Download as pdf or txt
You might also like
- Mapeh Least Learned Competencies 6Document5 pagesMapeh Least Learned Competencies 6Anonymous QnNICuArTx75% (12)
- M Test (Meridian Test) MukainoDocument11 pagesM Test (Meridian Test) MukainoVicente Acosta100% (1)
- Subiecte Olimpiadă Limba Engleză Clasa A 9aDocument3 pagesSubiecte Olimpiadă Limba Engleză Clasa A 9akallai annamaria100% (1)
- 2018 Evidence Based PV PDFDocument280 pages2018 Evidence Based PV PDFFRANKNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Bachata Dance PDFDocument3 pagesBachata Dance PDFAbbey Joy CollanoNo ratings yet
- Holistic Treatment of Lyme DiseaseDocument54 pagesHolistic Treatment of Lyme Diseasefrederic9866No ratings yet
- Global Animal Feed Additives MarketDocument18 pagesGlobal Animal Feed Additives MarketSanjay MatthewsNo ratings yet
- PharmacovigilanceDocument45 pagesPharmacovigilancepavani valluriNo ratings yet
- Pharmacovigilance: Masterkey To Drug Safety Monitoring and Its Status in IndiaDocument4 pagesPharmacovigilance: Masterkey To Drug Safety Monitoring and Its Status in IndiaSejal khumanNo ratings yet
- Pharmacovigilance Ensuring The Safe Use of MedicinesDocument18 pagesPharmacovigilance Ensuring The Safe Use of MedicinespopadrianionutzNo ratings yet
- Medication Errors: Pharmacovigilance Centres in Detection and PreventionDocument4 pagesMedication Errors: Pharmacovigilance Centres in Detection and PreventiongabyvaleNo ratings yet
- Pharmacovigilance Paper PDFDocument19 pagesPharmacovigilance Paper PDFHassan Ahmed KhanNo ratings yet
- IntroductionDocument22 pagesIntroductionsaurabh dhyaniNo ratings yet
- Importance of Pharmacovigilance For Pharmaceutical IndustryDocument24 pagesImportance of Pharmacovigilance For Pharmaceutical IndustryPiratesNo ratings yet
- Pharmacovigilance Report MAIN-1Document33 pagesPharmacovigilance Report MAIN-19Asfara AzeezNo ratings yet
- Establishing Pharmacovigilance programmeDocument23 pagesEstablishing Pharmacovigilance programmeAbhinav BhathejaNo ratings yet
- Abhijath Documents Those Who Are Preparing For Interview 1664876843Document36 pagesAbhijath Documents Those Who Are Preparing For Interview 1664876843naidujNo ratings yet
- Pharmacovigilance EnglishDocument4 pagesPharmacovigilance EnglishImmad AlviNo ratings yet
- Pharmacovigilance Programme of India: CommentaryDocument13 pagesPharmacovigilance Programme of India: CommentaryBhupesh KumarNo ratings yet
- Pharmacovigilance: Need and Future Prospective in Herbal and Ayurvedic MedicinesDocument5 pagesPharmacovigilance: Need and Future Prospective in Herbal and Ayurvedic MedicinesBhavana GangurdeNo ratings yet
- PHARMACOVIGILANCEDocument28 pagesPHARMACOVIGILANCENosheen JavedNo ratings yet
- Ad Hoc Data SourcesDocument11 pagesAd Hoc Data SourcesDona BasilNo ratings yet
- Ad Hoc Data SourcesDocument11 pagesAd Hoc Data SourcesVINAY KUMAR100% (1)
- Systematic Approach in Reporting and Monitoring of Adverse Drug ReactionDocument7 pagesSystematic Approach in Reporting and Monitoring of Adverse Drug ReactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pharmacovigilance Introduction and TerminologiesDocument50 pagesPharmacovigilance Introduction and TerminologiesSyama J.S100% (2)
- A_Case_Study_of_Pharmacovigilance_in_Nigeria_ChallDocument5 pagesA_Case_Study_of_Pharmacovigilance_in_Nigeria_ChallasresmenNo ratings yet
- Pharmacovigilance and Clinical ResearchDocument47 pagesPharmacovigilance and Clinical Researchdadimma100% (1)
- SMB5401Document288 pagesSMB5401funnymemesworld2023No ratings yet
- Guidelines On Pharmacovigilance 1Document20 pagesGuidelines On Pharmacovigilance 1NatashaNo ratings yet
- Detection, Verification, and Quantification of Adverse Drug ReactionsDocument4 pagesDetection, Verification, and Quantification of Adverse Drug ReactionsgabyvaleNo ratings yet
- Pharmacovigilance Topic 2 CAMDocument9 pagesPharmacovigilance Topic 2 CAMedwin osiyelNo ratings yet
- Pharmacovigilance in India - A PerspectiveDocument4 pagesPharmacovigilance in India - A PerspectiveVijay Venkatraman JanarthananNo ratings yet
- Philippine Medicine PolicyDocument7 pagesPhilippine Medicine PolicyMissy OrgelaNo ratings yet
- For Partial Fulfilment of The Requirement For TheDocument45 pagesFor Partial Fulfilment of The Requirement For ThesalmanNo ratings yet
- Notes To PharmacovigilanceDocument58 pagesNotes To Pharmacovigilancejay100% (1)
- Pharmacovigilance - Review ArticleDocument4 pagesPharmacovigilance - Review ArticleKishore100% (1)
- Pharmacovigilance - KhimyaDocument22 pagesPharmacovigilance - KhimyakimNo ratings yet
- Pharmacovigilance CentreDocument15 pagesPharmacovigilance Centrerutheaster29No ratings yet
- Imp of PVDocument5 pagesImp of PVrr48843No ratings yet
- Medication Safety: Improving Public HealthDocument6 pagesMedication Safety: Improving Public HealthViee Nie SfarmNo ratings yet
- Pharmacovigilance Risk Mitigation Plans PDFDocument11 pagesPharmacovigilance Risk Mitigation Plans PDFVladimir KostovskiNo ratings yet
- What Is Pharmacovigilance and Why Is It ImportantDocument8 pagesWhat Is Pharmacovigilance and Why Is It ImportantArunendu MajiNo ratings yet
- Covigilance Question BankDocument44 pagesCovigilance Question BankDrx Rinku Kundu0% (1)
- PV Minimum Requirements 2010 2Document2 pagesPV Minimum Requirements 2010 2KishoreNo ratings yet
- PV in Developing Countries - CrispDocument4 pagesPV in Developing Countries - CrispVandana ReddyNo ratings yet
- PV PDFDocument3 pagesPV PDFDAMBALENo ratings yet
- Underreporting of Adverse Drug Reaction: A Critical Issue in HealthcareDocument6 pagesUnderreporting of Adverse Drug Reaction: A Critical Issue in HealthcareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Falsified Medicines and The Global Public's Health: InsightDocument24 pagesFalsified Medicines and The Global Public's Health: InsightAndromeda KalapoyoNo ratings yet
- Role of Pharmacovigilance in Drug Discovery and Post Marketing SurveillanceDocument7 pagesRole of Pharmacovigilance in Drug Discovery and Post Marketing SurveillanceEditor IJTSRDNo ratings yet
- Consumer ReportingDocument36 pagesConsumer ReportingJai RamNo ratings yet
- KeywordsDocument12 pagesKeywordsaadrika negiNo ratings yet
- Role of The Pharmacist in Antimicrobial Stewardship: Rachel Fortin, Pharmd, BcpsDocument2 pagesRole of The Pharmacist in Antimicrobial Stewardship: Rachel Fortin, Pharmd, BcpsSih AtiiNo ratings yet
- By BhartiDocument17 pagesBy BhartikundagolNo ratings yet
- Clinical Pharmacy: Sohan Patel Assistant Professor, Modasa, Gujarat, IndiaDocument56 pagesClinical Pharmacy: Sohan Patel Assistant Professor, Modasa, Gujarat, IndiaRaju NiraulaNo ratings yet
- WHO International Drug MonitoringDocument23 pagesWHO International Drug MonitoringVasavi ChittemreddyNo ratings yet
- IndianJPharmacol40728-3361566 005601Document4 pagesIndianJPharmacol40728-3361566 005601rr48843No ratings yet
- Increasing Adverse Drug Reaction Reporting-How Can We Do BetterDocument15 pagesIncreasing Adverse Drug Reaction Reporting-How Can We Do Betterstacie010429No ratings yet
- Medication SafetyDocument180 pagesMedication SafetyAengus JoyceNo ratings yet
- Medicines Promotion: Assessing The Nature, Extent and Impact of RegulationDocument38 pagesMedicines Promotion: Assessing The Nature, Extent and Impact of RegulationAsmitaNo ratings yet
- Chapter 11 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Document2 pagesChapter 11 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Mobeen AhmedNo ratings yet
- Pharmacovigilance Strategy: Opportunities For Cross-National LearningDocument5 pagesPharmacovigilance Strategy: Opportunities For Cross-National LearningJOSE HUARCAYA ROJASNo ratings yet
- PV - RamDocument7 pagesPV - RamAura Anaya HernándezNo ratings yet
- 2000-WHO Drug Information Vol. 14 - No. 4 PDFDocument79 pages2000-WHO Drug Information Vol. 14 - No. 4 PDFAngela Castro RNo ratings yet
- Brit J Clinical Pharma - 2021 - Kiguba - Pharmacovigilance in Low and Middle Income Countries A Review With ParticularDocument19 pagesBrit J Clinical Pharma - 2021 - Kiguba - Pharmacovigilance in Low and Middle Income Countries A Review With ParticularlizaNo ratings yet
- Post Marketing Surveillance and PharmacoepidemiologyDocument7 pagesPost Marketing Surveillance and PharmacoepidemiologyEditor IJTSRDNo ratings yet
- Factors Affecting Medical Laboratory Science StudeDocument9 pagesFactors Affecting Medical Laboratory Science StudeAbbey Joy CollanoNo ratings yet
- Mary Rose T. Cerdenia: ObjectiveDocument3 pagesMary Rose T. Cerdenia: ObjectiveAbbey Joy CollanoNo ratings yet
- Cornelissen (5683823) ThesisDocument48 pagesCornelissen (5683823) ThesisAbbey Joy CollanoNo ratings yet
- Freshwater Resources and Water PollutionDocument61 pagesFreshwater Resources and Water PollutionAbbey Joy Collano100% (1)
- Service-Capability Checklist For General Clinical Laboratory - AO2021-0037Document6 pagesService-Capability Checklist For General Clinical Laboratory - AO2021-0037Abbey Joy CollanoNo ratings yet
- Unmet Needs and Coping Mechanisms Among Community-Dwelling Senior Citizens in The Philippines: A Qualitative StudyDocument16 pagesUnmet Needs and Coping Mechanisms Among Community-Dwelling Senior Citizens in The Philippines: A Qualitative StudyAbbey Joy CollanoNo ratings yet
- Cavite Mutiny 2Document50 pagesCavite Mutiny 2Abbey Joy CollanoNo ratings yet
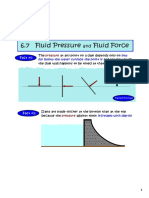
- 6.7 Fluid Pressure Fluid Force: Fact #1Document9 pages6.7 Fluid Pressure Fluid Force: Fact #1Abbey Joy CollanoNo ratings yet
- CH 14Document26 pagesCH 14Abbey Joy CollanoNo ratings yet
- 12 USP 2232 Elemental Contaminants in Dietary Supplements KGDocument14 pages12 USP 2232 Elemental Contaminants in Dietary Supplements KGAbbey Joy CollanoNo ratings yet
- 6.4: Physics Applications - Work, Force, and Pressure: Skills To DevelopDocument8 pages6.4: Physics Applications - Work, Force, and Pressure: Skills To DevelopAbbey Joy CollanoNo ratings yet
- Two-Sample T-Tests Assuming Equal VarianceDocument19 pagesTwo-Sample T-Tests Assuming Equal VarianceAbbey Joy CollanoNo ratings yet
- ViewPageProof CNSNS 4511Document21 pagesViewPageProof CNSNS 4511Abbey Joy CollanoNo ratings yet
- 457 PDFDocument8 pages457 PDFAbbey Joy CollanoNo ratings yet
- DOH Annual CalendarDocument1 pageDOH Annual CalendarBoni G. PajeNo ratings yet
- Analytical Exposition Text: By: Ariful SukronDocument8 pagesAnalytical Exposition Text: By: Ariful SukronAriful SukronNo ratings yet
- TractionDocument11 pagesTractionDenalyn Ann TormoNo ratings yet
- Implications of Demographics of AgingDocument5 pagesImplications of Demographics of AgingAndrei SubidoNo ratings yet
- Nestle India & Its Resililent SpiritDocument15 pagesNestle India & Its Resililent SpiritPrerna RathiNo ratings yet
- STEMI Clinical PathwayDocument1 pageSTEMI Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- A Systematic Review of Approaches For Continuous Quality Improvement Capacity-BuildingDocument8 pagesA Systematic Review of Approaches For Continuous Quality Improvement Capacity-Building'Amel'AyuRizkyAmeliyahNo ratings yet
- Bba Ii Sem HRD Unit 4 Part 2 Stress Management: Definition and Characteristics of StressDocument3 pagesBba Ii Sem HRD Unit 4 Part 2 Stress Management: Definition and Characteristics of StressBina SaxenaNo ratings yet
- 08 OHS Journal Aug 2012Document60 pages08 OHS Journal Aug 2012NazirAhmadBashiriNo ratings yet
- Myanmar Health Assistant Association Vacancy Announcement (VA-057/2021 MHAA-HR)Document3 pagesMyanmar Health Assistant Association Vacancy Announcement (VA-057/2021 MHAA-HR)MNo ratings yet
- Stress Among Charge NursesDocument10 pagesStress Among Charge NursesRey AllanNo ratings yet
- CXC Social Studies Sba 2023Document27 pagesCXC Social Studies Sba 2023David DillonNo ratings yet
- The Things They CarriedDocument2 pagesThe Things They Carriedapi-513974372No ratings yet
- Blood TransfucionDocument2 pagesBlood TransfucionShreyas WalvekarNo ratings yet
- PG CQ Phase 1 Collegewise - RevisedDocument54 pagesPG CQ Phase 1 Collegewise - Revisedmanmohansai bacheNo ratings yet
- Public Perceptions of Arguments Supporting and OpposingDocument23 pagesPublic Perceptions of Arguments Supporting and OpposingmafmortensonNo ratings yet
- Activity Desig FINAL SPORTS AND ARTS 1Document4 pagesActivity Desig FINAL SPORTS AND ARTS 1Marc QuiaNo ratings yet
- Attitude Towards Second Hand Smoke, Smoking and QuitingDocument5 pagesAttitude Towards Second Hand Smoke, Smoking and QuitingBaonganNo ratings yet
- Kinesiology Taping Theory and ApplicationDocument8 pagesKinesiology Taping Theory and Applicationtaxel00% (1)
- Procedures RationaleDocument3 pagesProcedures RationaleJamaica Leslie NovenoNo ratings yet
- Ozo Hand Sanitizer Spec Sheet Rev.5Document1 pageOzo Hand Sanitizer Spec Sheet Rev.5bernardo vergaraNo ratings yet
- INDIA - NRHM Common Review Mission - Fifth ReportDocument252 pagesINDIA - NRHM Common Review Mission - Fifth ReportKaushik BanerjeeNo ratings yet
- Portrayal of Underprivileged Children: Problem of Child Labour in Lost Spring: Stories of Lost Childhood by Anees JungDocument4 pagesPortrayal of Underprivileged Children: Problem of Child Labour in Lost Spring: Stories of Lost Childhood by Anees JungIJELS Research JournalNo ratings yet
- Indian Nutraceutical IndustryDocument64 pagesIndian Nutraceutical Industryhariom100% (2)
- Hse Induction: KYK Analysis of Potentially Hazardous Area (JSA)Document1 pageHse Induction: KYK Analysis of Potentially Hazardous Area (JSA)teman k3No ratings yet