
Program Registration Form
Program Registration Form
You might also like
- The DeadDocument837 pagesThe DeadLee Keeron86% (7)
- Caesars Sportsbook Prop Betting Menu - Super Bowl LVII - FinalDocument22 pagesCaesars Sportsbook Prop Betting Menu - Super Bowl LVII - FinalTony Garcia100% (1)
- Standard Quality Assurance Plan For Ac MotorDocument6 pagesStandard Quality Assurance Plan For Ac MotorSonti Mani kumar100% (1)
- B48PFF3071T3M Service ManualDocument30 pagesB48PFF3071T3M Service Manualanton Gonzalez0% (1)
- Endocrinology - Polyuria - SOAP Note - Jeanette GoguenDocument3 pagesEndocrinology - Polyuria - SOAP Note - Jeanette GoguenFrancieudo SampaioNo ratings yet
- CATC Camp Forms OnlyDocument2 pagesCATC Camp Forms OnlyManas Chetry50% (4)
- How To Date The Hottest Women… Online And OfflineFrom EverandHow To Date The Hottest Women… Online And OfflineRating: 5 out of 5 stars5/5 (1)
- BEGINNERDocument1 pageBEGINNERKeyur GadaNo ratings yet
- Curriculum WBBDocument202 pagesCurriculum WBBKeyur GadaNo ratings yet
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- Annexure 1 & 2Document1 pageAnnexure 1 & 2Hardik ChhabraNo ratings yet
- Application Form Student PackageDocument2 pagesApplication Form Student PackageVÁRÚŃ DzNo ratings yet
- UndertakingDocument1 pageUndertakingSoumya BhardwajNo ratings yet
- Candidate Details FormDocument3 pagesCandidate Details Formyour voicetechNo ratings yet
- Employment ApplicationDocument2 pagesEmployment Applicationnetposting_2No ratings yet
- Dossier InscriptionDocument2 pagesDossier Inscriptionglouden fullenNo ratings yet
- Mks CPSB Job Application Form 2022Document3 pagesMks CPSB Job Application Form 2022n8brjz5n8zNo ratings yet
- Mks CPSB Form 2022Document3 pagesMks CPSB Form 2022Eunice Mueni paulNo ratings yet
- Consent Form For Travelling OutsideDocument2 pagesConsent Form For Travelling Outsidejnu.saifulislamshakilNo ratings yet
- New Glico Travel Insurance Form For Both Regular & FamilyDocument1 pageNew Glico Travel Insurance Form For Both Regular & FamilyjoeNo ratings yet
- UBTH Application FormDocument4 pagesUBTH Application FormNi'imatullahiNo ratings yet
- Appendix 4 - Kyc Form by Site Visit For Different Ccris Supplementary Report or SpekarDocument1 pageAppendix 4 - Kyc Form by Site Visit For Different Ccris Supplementary Report or Spekarahmad bahiyuddin21No ratings yet
- University of Colombo, Sri Lanka Faculty of Law Department of Private and Comparative LawDocument3 pagesUniversity of Colombo, Sri Lanka Faculty of Law Department of Private and Comparative Law22nk5yq2d9No ratings yet
- Application FormDocument4 pagesApplication FormmaasandhyaessentialgroupNo ratings yet
- Kementerian Pendidikan Dan Kebudayaan Universitas Negeri Malang (Um)Document1 pageKementerian Pendidikan Dan Kebudayaan Universitas Negeri Malang (Um)zahrul ichsan wajdiNo ratings yet
- Application Form For Original Pass Certificate: Srimanta Sankaradeva University of Health SciencesDocument2 pagesApplication Form For Original Pass Certificate: Srimanta Sankaradeva University of Health SciencesHimangsuNo ratings yet
- Quraan Class Enrollment FormDocument1 pageQuraan Class Enrollment Formராஜா MVSNo ratings yet
- DOWRY DeclarationDocument1 pageDOWRY Declarationnasla pNo ratings yet
- Annexture A Staff Particulars and Contact Details of MembersDocument3 pagesAnnexture A Staff Particulars and Contact Details of MembersPrivilegeNo ratings yet
- Photo: Application FormDocument2 pagesPhoto: Application FormjkNo ratings yet
- 2021-New Application Form For Individual Membership FieldsDocument4 pages2021-New Application Form For Individual Membership FieldsLukhanyoNo ratings yet
- Application FormDocument2 pagesApplication Formapi-227090856No ratings yet
- CDCE 2014 Application 15th BatchDocument12 pagesCDCE 2014 Application 15th BatchThang Thawn TuangNo ratings yet
- Revised Corporate Account Opening FormDocument10 pagesRevised Corporate Account Opening FormFrancis NdumbaroNo ratings yet
- 7 - Tracer Study Form For Graduates (FINAL)Document6 pages7 - Tracer Study Form For Graduates (FINAL)Kia AdionNo ratings yet
- Job Application Form-1Document4 pagesJob Application Form-1musa ballah koromaNo ratings yet
- Prescribed Application Form ADocument3 pagesPrescribed Application Form ABhavish RamroopNo ratings yet
- Enrollment Form: EducationDocument2 pagesEnrollment Form: EducationS V ENTERPRISES67% (3)
- Apll Enrollment FormDocument2 pagesApll Enrollment FormUjjval KumarNo ratings yet
- Guarantors FORM - Doc BADocument3 pagesGuarantors FORM - Doc BAagbaipissNo ratings yet
- Dependant's Bursary Application FormDocument3 pagesDependant's Bursary Application Formal lakwenaNo ratings yet
- BFC Employment Application Form v4Document4 pagesBFC Employment Application Form v4Sofia Linelle P EdecerNo ratings yet
- Laadli Regn FormDocument1 pageLaadli Regn FormVansh AggarwalNo ratings yet
- Application Form: Black Ink and BLOCK CAPITALSDocument5 pagesApplication Form: Black Ink and BLOCK CAPITALSZack ALGNo ratings yet
- Interview Form - TesoropetrolDocument2 pagesInterview Form - Tesoropetrolkudabo oluwatosinNo ratings yet
- Application FormDocument2 pagesApplication Formtech visionNo ratings yet
- IIA RegistrationDocument3 pagesIIA RegistrationJohn CramwellNo ratings yet
- Application Form ITK LeipzigDocument4 pagesApplication Form ITK LeipzigbpembdisporapulpisNo ratings yet
- Form NCC CampDocument2 pagesForm NCC CampREJI G.DNo ratings yet
- Student Application - Visa FormDocument3 pagesStudent Application - Visa FormTam LeNo ratings yet
- Nursery Application Form - Docx 2Document10 pagesNursery Application Form - Docx 2Hamza YasinNo ratings yet
- Application Form Date of Joining: 10 September, 2019 Data Entry OperatorDocument3 pagesApplication Form Date of Joining: 10 September, 2019 Data Entry Operatorkmr ShivamNo ratings yet
- Curiculum Vitae: EDUCATION & TRAINING (Specialty) Period, Name of School, Address Specialty, CertificateDocument2 pagesCuriculum Vitae: EDUCATION & TRAINING (Specialty) Period, Name of School, Address Specialty, CertificatethetiepNo ratings yet
- Specimen ApplicationDocument2 pagesSpecimen Applicationrathiy intechNo ratings yet
- Form Rekom S3Document2 pagesForm Rekom S3BEN SUPRINo ratings yet
- BFC Employment Application Form v4 PDFDocument4 pagesBFC Employment Application Form v4 PDFMutie Ul Rehman BhuttaNo ratings yet
- HYA Form Silver Ilovepdf CompressedDocument1 pageHYA Form Silver Ilovepdf CompressedUtkarsh VasaniNo ratings yet
- All Other Application Form 2Document7 pagesAll Other Application Form 2najmahNo ratings yet
- Curriculum Vitae - TipDocument1 pageCurriculum Vitae - Tipclau2u.serbanNo ratings yet
- Application Form LusundvuDocument4 pagesApplication Form Lusundvubusiswamavimbela06No ratings yet
- MV Registration & DL LL FormDocument2 pagesMV Registration & DL LL Formkarma wangyalNo ratings yet
- Undergraduate Application FormDocument2 pagesUndergraduate Application FormMizero Aime olivierNo ratings yet
- BASES JEDPA 2023 Removed RemovedDocument1 pageBASES JEDPA 2023 Removed RemovedPerez EvertNo ratings yet
- Registration Form: Ref: Advertisement No: 37/2020-HRD Post Code No.:...............Document2 pagesRegistration Form: Ref: Advertisement No: 37/2020-HRD Post Code No.:...............ankitNo ratings yet
- P.& J Application FormDocument2 pagesP.& J Application FormsdcrownjohnNo ratings yet
- Insurance and Full and Final Settlement DeclarationDocument1 pageInsurance and Full and Final Settlement Declarationsiva ramNo ratings yet
- Application Forms For Trainee Technician MembersDocument6 pagesApplication Forms For Trainee Technician MembersSilas Nana-Baah MensahNo ratings yet
- Metaverse and NFT Investing 2022 and Beyond: A Beginners Guide On Making Money In Virtual Lands, Blockchain Gaming, Non-Fungible Tokens, Crypto Art, DeFi Projects, Smart Contracts, Web 3.0From EverandMetaverse and NFT Investing 2022 and Beyond: A Beginners Guide On Making Money In Virtual Lands, Blockchain Gaming, Non-Fungible Tokens, Crypto Art, DeFi Projects, Smart Contracts, Web 3.0No ratings yet
- How To Edit This Worksheet: Copy "Document10 pagesHow To Edit This Worksheet: Copy "Keyur GadaNo ratings yet
- How To Edit This Worksheet: Copy "Document9 pagesHow To Edit This Worksheet: Copy "Keyur GadaNo ratings yet
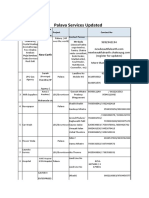
- Palava Services UpdatedDocument2 pagesPalava Services UpdatedKeyur GadaNo ratings yet
- Kevins FEN Viewer BasicDocument3 pagesKevins FEN Viewer BasicKeyur GadaNo ratings yet
- Art, Culture & Events Resident Committee Nomination Form.: Will Be Composed of 5 Nominated Palava ResidentsDocument2 pagesArt, Culture & Events Resident Committee Nomination Form.: Will Be Composed of 5 Nominated Palava ResidentsKeyur GadaNo ratings yet
- I Radiate Confidence, Beauty and GraceDocument2 pagesI Radiate Confidence, Beauty and GraceKeyur GadaNo ratings yet
- Chess Club AttendanceDocument6 pagesChess Club AttendanceKeyur GadaNo ratings yet
- Enjoy A Naturally Rejuvenating Alternative To Treat Yourself With Himalayan Wellness Products!Document6 pagesEnjoy A Naturally Rejuvenating Alternative To Treat Yourself With Himalayan Wellness Products!Keyur GadaNo ratings yet
- Coming Soon - Ash Gourd JuiceDocument5 pagesComing Soon - Ash Gourd JuiceKeyur GadaNo ratings yet
- THE CHESS CLUB - Registration FormDocument2 pagesTHE CHESS CLUB - Registration FormKeyur GadaNo ratings yet
- Facenovice Intermediate AdvancedDocument2 pagesFacenovice Intermediate AdvancedKeyur GadaNo ratings yet
- The Dynamics of Critical ThinkingDocument3 pagesThe Dynamics of Critical ThinkingKeyur GadaNo ratings yet
- J.H. Blake - Chess Endings For Beginners 7th EdDocument1 pageJ.H. Blake - Chess Endings For Beginners 7th EdKeyur Gada0% (1)
- Funda Test DrillDocument32 pagesFunda Test DrillNurseRiemNo ratings yet
- Rooftop Fish FarmsDocument4 pagesRooftop Fish FarmsbobsraineyNo ratings yet
- JaxfunDocument91 pagesJaxfunCasper ManNo ratings yet
- Skin Staples HectingDocument5 pagesSkin Staples HectingdesyNo ratings yet
- Magna Carta of Women Implementing Rules and RegulationsDocument47 pagesMagna Carta of Women Implementing Rules and RegulationsJems100% (2)
- Ecology Lesson 3 PDFDocument14 pagesEcology Lesson 3 PDFKelly MccartyNo ratings yet
- Gate Driver Design - From Basics To Details: Wei ZhangDocument33 pagesGate Driver Design - From Basics To Details: Wei ZhangRajiv ChaudhariNo ratings yet
- 13 - Photosynthesis AQA BookletDocument28 pages13 - Photosynthesis AQA BookletSevilay CaferogluNo ratings yet
- Commissioning: SAIS Information For BuffersDocument16 pagesCommissioning: SAIS Information For BuffersAli DiabNo ratings yet
- Sandvik Cs550 Cone Crusher: Technical SpecificationDocument8 pagesSandvik Cs550 Cone Crusher: Technical SpecificationLmf DanielNo ratings yet
- Castrol Activ Scooter 10W-40 4-ATDocument2 pagesCastrol Activ Scooter 10W-40 4-ATDitha KiranaNo ratings yet
- Child'S Horoscop E: Astrological Interpretation and Text Liz Greene Programming Alois TreindlDocument28 pagesChild'S Horoscop E: Astrological Interpretation and Text Liz Greene Programming Alois TreindlRamanasarmaNo ratings yet
- Handbook MBBS 2013 2014Document221 pagesHandbook MBBS 2013 2014Abd SamadNo ratings yet
- Advisory Committee On Human Radiation Experiments-1053 PDFDocument1,053 pagesAdvisory Committee On Human Radiation Experiments-1053 PDFsagor sagor100% (1)
- Midterm Review 2Document82 pagesMidterm Review 2middletown njNo ratings yet
- PVSyst Loss Description - by Filipe AndradeDocument12 pagesPVSyst Loss Description - by Filipe AndradeMezrag mohamedNo ratings yet
- Conval Training Material Part 1Document23 pagesConval Training Material Part 1Kumar Phanishwar50% (2)
- Cell Organelles Worksheet-PrintDocument2 pagesCell Organelles Worksheet-PrintmuraliMuNo ratings yet
- Methods of Constructing Earthen DamsDocument3 pagesMethods of Constructing Earthen DamsZac MwebNo ratings yet
- Chapter - 9 Fluorescence SpectrosDocument12 pagesChapter - 9 Fluorescence SpectrosMadhur ShrivastavaNo ratings yet
- Jadwal PM JanuariDocument3 pagesJadwal PM JanuariZulkarnain HNo ratings yet
- Chapter 5Document5 pagesChapter 5Rena Jocelle NalzaroNo ratings yet
- ITDI Hand Sanitizer Production 07172020Document27 pagesITDI Hand Sanitizer Production 07172020Marilyn LaquindanumNo ratings yet
- Cabison - Histopath ReviewerDocument17 pagesCabison - Histopath ReviewerPatricia CabisonNo ratings yet






































































































Download as docx, pdf, or txt
You might also like
- The DeadDocument837 pagesThe DeadLee Keeron86% (7)
- Caesars Sportsbook Prop Betting Menu - Super Bowl LVII - FinalDocument22 pagesCaesars Sportsbook Prop Betting Menu - Super Bowl LVII - FinalTony Garcia100% (1)
- Standard Quality Assurance Plan For Ac MotorDocument6 pagesStandard Quality Assurance Plan For Ac MotorSonti Mani kumar100% (1)
- B48PFF3071T3M Service ManualDocument30 pagesB48PFF3071T3M Service Manualanton Gonzalez0% (1)
- Endocrinology - Polyuria - SOAP Note - Jeanette GoguenDocument3 pagesEndocrinology - Polyuria - SOAP Note - Jeanette GoguenFrancieudo SampaioNo ratings yet
- CATC Camp Forms OnlyDocument2 pagesCATC Camp Forms OnlyManas Chetry50% (4)
- How To Date The Hottest Women… Online And OfflineFrom EverandHow To Date The Hottest Women… Online And OfflineRating: 5 out of 5 stars5/5 (1)
- BEGINNERDocument1 pageBEGINNERKeyur GadaNo ratings yet
- Curriculum WBBDocument202 pagesCurriculum WBBKeyur GadaNo ratings yet
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- Annexure 1 & 2Document1 pageAnnexure 1 & 2Hardik ChhabraNo ratings yet
- Application Form Student PackageDocument2 pagesApplication Form Student PackageVÁRÚŃ DzNo ratings yet
- UndertakingDocument1 pageUndertakingSoumya BhardwajNo ratings yet
- Candidate Details FormDocument3 pagesCandidate Details Formyour voicetechNo ratings yet
- Employment ApplicationDocument2 pagesEmployment Applicationnetposting_2No ratings yet
- Dossier InscriptionDocument2 pagesDossier Inscriptionglouden fullenNo ratings yet
- Mks CPSB Job Application Form 2022Document3 pagesMks CPSB Job Application Form 2022n8brjz5n8zNo ratings yet
- Mks CPSB Form 2022Document3 pagesMks CPSB Form 2022Eunice Mueni paulNo ratings yet
- Consent Form For Travelling OutsideDocument2 pagesConsent Form For Travelling Outsidejnu.saifulislamshakilNo ratings yet
- New Glico Travel Insurance Form For Both Regular & FamilyDocument1 pageNew Glico Travel Insurance Form For Both Regular & FamilyjoeNo ratings yet
- UBTH Application FormDocument4 pagesUBTH Application FormNi'imatullahiNo ratings yet
- Appendix 4 - Kyc Form by Site Visit For Different Ccris Supplementary Report or SpekarDocument1 pageAppendix 4 - Kyc Form by Site Visit For Different Ccris Supplementary Report or Spekarahmad bahiyuddin21No ratings yet
- University of Colombo, Sri Lanka Faculty of Law Department of Private and Comparative LawDocument3 pagesUniversity of Colombo, Sri Lanka Faculty of Law Department of Private and Comparative Law22nk5yq2d9No ratings yet
- Application FormDocument4 pagesApplication FormmaasandhyaessentialgroupNo ratings yet
- Kementerian Pendidikan Dan Kebudayaan Universitas Negeri Malang (Um)Document1 pageKementerian Pendidikan Dan Kebudayaan Universitas Negeri Malang (Um)zahrul ichsan wajdiNo ratings yet
- Application Form For Original Pass Certificate: Srimanta Sankaradeva University of Health SciencesDocument2 pagesApplication Form For Original Pass Certificate: Srimanta Sankaradeva University of Health SciencesHimangsuNo ratings yet
- Quraan Class Enrollment FormDocument1 pageQuraan Class Enrollment Formராஜா MVSNo ratings yet
- DOWRY DeclarationDocument1 pageDOWRY Declarationnasla pNo ratings yet
- Annexture A Staff Particulars and Contact Details of MembersDocument3 pagesAnnexture A Staff Particulars and Contact Details of MembersPrivilegeNo ratings yet
- Photo: Application FormDocument2 pagesPhoto: Application FormjkNo ratings yet
- 2021-New Application Form For Individual Membership FieldsDocument4 pages2021-New Application Form For Individual Membership FieldsLukhanyoNo ratings yet
- Application FormDocument2 pagesApplication Formapi-227090856No ratings yet
- CDCE 2014 Application 15th BatchDocument12 pagesCDCE 2014 Application 15th BatchThang Thawn TuangNo ratings yet
- Revised Corporate Account Opening FormDocument10 pagesRevised Corporate Account Opening FormFrancis NdumbaroNo ratings yet
- 7 - Tracer Study Form For Graduates (FINAL)Document6 pages7 - Tracer Study Form For Graduates (FINAL)Kia AdionNo ratings yet
- Job Application Form-1Document4 pagesJob Application Form-1musa ballah koromaNo ratings yet
- Prescribed Application Form ADocument3 pagesPrescribed Application Form ABhavish RamroopNo ratings yet
- Enrollment Form: EducationDocument2 pagesEnrollment Form: EducationS V ENTERPRISES67% (3)
- Apll Enrollment FormDocument2 pagesApll Enrollment FormUjjval KumarNo ratings yet
- Guarantors FORM - Doc BADocument3 pagesGuarantors FORM - Doc BAagbaipissNo ratings yet
- Dependant's Bursary Application FormDocument3 pagesDependant's Bursary Application Formal lakwenaNo ratings yet
- BFC Employment Application Form v4Document4 pagesBFC Employment Application Form v4Sofia Linelle P EdecerNo ratings yet
- Laadli Regn FormDocument1 pageLaadli Regn FormVansh AggarwalNo ratings yet
- Application Form: Black Ink and BLOCK CAPITALSDocument5 pagesApplication Form: Black Ink and BLOCK CAPITALSZack ALGNo ratings yet
- Interview Form - TesoropetrolDocument2 pagesInterview Form - Tesoropetrolkudabo oluwatosinNo ratings yet
- Application FormDocument2 pagesApplication Formtech visionNo ratings yet
- IIA RegistrationDocument3 pagesIIA RegistrationJohn CramwellNo ratings yet
- Application Form ITK LeipzigDocument4 pagesApplication Form ITK LeipzigbpembdisporapulpisNo ratings yet
- Form NCC CampDocument2 pagesForm NCC CampREJI G.DNo ratings yet
- Student Application - Visa FormDocument3 pagesStudent Application - Visa FormTam LeNo ratings yet
- Nursery Application Form - Docx 2Document10 pagesNursery Application Form - Docx 2Hamza YasinNo ratings yet
- Application Form Date of Joining: 10 September, 2019 Data Entry OperatorDocument3 pagesApplication Form Date of Joining: 10 September, 2019 Data Entry Operatorkmr ShivamNo ratings yet
- Curiculum Vitae: EDUCATION & TRAINING (Specialty) Period, Name of School, Address Specialty, CertificateDocument2 pagesCuriculum Vitae: EDUCATION & TRAINING (Specialty) Period, Name of School, Address Specialty, CertificatethetiepNo ratings yet
- Specimen ApplicationDocument2 pagesSpecimen Applicationrathiy intechNo ratings yet
- Form Rekom S3Document2 pagesForm Rekom S3BEN SUPRINo ratings yet
- BFC Employment Application Form v4 PDFDocument4 pagesBFC Employment Application Form v4 PDFMutie Ul Rehman BhuttaNo ratings yet
- HYA Form Silver Ilovepdf CompressedDocument1 pageHYA Form Silver Ilovepdf CompressedUtkarsh VasaniNo ratings yet
- All Other Application Form 2Document7 pagesAll Other Application Form 2najmahNo ratings yet
- Curriculum Vitae - TipDocument1 pageCurriculum Vitae - Tipclau2u.serbanNo ratings yet
- Application Form LusundvuDocument4 pagesApplication Form Lusundvubusiswamavimbela06No ratings yet
- MV Registration & DL LL FormDocument2 pagesMV Registration & DL LL Formkarma wangyalNo ratings yet
- Undergraduate Application FormDocument2 pagesUndergraduate Application FormMizero Aime olivierNo ratings yet
- BASES JEDPA 2023 Removed RemovedDocument1 pageBASES JEDPA 2023 Removed RemovedPerez EvertNo ratings yet
- Registration Form: Ref: Advertisement No: 37/2020-HRD Post Code No.:...............Document2 pagesRegistration Form: Ref: Advertisement No: 37/2020-HRD Post Code No.:...............ankitNo ratings yet
- P.& J Application FormDocument2 pagesP.& J Application FormsdcrownjohnNo ratings yet
- Insurance and Full and Final Settlement DeclarationDocument1 pageInsurance and Full and Final Settlement Declarationsiva ramNo ratings yet
- Application Forms For Trainee Technician MembersDocument6 pagesApplication Forms For Trainee Technician MembersSilas Nana-Baah MensahNo ratings yet
- Metaverse and NFT Investing 2022 and Beyond: A Beginners Guide On Making Money In Virtual Lands, Blockchain Gaming, Non-Fungible Tokens, Crypto Art, DeFi Projects, Smart Contracts, Web 3.0From EverandMetaverse and NFT Investing 2022 and Beyond: A Beginners Guide On Making Money In Virtual Lands, Blockchain Gaming, Non-Fungible Tokens, Crypto Art, DeFi Projects, Smart Contracts, Web 3.0No ratings yet
- How To Edit This Worksheet: Copy "Document10 pagesHow To Edit This Worksheet: Copy "Keyur GadaNo ratings yet
- How To Edit This Worksheet: Copy "Document9 pagesHow To Edit This Worksheet: Copy "Keyur GadaNo ratings yet
- Palava Services UpdatedDocument2 pagesPalava Services UpdatedKeyur GadaNo ratings yet
- Kevins FEN Viewer BasicDocument3 pagesKevins FEN Viewer BasicKeyur GadaNo ratings yet
- Art, Culture & Events Resident Committee Nomination Form.: Will Be Composed of 5 Nominated Palava ResidentsDocument2 pagesArt, Culture & Events Resident Committee Nomination Form.: Will Be Composed of 5 Nominated Palava ResidentsKeyur GadaNo ratings yet
- I Radiate Confidence, Beauty and GraceDocument2 pagesI Radiate Confidence, Beauty and GraceKeyur GadaNo ratings yet
- Chess Club AttendanceDocument6 pagesChess Club AttendanceKeyur GadaNo ratings yet
- Enjoy A Naturally Rejuvenating Alternative To Treat Yourself With Himalayan Wellness Products!Document6 pagesEnjoy A Naturally Rejuvenating Alternative To Treat Yourself With Himalayan Wellness Products!Keyur GadaNo ratings yet
- Coming Soon - Ash Gourd JuiceDocument5 pagesComing Soon - Ash Gourd JuiceKeyur GadaNo ratings yet
- THE CHESS CLUB - Registration FormDocument2 pagesTHE CHESS CLUB - Registration FormKeyur GadaNo ratings yet
- Facenovice Intermediate AdvancedDocument2 pagesFacenovice Intermediate AdvancedKeyur GadaNo ratings yet
- The Dynamics of Critical ThinkingDocument3 pagesThe Dynamics of Critical ThinkingKeyur GadaNo ratings yet
- J.H. Blake - Chess Endings For Beginners 7th EdDocument1 pageJ.H. Blake - Chess Endings For Beginners 7th EdKeyur Gada0% (1)
- Funda Test DrillDocument32 pagesFunda Test DrillNurseRiemNo ratings yet
- Rooftop Fish FarmsDocument4 pagesRooftop Fish FarmsbobsraineyNo ratings yet
- JaxfunDocument91 pagesJaxfunCasper ManNo ratings yet
- Skin Staples HectingDocument5 pagesSkin Staples HectingdesyNo ratings yet
- Magna Carta of Women Implementing Rules and RegulationsDocument47 pagesMagna Carta of Women Implementing Rules and RegulationsJems100% (2)
- Ecology Lesson 3 PDFDocument14 pagesEcology Lesson 3 PDFKelly MccartyNo ratings yet
- Gate Driver Design - From Basics To Details: Wei ZhangDocument33 pagesGate Driver Design - From Basics To Details: Wei ZhangRajiv ChaudhariNo ratings yet
- 13 - Photosynthesis AQA BookletDocument28 pages13 - Photosynthesis AQA BookletSevilay CaferogluNo ratings yet
- Commissioning: SAIS Information For BuffersDocument16 pagesCommissioning: SAIS Information For BuffersAli DiabNo ratings yet
- Sandvik Cs550 Cone Crusher: Technical SpecificationDocument8 pagesSandvik Cs550 Cone Crusher: Technical SpecificationLmf DanielNo ratings yet
- Castrol Activ Scooter 10W-40 4-ATDocument2 pagesCastrol Activ Scooter 10W-40 4-ATDitha KiranaNo ratings yet
- Child'S Horoscop E: Astrological Interpretation and Text Liz Greene Programming Alois TreindlDocument28 pagesChild'S Horoscop E: Astrological Interpretation and Text Liz Greene Programming Alois TreindlRamanasarmaNo ratings yet
- Handbook MBBS 2013 2014Document221 pagesHandbook MBBS 2013 2014Abd SamadNo ratings yet
- Advisory Committee On Human Radiation Experiments-1053 PDFDocument1,053 pagesAdvisory Committee On Human Radiation Experiments-1053 PDFsagor sagor100% (1)
- Midterm Review 2Document82 pagesMidterm Review 2middletown njNo ratings yet
- PVSyst Loss Description - by Filipe AndradeDocument12 pagesPVSyst Loss Description - by Filipe AndradeMezrag mohamedNo ratings yet
- Conval Training Material Part 1Document23 pagesConval Training Material Part 1Kumar Phanishwar50% (2)
- Cell Organelles Worksheet-PrintDocument2 pagesCell Organelles Worksheet-PrintmuraliMuNo ratings yet
- Methods of Constructing Earthen DamsDocument3 pagesMethods of Constructing Earthen DamsZac MwebNo ratings yet
- Chapter - 9 Fluorescence SpectrosDocument12 pagesChapter - 9 Fluorescence SpectrosMadhur ShrivastavaNo ratings yet
- Jadwal PM JanuariDocument3 pagesJadwal PM JanuariZulkarnain HNo ratings yet
- Chapter 5Document5 pagesChapter 5Rena Jocelle NalzaroNo ratings yet
- ITDI Hand Sanitizer Production 07172020Document27 pagesITDI Hand Sanitizer Production 07172020Marilyn LaquindanumNo ratings yet
- Cabison - Histopath ReviewerDocument17 pagesCabison - Histopath ReviewerPatricia CabisonNo ratings yet