Download as docx, pdf, or txt
You might also like
- Ironman 70 - 3 Base Training Plan PDFDocument31 pagesIronman 70 - 3 Base Training Plan PDFCarlos De Veer100% (3)
- MMA - 1 Week Workout PlanDocument3 pagesMMA - 1 Week Workout PlannehapanditayinNo ratings yet
- NCP - Acute Pain Related To Presence of Postoperative Surgical IncisionDocument2 pagesNCP - Acute Pain Related To Presence of Postoperative Surgical IncisionRene John Francisco90% (10)
- Strength and Power Training For Older Adults: A Harvard Medical SchoolDocument53 pagesStrength and Power Training For Older Adults: A Harvard Medical SchoolMurray Wickwire75% (4)
- Septic Arthritis NCPDocument3 pagesSeptic Arthritis NCPMae Therese B. MAGNO0% (1)
- NCP - Acute PainDocument3 pagesNCP - Acute PainRene John Francisco0% (1)
- M&F ULTRA Month3 PrintDocument11 pagesM&F ULTRA Month3 Printap100% (1)
- Get Ripped, Stay Big - 365 Circuit Trainer With Julien GreauxDocument7 pagesGet Ripped, Stay Big - 365 Circuit Trainer With Julien Greauxmohamed ali100% (1)
- Chronic Pain (Nyeri Kronis)Document10 pagesChronic Pain (Nyeri Kronis)Eki MegaraniNo ratings yet
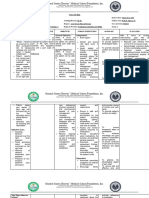
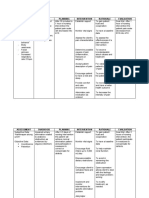
- General Santos Doctors' Medical School Foundation Inc. NCM: Rle ExposureDocument3 pagesGeneral Santos Doctors' Medical School Foundation Inc. NCM: Rle ExposureEloisa Joy MaquidatoNo ratings yet
- 利用纳米技术通过新型无药局部止痛贴片改善疼痛和功能Document20 pages利用纳米技术通过新型无药局部止痛贴片改善疼痛和功能shexinyejianNo ratings yet
- Subjective DataDocument1 pageSubjective DataKevean Kimi LimNo ratings yet
- Review of Different Methods Used For Clinical Recognition and Assessment of Pain in Dogs and CatsDocument12 pagesReview of Different Methods Used For Clinical Recognition and Assessment of Pain in Dogs and CatsAna Paula GaldinoNo ratings yet
- NCP Format 1Document4 pagesNCP Format 1Kylle AlimosaNo ratings yet
- NCP Sir EzerDocument5 pagesNCP Sir EzerJamaeca AbesamisNo ratings yet
- Nursing Care Plan: Cebu Normal UniversityDocument5 pagesNursing Care Plan: Cebu Normal UniversityFaye Andrea FranciscoNo ratings yet
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- Table 30.5 List of Behavioural Pain Assessment Scales: Evidence-Informed PracticeDocument8 pagesTable 30.5 List of Behavioural Pain Assessment Scales: Evidence-Informed Practicerahtu suzi ameliaNo ratings yet
- Nursing Pain PolicyDocument9 pagesNursing Pain Policyapi-518235690No ratings yet
- Subjective Cues: Short Term Goal: Short Term GoalDocument4 pagesSubjective Cues: Short Term Goal: Short Term GoalLarr SumalpongNo ratings yet
- Running Head: Applied Behavioral Pain Management Strategies 1Document5 pagesRunning Head: Applied Behavioral Pain Management Strategies 1george mulaaNo ratings yet
- Preoperative Pain Management Education An Evidence-Based Practice ProjectDocument8 pagesPreoperative Pain Management Education An Evidence-Based Practice Projectfachrudin arNo ratings yet
- The Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementDocument4 pagesThe Argument For Enhanced Use of Complementary and Alternative Therapies in Chronic Pain ManagementquadrospauloNo ratings yet
- Nursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale EvaluationDocument6 pagesNursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale EvaluationNajla Kaye PerezNo ratings yet
- Qst. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingDocument5 pagesQst. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingChristian UmosoNo ratings yet
- Nursing Pain PolicyDocument9 pagesNursing Pain Policyapi-518252452No ratings yet
- Austria - NCP - ObDocument2 pagesAustria - NCP - ObRiczhelle AustriaNo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Nursing Care Plan: Student's Name: ID: Course Name: SettingDocument3 pagesNursing Care Plan: Student's Name: ID: Course Name: SettingnjoodNo ratings yet
- Format For CAse AnalysisDocument2 pagesFormat For CAse AnalysisJoeyca Shien PiolNo ratings yet
- Care Plan PostpartumDocument2 pagesCare Plan PostpartumSiwei Yang100% (1)
- The Impact of Combining Pain Education Strategies With Physical TherapyDocument13 pagesThe Impact of Combining Pain Education Strategies With Physical Therapypedro.herreraNo ratings yet
- Artikel Pain MenegementDocument19 pagesArtikel Pain Menegementrizki heriyadiNo ratings yet
- AAFP NyeriDocument40 pagesAAFP Nyeriscan resepNo ratings yet
- St. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingDocument5 pagesSt. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingChristian UmosoNo ratings yet
- Scientific BasisDocument3 pagesScientific BasissecretNo ratings yet
- Nursing Care Plan Acute Pain: Assessment Evaluation PlanningDocument9 pagesNursing Care Plan Acute Pain: Assessment Evaluation PlanningAngelokeizer GavinoNo ratings yet
- 23 - RA-Dmytro-Ped Pain - HP WordDocument10 pages23 - RA-Dmytro-Ped Pain - HP WordaldybebikaNo ratings yet
- Acute Pain Nursing Diagnosis & Care Plan - NurseslabsDocument1 pageAcute Pain Nursing Diagnosis & Care Plan - NurseslabsShimaa Al SiyabiNo ratings yet
- Optimizing Acute Pain Management: A Guide To Multimodal Analgesia and Quality ImprovementDocument10 pagesOptimizing Acute Pain Management: A Guide To Multimodal Analgesia and Quality ImprovementAgus HendraNo ratings yet
- New HTP Neuro Acute PainDocument5 pagesNew HTP Neuro Acute PainddsadNo ratings yet
- CaseDocument3 pagesCasebLessy_july16No ratings yet
- Nursing Diagnosis: Acute Pain: NANDA Definition: Pain Is Whatever The ExperiencingDocument13 pagesNursing Diagnosis: Acute Pain: NANDA Definition: Pain Is Whatever The Experiencingasmika danaNo ratings yet
- Acute Pain POCDocument3 pagesAcute Pain POCHeidi Atkinson ThomasNo ratings yet
- Psychological Aspects of Persistent Pain Current State of The ScienceDocument17 pagesPsychological Aspects of Persistent Pain Current State of The Scienceraquelalcides1412No ratings yet
- Little Nursing Plan of Care - FinalDocument5 pagesLittle Nursing Plan of Care - Finalapi-541785084No ratings yet
- By: Novi Ayun N Uswatun Nisa Rita Cahyanti Yesi DevitasariDocument8 pagesBy: Novi Ayun N Uswatun Nisa Rita Cahyanti Yesi DevitasariNophienyagigghz Luphmoepolephel Anyun'nyuntamaNo ratings yet
- Pain Management GuidelinesDocument3 pagesPain Management GuidelinesMr. BamsNo ratings yet
- Clinical Simulation Day 1 Care Plan ms3 Chest Pain SHDocument3 pagesClinical Simulation Day 1 Care Plan ms3 Chest Pain SHapi-575469761No ratings yet
- Medical-Surgical Nursing Pain Management StrategiesDocument5 pagesMedical-Surgical Nursing Pain Management StrategiesMark Russel Sean LealNo ratings yet
- Nursing Care Plan: University of San Jose-RecoletosDocument2 pagesNursing Care Plan: University of San Jose-RecoletosIvan A. EleginoNo ratings yet
- Postoperative & Critical Care Medicine: Vitebsk State Medical UniversityDocument50 pagesPostoperative & Critical Care Medicine: Vitebsk State Medical UniversitySuvini GunasekaraNo ratings yet
- Nursing Documentation ReportDocument4 pagesNursing Documentation ReportRicco Valentino CoenraadNo ratings yet
- Part #3 Nursing Problem/Goal/Interventions/Evaluation (10%) (Due Week 11)Document5 pagesPart #3 Nursing Problem/Goal/Interventions/Evaluation (10%) (Due Week 11)glenda roblesNo ratings yet
- NCP NephrolithiasisDocument3 pagesNCP NephrolithiasisMANUEL EMERSONNo ratings yet
- 2009 Pain Assessment and ManagementDocument22 pages2009 Pain Assessment and ManagementErnawa RikaNo ratings yet
- Physical Health AssignmentDocument2 pagesPhysical Health AssignmentSherry BoychukNo ratings yet
- Clin Psychology and Psychoth - 2017 - Durá Ferrandis - Confirming The Mechanisms Behind Cognitive Behavioural TherapyDocument7 pagesClin Psychology and Psychoth - 2017 - Durá Ferrandis - Confirming The Mechanisms Behind Cognitive Behavioural TherapyNatalie JaraNo ratings yet
- NCP 2BCDocument6 pagesNCP 2BCPMG BrightNo ratings yet
- 2.chronicback PainDocument9 pages2.chronicback PainRiantiara PutrizaNo ratings yet
- Pain: Current Understanding of Assessment, Management, and Treatments (An Overview of Two Monographs)Document4 pagesPain: Current Understanding of Assessment, Management, and Treatments (An Overview of Two Monographs)National Pharmaceutical Council100% (1)
- 20.more Than Pills Alternative ADocument6 pages20.more Than Pills Alternative AIrna SulistiyaniNo ratings yet
- 'Urdaneta City University College of Health Sciences: Bachelor of Science in NursingDocument4 pages'Urdaneta City University College of Health Sciences: Bachelor of Science in NursingDan Dan ManaoisNo ratings yet
- Chronic Pain NandaDocument7 pagesChronic Pain NandaJude Bello-AlvearNo ratings yet
- Pain Assessment AND Management: Mr. Swapnil Wanjari Clinical InstructorDocument27 pagesPain Assessment AND Management: Mr. Swapnil Wanjari Clinical InstructorSWAPNIL WANJARINo ratings yet
- Running Head: Program Graduate Competencies 1Document12 pagesRunning Head: Program Graduate Competencies 1api-509672908No ratings yet
- Running Head: Policy Action Plan: Health Care Disparities 1Document9 pagesRunning Head: Policy Action Plan: Health Care Disparities 1api-509672908No ratings yet
- Running Head: Computerized Provider Order Entry 1Document9 pagesRunning Head: Computerized Provider Order Entry 1api-509672908No ratings yet
- Running Head: Emotional Intelligence Leadership Theory 1Document8 pagesRunning Head: Emotional Intelligence Leadership Theory 1api-509672908No ratings yet
- Jessiembahproblem BasedresearchpaperDocument11 pagesJessiembahproblem Basedresearchpaperapi-509672908No ratings yet
- PE7-Q2 M1 IdentifyingStrengthsandWeaknessesinSkills v6Document19 pagesPE7-Q2 M1 IdentifyingStrengthsandWeaknessesinSkills v6Jeneva Rose PerezNo ratings yet
- Lesson 2 - Muscular SystemDocument7 pagesLesson 2 - Muscular SystemCherubim GimaranganNo ratings yet
- Nursing Care Plan: Subjective CuesDocument2 pagesNursing Care Plan: Subjective CuesNicole cuencosNo ratings yet
- Essentials of Nutritional Assessment and Diet Planning: HND-713 Professional DieteticsDocument36 pagesEssentials of Nutritional Assessment and Diet Planning: HND-713 Professional Dieteticssaba shahid100% (1)
- Fuel For PerformanceDocument20 pagesFuel For PerformanceMALAKIPWETKO100% (1)
- Project 000Document33 pagesProject 000Sonu JoseNo ratings yet
- TPL 6 Reading 3 WorksheetDocument3 pagesTPL 6 Reading 3 WorksheetKeluarga SuksesNo ratings yet
- Teaching Final PaperDocument11 pagesTeaching Final Paperapi-424938899No ratings yet
- Lab Report Format Physiology of ExerciseDocument11 pagesLab Report Format Physiology of Exercisetowowot594No ratings yet
- Summarizing-Grade 7 EditedDocument17 pagesSummarizing-Grade 7 EditedCeciliaNo ratings yet
- Coordinated School Health Programs - LESSON 1Document4 pagesCoordinated School Health Programs - LESSON 1Jamaica DumasNo ratings yet
- PET Health, MedicineDocument2 pagesPET Health, MedicineЛусине ХачатрянNo ratings yet
- Health Related ComponentsDocument2 pagesHealth Related ComponentsCharlotte Palingcod BaldapanNo ratings yet
- DR 01 Concept Note TemplateDocument7 pagesDR 01 Concept Note TemplatesurafelNo ratings yet
- Society: Finding The Motivation For Exercise and Fitness WithinDocument8 pagesSociety: Finding The Motivation For Exercise and Fitness WithinFabiano HenriqueNo ratings yet
- Holistic Approach To Mental HealthDocument38 pagesHolistic Approach To Mental HealthabhishekNo ratings yet
- Weiyun Chen, Ph. D., Associate Professor: Academic DegreesDocument50 pagesWeiyun Chen, Ph. D., Associate Professor: Academic DegreesArie AnggaNo ratings yet
- Benefits of CampingDocument1 pageBenefits of CampingRose Marie HermosaNo ratings yet
- Lesson 1: Personal Physical Activity InventoryDocument8 pagesLesson 1: Personal Physical Activity InventoryJopit Olavario RiveraNo ratings yet
- Introduction To Medical Surgical Nursing 6Th Edition Linton Test Bank Full Chapter PDFDocument31 pagesIntroduction To Medical Surgical Nursing 6Th Edition Linton Test Bank Full Chapter PDFschahheelpost4ogl100% (11)
- Parkinson's Disease Discharge PlanDocument2 pagesParkinson's Disease Discharge PlanCristine Joy Alarcon MonteroNo ratings yet
- The ESC Handbook of Cardiovascular Rehabilitation 2020Document225 pagesThe ESC Handbook of Cardiovascular Rehabilitation 2020Daboin ZambranoNo ratings yet
- Unit 1: The Physical Self: ExplainDocument6 pagesUnit 1: The Physical Self: ExplainELI BUSLIGNo ratings yet
- DR Sachin Patel - Morning RoutineDocument13 pagesDR Sachin Patel - Morning RoutineDimi ArchiNo ratings yet
- Answer Key 2Document8 pagesAnswer Key 2praveenNo ratings yet