNo ratings yet
- Elementary Differential Equations by Earl D Rainville B0000cm3caDocument5 pagesElementary Differential Equations by Earl D Rainville B0000cm3caJohncarlo PanganibanNo ratings yet
- Colgate Brand Image Mapping PDFDocument27 pagesColgate Brand Image Mapping PDFSumedha DuttaNo ratings yet
- Script TemplateDocument8 pagesScript TemplateamberkaplanNo ratings yet
- Republic v. Court of Appeals, G.R. No. 108998, August 24, 1994Document18 pagesRepublic v. Court of Appeals, G.R. No. 108998, August 24, 1994KadzNituraNo ratings yet
- Omnify Sales Process For Swimming Pools by Vipul JhaDocument16 pagesOmnify Sales Process For Swimming Pools by Vipul JhaAshana JhaNo ratings yet
- Judge Merchan Order To Show Cause New York Truth PostsDocument2 pagesJudge Merchan Order To Show Cause New York Truth PostsRobert GouveiaNo ratings yet
- Data Warehousing Quick GuideDocument66 pagesData Warehousing Quick Guidejacktheking2010No ratings yet
- Ethics in OBGYNDocument2 pagesEthics in OBGYNAbdulmajeed AltamimiNo ratings yet
- JAM2015 MA SyllabusDocument1 pageJAM2015 MA Syllabusrcpuram01No ratings yet
- Files-2-Lectures CH 05 Problem Definition and The Research ProposalDocument18 pagesFiles-2-Lectures CH 05 Problem Definition and The Research ProposalAl Hafiz Ibn HamzahNo ratings yet
- Concerto in C Minor - Johann Christian Bach - CelloDocument24 pagesConcerto in C Minor - Johann Christian Bach - CellojosianeNo ratings yet
- Practice Test Cao Hoc 2012Document9 pagesPractice Test Cao Hoc 2012SeaBlueNo ratings yet
- Pages From API.5l.2004-A25Document1 pagePages From API.5l.2004-A25A.ANo ratings yet
- South Sudan Gender AnalysisDocument68 pagesSouth Sudan Gender AnalysisOxfamNo ratings yet
- Marketing ManagementDocument9 pagesMarketing ManagementShashi mehtaNo ratings yet
- Kvs Split Up of Syllabus Class I & IIDocument9 pagesKvs Split Up of Syllabus Class I & IISanjeev MachalNo ratings yet
- Design and Analysis of AlgorithmsDocument200 pagesDesign and Analysis of AlgorithmsChitra RNo ratings yet
- Eating Disorder PPT by Shreyasi MittalDocument35 pagesEating Disorder PPT by Shreyasi MittalPrachi gattaniNo ratings yet
- Customizable Daily Growth PlanDocument12 pagesCustomizable Daily Growth PlanManojkumar Nair100% (1)










































































































Download as docx, pdf, or txt
You might also like
- Acute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology: Precipitating Factors: Etiology: Predisposing FactorsromelynNo ratings yet
- CASE3Document5 pagesCASE3romelynNo ratings yet
- Hygiene (NCLEX) Flashcards - QuizletDocument5 pagesHygiene (NCLEX) Flashcards - QuizletA.No ratings yet
- SOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticDocument5 pagesSOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticvidyahamzahNo ratings yet
- PnclexDocument3 pagesPnclexPaul Michael BaguhinNo ratings yet
- HIV Practice TestDocument2 pagesHIV Practice TestJoslyn GrossNo ratings yet
- Complete Question Bank - Entrepreneurship DevelopmentDocument3 pagesComplete Question Bank - Entrepreneurship DevelopmentUday Gowda100% (1)
- Columbus - Hero or VillainDocument4 pagesColumbus - Hero or Villainapi-264258719No ratings yet
- OB2 - Renal and Urinary Tract Disorders in Pregnancy - Dr. TanDocument6 pagesOB2 - Renal and Urinary Tract Disorders in Pregnancy - Dr. TanHazel Fernandez VillarNo ratings yet
- Initiating A Blood TransfusionDocument5 pagesInitiating A Blood TransfusionJoyce Kathreen Ebio LopezNo ratings yet
- NCP (Burn)Document2 pagesNCP (Burn)Maricel R. ManabatNo ratings yet
- Disaster Nursing P1 Learning PlanDocument5 pagesDisaster Nursing P1 Learning PlanPamela GastalaNo ratings yet
- Cavite State University: I. ObjectivesDocument7 pagesCavite State University: I. ObjectivesChamy CruzNo ratings yet
- CIP-NCM-121-Disaster Nursing-TuesdaysDocument3 pagesCIP-NCM-121-Disaster Nursing-TuesdaysKhen QuiringNo ratings yet
- Foreigh Body Airway Obstruction Management July 2019Document1 pageForeigh Body Airway Obstruction Management July 2019Feliros S. SanciangcoNo ratings yet
- Course Specification Emergency NursingDocument6 pagesCourse Specification Emergency NursingWael LotfyNo ratings yet
- Congruent Care, Which Is The Primary Goal of TransculturalDocument3 pagesCongruent Care, Which Is The Primary Goal of TransculturalPrince SoletaNo ratings yet
- WK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TideDocument43 pagesWK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TidePotato PceeNo ratings yet
- Maternal and Child Health Nursing: KeepsDocument32 pagesMaternal and Child Health Nursing: Keepsshenric16No ratings yet
- Sexually Transmitted InfectionsDocument34 pagesSexually Transmitted InfectionsMariana Creciun100% (1)
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaNo ratings yet
- 08 At-Risk or High-Risk Sick NewbornDocument17 pages08 At-Risk or High-Risk Sick NewbornJAN CAMILLE LENONNo ratings yet
- TLG IV TherapyDocument10 pagesTLG IV TherapyStephanie Joy EscalaNo ratings yet
- AMOEBIASISDocument8 pagesAMOEBIASISCheska ت HortelanoNo ratings yet
- Performing Heimlich ManeuverDocument5 pagesPerforming Heimlich ManeuverAngelie PantajoNo ratings yet
- Submitted By: Bsn-Iv A Submitted To: Clinical Instructor: Cabatbat, Wyen CDocument5 pagesSubmitted By: Bsn-Iv A Submitted To: Clinical Instructor: Cabatbat, Wyen CWyen CabatbatNo ratings yet
- NCM 107 - RleDocument23 pagesNCM 107 - RleMaxinne Allyssa Cancino RoseñoNo ratings yet
- NCM 109 Rle ClinicalDocument20 pagesNCM 109 Rle ClinicalBiway RegalaNo ratings yet
- Competency Appraisal 1Document30 pagesCompetency Appraisal 1mirai desuNo ratings yet
- Making An Occupied BedDocument2 pagesMaking An Occupied BedAnonymous h2EnKyDb100% (1)
- Cesarean Section: Yusef C. Wibowo, S.ST.,M.HDocument6 pagesCesarean Section: Yusef C. Wibowo, S.ST.,M.HberlyanaNo ratings yet
- Mosquito Borne DiseasesDocument31 pagesMosquito Borne DiseasesRizna SaidNo ratings yet
- Teaching Plan 2Document10 pagesTeaching Plan 2Terma JamiriNo ratings yet
- Linear Arrangements of DR InstrumentsDocument42 pagesLinear Arrangements of DR Instrumentsxxegyzz100% (1)
- Naso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringDocument12 pagesNaso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringmeisygraniaNo ratings yet
- Availability and Utilization of Health Informatics System Among Health Workers in Niger State, NigeriaDocument8 pagesAvailability and Utilization of Health Informatics System Among Health Workers in Niger State, NigeriaEditor IJTSRDNo ratings yet
- Expanded Program On ImmunizationDocument23 pagesExpanded Program On ImmunizationKate E. GatchalianNo ratings yet
- Incontinence Case StudyDocument26 pagesIncontinence Case StudyRose AnnNo ratings yet
- NCM 118 - Lesson 7 (Pneumothorax)Document4 pagesNCM 118 - Lesson 7 (Pneumothorax)Bobby Christian DuronNo ratings yet
- Vaccination or ImmunizationDocument4 pagesVaccination or ImmunizationPrincessNo ratings yet
- In The Name of Allah, The Most Beneficent and MercifulDocument35 pagesIn The Name of Allah, The Most Beneficent and MercifulAhmedMenshawyNo ratings yet
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoNo ratings yet
- Health Assessment IntroductionDocument50 pagesHealth Assessment IntroductionEdna Uneta RoblesNo ratings yet
- 10 Golden Rules of IV TherapyDocument8 pages10 Golden Rules of IV Therapybbasya eihynaNo ratings yet
- Administering Pulse OxDocument2 pagesAdministering Pulse OxjepoiNo ratings yet
- Demo Teaching Physical Health AssessmentDocument5 pagesDemo Teaching Physical Health AssessmentJulie May SuganobNo ratings yet
- Emergency Department FlowchartDocument2 pagesEmergency Department FlowchartRaqz LopezNo ratings yet
- 2nd Sem NSG Lec NotesDocument105 pages2nd Sem NSG Lec NotesJan Crizza Dale R. FrancoNo ratings yet
- Hematologic ManagementDocument17 pagesHematologic ManagementAlyssa MontimorNo ratings yet
- Reflective Journal NCM 107 SKL (NIEGAS)Document1 pageReflective Journal NCM 107 SKL (NIEGAS)Dominic GarciaNo ratings yet
- Intensive V (Complications)Document117 pagesIntensive V (Complications)darren55No ratings yet
- Rating Scale: 0 Omitted 1 Poorly Done 2 Fairly Done 3 Well Done Indicates Critical Step Omission or Poor Performance Equates To FailureDocument3 pagesRating Scale: 0 Omitted 1 Poorly Done 2 Fairly Done 3 Well Done Indicates Critical Step Omission or Poor Performance Equates To FailureTemahlungwane100% (2)
- Chikungunya FeverDocument15 pagesChikungunya FeverAyomide AlayandeNo ratings yet
- Prepared By: Sarah Diana Rise S. Manalili, RNDocument38 pagesPrepared By: Sarah Diana Rise S. Manalili, RNSARAH DIANA ROSE S. MANALILI100% (1)
- Journal Gadar Choking-Managing The Risk of Choking GuidelinesDocument18 pagesJournal Gadar Choking-Managing The Risk of Choking GuidelinesnurulNo ratings yet
- Intracranial SurgeryDocument12 pagesIntracranial SurgerysetanpikulanNo ratings yet
- Konsep Palliative Care Pada AnakDocument48 pagesKonsep Palliative Care Pada AnakDayu Dani100% (1)
- MeaslesDocument32 pagesMeaslesYum C100% (2)
- Diphtheria in NepalDocument30 pagesDiphtheria in NepalBinaya100% (1)
- A. Setting Up B. Inserting IV Utilizing The Dummy Arm C. Changing An IV Solution D. Discontinuing An IV InfusionDocument7 pagesA. Setting Up B. Inserting IV Utilizing The Dummy Arm C. Changing An IV Solution D. Discontinuing An IV InfusionJerika Shane MañosoNo ratings yet
- Conceptual Foundation and Critical Care NursingDocument41 pagesConceptual Foundation and Critical Care NursingAbdulNo ratings yet
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- NURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYFrom EverandNURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYNo ratings yet
- SF2 - 2019 - Grade 2 D ROSE FEBDocument3 pagesSF2 - 2019 - Grade 2 D ROSE FEBromelynNo ratings yet
- School Form 2 (SF2) Daily Attendance Report of Learners: X XX X X X XX X XDocument6 pagesSchool Form 2 (SF2) Daily Attendance Report of Learners: X XX X X X XX X XromelynNo ratings yet
- SF2 - 2019 - Grade 2 D ROSE APRILDocument3 pagesSF2 - 2019 - Grade 2 D ROSE APRILromelynNo ratings yet
- Output 3 - Family Health NursingDocument9 pagesOutput 3 - Family Health Nursingromelyn100% (1)
- Mary Jesrel J. Cudia BSN Ii-A: RightsDocument3 pagesMary Jesrel J. Cudia BSN Ii-A: RightsromelynNo ratings yet
- Output 3 - Family Health NursingDocument5 pagesOutput 3 - Family Health NursingromelynNo ratings yet
- Intensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 4: Pre - School (Respiratory System)Document5 pagesIntensive Nursing Practicum - Pediatric Ward (BMC) CASE STUDY 4: Pre - School (Respiratory System)romelynNo ratings yet
- Inp 402.rubics - Case.anaDocument2 pagesInp 402.rubics - Case.anaromelyn0% (1)
- Nursing Care Plan (NCP) For Acute Lymphocytic LeukemiaDocument4 pagesNursing Care Plan (NCP) For Acute Lymphocytic LeukemiaromelynNo ratings yet
- NCP 2Document3 pagesNCP 2romelyn100% (1)
- Inp Rle Pedia Ward Case7Document1 pageInp Rle Pedia Ward Case7romelynNo ratings yet
- School Forms Checking Report (SFCR) : Table 1. Learners Record Examined/ReviewedDocument1 pageSchool Forms Checking Report (SFCR) : Table 1. Learners Record Examined/ReviewedromelynNo ratings yet
- NURSING HEALTH HISTORYup.Document5 pagesNURSING HEALTH HISTORYup.romelynNo ratings yet
- Preparing To Use A Nebulizer: 1 Wash Your HandsDocument4 pagesPreparing To Use A Nebulizer: 1 Wash Your HandsromelynNo ratings yet
- ESP A.P English MTB Math Filipino MAPEH (Art) : GRADES 1 To 12 Daily Lesson LogDocument9 pagesESP A.P English MTB Math Filipino MAPEH (Art) : GRADES 1 To 12 Daily Lesson LogromelynNo ratings yet
- Health History: I. Personal DataDocument7 pagesHealth History: I. Personal DataromelynNo ratings yet
- Sf2 - 2019 - Grade 2 - D - Rose (June)Document1 pageSf2 - 2019 - Grade 2 - D - Rose (June)romelynNo ratings yet
- PhillipDocument4 pagesPhilliplucasdoriamaiaNo ratings yet
- 21 Days Prayer Fasting RiversideDocument5 pages21 Days Prayer Fasting RiversideAnaPereiraNo ratings yet
- When To Salute - Military Protocol Guide To Showing RespectDocument20 pagesWhen To Salute - Military Protocol Guide To Showing RespectGreg JohnsonNo ratings yet
- Work Function: Applications MeasurementDocument10 pagesWork Function: Applications MeasurementshiravandNo ratings yet
- Ancient Athens Brochure Assignment and RubricDocument2 pagesAncient Athens Brochure Assignment and Rubricapi-297382264No ratings yet
- LiberalismDocument3 pagesLiberalismNafis FuadNo ratings yet
- Drimzo Oil Interview FormDocument2 pagesDrimzo Oil Interview Formdmita9276No ratings yet
- A Project Report ON Recruitment and Selection Process at Big BazarDocument41 pagesA Project Report ON Recruitment and Selection Process at Big BazarGurusaran SinghNo ratings yet
- 2nd Q Tos and Test-Math3-2023-2024Document10 pages2nd Q Tos and Test-Math3-2023-2024Jessica MoranoNo ratings yet
- Elementary Differential Equations by Earl D Rainville B0000cm3caDocument5 pagesElementary Differential Equations by Earl D Rainville B0000cm3caJohncarlo PanganibanNo ratings yet
- Colgate Brand Image Mapping PDFDocument27 pagesColgate Brand Image Mapping PDFSumedha DuttaNo ratings yet
- Script TemplateDocument8 pagesScript TemplateamberkaplanNo ratings yet
- Republic v. Court of Appeals, G.R. No. 108998, August 24, 1994Document18 pagesRepublic v. Court of Appeals, G.R. No. 108998, August 24, 1994KadzNituraNo ratings yet
- Omnify Sales Process For Swimming Pools by Vipul JhaDocument16 pagesOmnify Sales Process For Swimming Pools by Vipul JhaAshana JhaNo ratings yet
- Judge Merchan Order To Show Cause New York Truth PostsDocument2 pagesJudge Merchan Order To Show Cause New York Truth PostsRobert GouveiaNo ratings yet
- Data Warehousing Quick GuideDocument66 pagesData Warehousing Quick Guidejacktheking2010No ratings yet
- Ethics in OBGYNDocument2 pagesEthics in OBGYNAbdulmajeed AltamimiNo ratings yet
- JAM2015 MA SyllabusDocument1 pageJAM2015 MA Syllabusrcpuram01No ratings yet
- Files-2-Lectures CH 05 Problem Definition and The Research ProposalDocument18 pagesFiles-2-Lectures CH 05 Problem Definition and The Research ProposalAl Hafiz Ibn HamzahNo ratings yet
- Concerto in C Minor - Johann Christian Bach - CelloDocument24 pagesConcerto in C Minor - Johann Christian Bach - CellojosianeNo ratings yet
- Practice Test Cao Hoc 2012Document9 pagesPractice Test Cao Hoc 2012SeaBlueNo ratings yet
- Pages From API.5l.2004-A25Document1 pagePages From API.5l.2004-A25A.ANo ratings yet
- South Sudan Gender AnalysisDocument68 pagesSouth Sudan Gender AnalysisOxfamNo ratings yet
- Marketing ManagementDocument9 pagesMarketing ManagementShashi mehtaNo ratings yet
- Kvs Split Up of Syllabus Class I & IIDocument9 pagesKvs Split Up of Syllabus Class I & IISanjeev MachalNo ratings yet
- Design and Analysis of AlgorithmsDocument200 pagesDesign and Analysis of AlgorithmsChitra RNo ratings yet
- Eating Disorder PPT by Shreyasi MittalDocument35 pagesEating Disorder PPT by Shreyasi MittalPrachi gattaniNo ratings yet
- Customizable Daily Growth PlanDocument12 pagesCustomizable Daily Growth PlanManojkumar Nair100% (1)