Download as pdf or txt
You might also like
- The AAS Personal StatementDocument3 pagesThe AAS Personal StatementRetno Suminar100% (3)
- ATT - 1404901736356 - Workforce Free Test Questions - PDF 2Document5 pagesATT - 1404901736356 - Workforce Free Test Questions - PDF 2Oluwaseun Alowonle IfekoyaNo ratings yet
- TEA-CCRDA Narrative ReportDocument12 pagesTEA-CCRDA Narrative ReportTEA Executive DirectorNo ratings yet
- Final Program Plan 634Document8 pagesFinal Program Plan 634api-300887059No ratings yet
- HSC 402 ImplementationplanDocument4 pagesHSC 402 Implementationplanapi-356117299No ratings yet
- HSC 581 CurriculumDocument9 pagesHSC 581 Curriculumapi-743588712No ratings yet
- Activity Report (Training On HIV Counseling and Testing - June 29 - July 2, 2023)Document6 pagesActivity Report (Training On HIV Counseling and Testing - June 29 - July 2, 2023)Angelica GementizaNo ratings yet
- HLTH 634 Health Program Plan OutlineDocument8 pagesHLTH 634 Health Program Plan Outlineapi-376803951No ratings yet
- Positive Interventions: Vital To HIV PreventionDocument35 pagesPositive Interventions: Vital To HIV PreventioneramossotoNo ratings yet
- NSTP Project Proposal FinalDocument7 pagesNSTP Project Proposal FinalPamela Joyce RiambonNo ratings yet
- Article Critique 1Document3 pagesArticle Critique 1api-642711495No ratings yet
- ToRs SHM Zvandiri Endline EvaluationDocument6 pagesToRs SHM Zvandiri Endline Evaluationraymondkaridza5No ratings yet
- VCT ManualDocument70 pagesVCT ManualNay Lin HtikeNo ratings yet
- 1 Introduction BCC PDFDocument4 pages1 Introduction BCC PDFmkmznsNo ratings yet
- Focal PersonDocument13 pagesFocal PersonkenyapeeredNo ratings yet
- Literature Review On Hiv Counselling and TestingDocument4 pagesLiterature Review On Hiv Counselling and Testingwopugemep0h3100% (1)
- Student Mental Health & Peer-Support Program (MHAPS) : 9th February 2015 Edward Pinkney, Hong Kong UniversityDocument13 pagesStudent Mental Health & Peer-Support Program (MHAPS) : 9th February 2015 Edward Pinkney, Hong Kong UniversityEd PinkneyNo ratings yet
- Lecture Eleven Prevention of HIV InfectionDocument8 pagesLecture Eleven Prevention of HIV InfectionMaraka MichaelNo ratings yet
- Behaviour Change CommunicationDocument5 pagesBehaviour Change CommunicationluttomiayvonneNo ratings yet
- Hiv Testing and Counselling (HTC)Document12 pagesHiv Testing and Counselling (HTC)iammathetaNo ratings yet
- Intervention StrategyDocument2 pagesIntervention StrategyAlyssaNo ratings yet
- Step 1: Choose A Program To EvaluateDocument4 pagesStep 1: Choose A Program To Evaluateapi-340543995No ratings yet
- Discuss and Define Community-Based ResearchDocument11 pagesDiscuss and Define Community-Based ResearchashNo ratings yet
- hsc435 ProgramkaylamartinezDocument11 pageshsc435 Programkaylamartinezapi-404291045No ratings yet
- HSC 421 Group PresentationDocument21 pagesHSC 421 Group Presentationapi-294418947No ratings yet
- Rapid PEER Study To Strengthen The Injecting Drug Users' Quality of Life ProgrammeDocument88 pagesRapid PEER Study To Strengthen The Injecting Drug Users' Quality of Life ProgrammePascal TanguayNo ratings yet
- E Portfolio Part 7Document6 pagesE Portfolio Part 7api-308280151No ratings yet
- DONE Research Questions W - o ValidationDocument6 pagesDONE Research Questions W - o ValidationCloyd VillegasNo ratings yet
- 224 Filename Hiv Adolescents 02Document117 pages224 Filename Hiv Adolescents 02Farah MarisNo ratings yet
- Reach People With AidsDocument6 pagesReach People With AidsLito GallegoNo ratings yet
- Public Service Announcement ProposalDocument5 pagesPublic Service Announcement ProposalGerard JuntillaNo ratings yet
- Increasing Youth Safety and Responsible Behavior Online: Putting in Place Programs That Work.Document14 pagesIncreasing Youth Safety and Responsible Behavior Online: Putting in Place Programs That Work.aspentaskforceNo ratings yet
- Becoming A Responsible TeenDocument5 pagesBecoming A Responsible TeenAmir Iejie100% (1)
- Anubhav - Assignment FLCDocument14 pagesAnubhav - Assignment FLCTREESANo ratings yet
- Project To Raise Health Awareness Among Youngsters: Hiv/AidsDocument10 pagesProject To Raise Health Awareness Among Youngsters: Hiv/AidsRussline PacquingNo ratings yet
- Aids and DevelopmentDocument7 pagesAids and DevelopmentHonorebel MajokaNo ratings yet
- ACKNOWLEGDEMENTDocument10 pagesACKNOWLEGDEMENTswapans871No ratings yet
- Qi ProjectDocument14 pagesQi Projectapi-641561231No ratings yet
- Blog 5 New ReleaseDocument3 pagesBlog 5 New Releaseapi-323496212No ratings yet
- Week 1: ProgramsDocument21 pagesWeek 1: ProgramsRussell HartNo ratings yet
- What Is A Monitoring and Evaluation PlanDocument9 pagesWhat Is A Monitoring and Evaluation PlanTran Linh ThanhNo ratings yet
- Uts Advocacy PaperDocument11 pagesUts Advocacy PaperPlu AldiniNo ratings yet
- Deferentiated CareDocument5 pagesDeferentiated CarebaisonjoeNo ratings yet
- Writing Good Success StoriesDocument47 pagesWriting Good Success StoriesNinad JhalaNo ratings yet
- Emily Chahalis Eliza Broadbent Paola Donoso Lexi Sayer Team Innovation Pitch Fall 2020Document3 pagesEmily Chahalis Eliza Broadbent Paola Donoso Lexi Sayer Team Innovation Pitch Fall 2020Paz DonosoNo ratings yet
- Survey Report FinalDocument19 pagesSurvey Report Finalessyl saïdiNo ratings yet
- Monitoring HIV-AIDS Programs (Participant) - Module 7Document9 pagesMonitoring HIV-AIDS Programs (Participant) - Module 7Yuga MasayuNo ratings yet
- Quantitative Study ProposalDocument6 pagesQuantitative Study Proposalapi-663958474No ratings yet
- Essays For CSCDocument4 pagesEssays For CSCanonymous machineNo ratings yet
- Advocating For The Nursing RoleDocument6 pagesAdvocating For The Nursing Rolemp1757100% (1)
- Example of Acceptability StudyDocument10 pagesExample of Acceptability StudyJennelie jandusayNo ratings yet
- Cur 528 Week 4 Signature Assignment Planning A Needs AssessmentDocument8 pagesCur 528 Week 4 Signature Assignment Planning A Needs Assessmentapi-528349363No ratings yet
- Successful HIV Prevention Programming For HIV-Positive MSMDocument60 pagesSuccessful HIV Prevention Programming For HIV-Positive MSMeramossotoNo ratings yet
- The Internet and Health Promotion: Current Issues, Trends and InterventionsDocument37 pagesThe Internet and Health Promotion: Current Issues, Trends and InterventionsJijeesh GangadharanNo ratings yet
- HIDTA Implementation Guide 3 18 16Document5 pagesHIDTA Implementation Guide 3 18 16habibiharoon9No ratings yet
- HSM200 FeedbackDocument37 pagesHSM200 FeedbackMoreen WachukaNo ratings yet
- Corporate Social Responsibility Project Proposal Part I-Overview of The Societal ProblemsDocument7 pagesCorporate Social Responsibility Project Proposal Part I-Overview of The Societal ProblemsJusteen Rodriguez JuatasNo ratings yet
- Course 710.709B JChhim WHaynes 4.6.21 Methods PaperDocument8 pagesCourse 710.709B JChhim WHaynes 4.6.21 Methods PaperWendy DixonNo ratings yet
- Pr1 DefenseDocument4 pagesPr1 DefenseJecka PalabayNo ratings yet
- Building a Safepath: from Confusion to Clarity: Facilitator’s GuideFrom EverandBuilding a Safepath: from Confusion to Clarity: Facilitator’s GuideNo ratings yet
- The Business of Nur$ing: Telemedicine, DEA and FPA guidelines, A Toolkit for Nurse Practitioners Vol. 2From EverandThe Business of Nur$ing: Telemedicine, DEA and FPA guidelines, A Toolkit for Nurse Practitioners Vol. 2No ratings yet
- Updated Resume April 2020Document1 pageUpdated Resume April 2020api-502687231No ratings yet
- Scope and Sequence Chung Ford Madrigal Soto Wager YaoDocument4 pagesScope and Sequence Chung Ford Madrigal Soto Wager Yaoapi-502687231No ratings yet
- Budget JustificationDocument6 pagesBudget Justificationapi-502687231No ratings yet
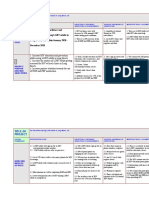
- HSC 435 Final Draft LogframeDocument4 pagesHSC 435 Final Draft Logframeapi-502687231No ratings yet
- HSC 430 Childhood Disease PaperDocument10 pagesHSC 430 Childhood Disease Paperapi-502687231No ratings yet
- HSC 421 Research PaperDocument13 pagesHSC 421 Research Paperapi-502687231No ratings yet
- Maharashtra Educational Institutions Regulation of Collection of Fee Act 2011 PDFDocument19 pagesMaharashtra Educational Institutions Regulation of Collection of Fee Act 2011 PDFSakshi VadatkarNo ratings yet
- Nutritional Status and Associated Factors in Under-Five Children of RawalpindiDocument5 pagesNutritional Status and Associated Factors in Under-Five Children of RawalpindiMarya Fitri02No ratings yet
- Quality of Work Life With Special Reference To Academic SectorDocument4 pagesQuality of Work Life With Special Reference To Academic Sectoryashika swamiNo ratings yet
- Harmony in Family and Society 87Document11 pagesHarmony in Family and Society 87Jasleen BoparaiNo ratings yet
- Daily InquirerDocument5 pagesDaily InquirerAlleihs GardoceNo ratings yet
- Ignorance Thesis StatementDocument8 pagesIgnorance Thesis StatementLisa Graves100% (2)
- Memorandum: United States Department of EducationDocument3 pagesMemorandum: United States Department of EducationKevinOhlandtNo ratings yet
- MYP 3 SA - Genetics - Crit A and DDocument5 pagesMYP 3 SA - Genetics - Crit A and Djaivik230No ratings yet
- Health Educ QuizDocument3 pagesHealth Educ QuizLois DanielleNo ratings yet
- Are Legendary Hominoids Worth Looking For?: Views From Ethnobiology and PalaeoanthropologyDocument4 pagesAre Legendary Hominoids Worth Looking For?: Views From Ethnobiology and PalaeoanthropologyElisa CazorlaNo ratings yet
- Exercise of CaptionDocument5 pagesExercise of CaptionMei Letta21No ratings yet
- MÃ ĐỀ 01Document4 pagesMÃ ĐỀ 01Kiet HoangNo ratings yet
- BPSYCH11 - Chapter 1 - Introduction To Culture PsychologyDocument10 pagesBPSYCH11 - Chapter 1 - Introduction To Culture PsychologyJEDION JOSIAH JASANo ratings yet
- How To Be Good SecretaryDocument7 pagesHow To Be Good Secretarysalma dhiyya saputriNo ratings yet
- Syllabus Ugba102b sp2021Document5 pagesSyllabus Ugba102b sp2021Gwendolyn Chloe PurnamaNo ratings yet
- #411178596 - Cultural Humility in PracticeDocument7 pages#411178596 - Cultural Humility in PracticeTimothyNo ratings yet
- Contrast Two or More Classification Systems For Abnormal BehaviorDocument3 pagesContrast Two or More Classification Systems For Abnormal BehaviorSerena MohajerNo ratings yet
- Utilize Quality TrimmingsDocument8 pagesUtilize Quality Trimmingsjinky jemoyaNo ratings yet
- The Meaning and Scope of Administration Ans SupervisionDocument27 pagesThe Meaning and Scope of Administration Ans SupervisionAbigailFelixMesina100% (1)
- Hospital ListDocument10 pagesHospital ListHercules SafesNo ratings yet
- Emotional Intelligence and Work Life Balance.: P.Shylaja, Dr. CH - Jayasankara PrasadDocument4 pagesEmotional Intelligence and Work Life Balance.: P.Shylaja, Dr. CH - Jayasankara PrasadkomalNo ratings yet
- Shri Sangameshwar Arts, Commerce, Bca, BSC, College, Chadchan - 586 205Document5 pagesShri Sangameshwar Arts, Commerce, Bca, BSC, College, Chadchan - 586 205Md Izaz H DakhaniNo ratings yet
- Seminar Report 2023Document14 pagesSeminar Report 2023Akash TaradaleNo ratings yet
- IBPS AFO Syllabus 2Document3 pagesIBPS AFO Syllabus 2deepak palNo ratings yet
- The Scoutmaster - HandbookDocument201 pagesThe Scoutmaster - HandbooktadeumatasNo ratings yet
- The Relationship of Students' Learning Styles and Academic PerformanceDocument7 pagesThe Relationship of Students' Learning Styles and Academic PerformanceAct SriNo ratings yet
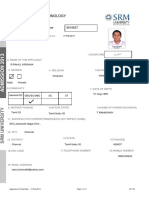
- SRM ApplicationDocument2 pagesSRM ApplicationNirmal KumarNo ratings yet
- Risk Management in IoT ImplementationDocument4 pagesRisk Management in IoT ImplementationvsureshaNo ratings yet
- Module 3: Counsel The Hiv Positive Mother: Imci Complementary Course On Hiv/AidsDocument32 pagesModule 3: Counsel The Hiv Positive Mother: Imci Complementary Course On Hiv/AidsKanaka KNo ratings yet