
Download as pdf or txt
You might also like
- A320 Family Maintenance Concept PosterDocument1 pageA320 Family Maintenance Concept PosterKamran Khan Tareen100% (1)
- RenalDocument1 pageRenalYezin Shamoon100% (1)
- Instant Assessments for Data Tracking, Grade K: Language ArtsFrom EverandInstant Assessments for Data Tracking, Grade K: Language ArtsNo ratings yet
- BFSDocument2 pagesBFSJohnny BeeNo ratings yet
- Heavy Metals Test KitsDocument2 pagesHeavy Metals Test KitsosumexNo ratings yet
- Tooth TraumaDocument111 pagesTooth TraumaNavroop Kaur50% (2)
- Gen Path Case StudyDocument3 pagesGen Path Case Studydex7reme0% (1)
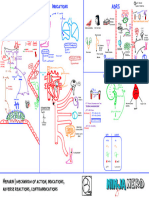
- Mind Map Sym&Parasym DrugsDocument2 pagesMind Map Sym&Parasym Drugsjitpinun.sNo ratings yet
- Angeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsDocument10 pagesAngeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsMiguel C. DolotNo ratings yet
- Online Edition - Digital AccessDocument1 pageOnline Edition - Digital Access18aw2708No ratings yet
- All Charts Final Exam 1 PDFDocument294 pagesAll Charts Final Exam 1 PDFYasir RasoolNo ratings yet
- Restaurant Risk MatrixDocument2 pagesRestaurant Risk MatrixScribdTranslationsNo ratings yet
- Patient Data - 100Document1 pagePatient Data - 100pavankn0402No ratings yet
- Nifedi-Denk 20 Retard - Nifedipine 20mg Prolonged release tablet - PILDocument2 pagesNifedi-Denk 20 Retard - Nifedipine 20mg Prolonged release tablet - PILHamadou FadimatouNo ratings yet
- IRAC Modes of ActionDocument1 pageIRAC Modes of ActionsigitNo ratings yet
- Appendix 5 Hazmat Inventory SheetDocument1 pageAppendix 5 Hazmat Inventory Sheetaldrb hospitalNo ratings yet
- Endocrine SystemDocument1 pageEndocrine SystemTin Myat SweNo ratings yet
- Permanent Plus: Engine ControlDocument1 pagePermanent Plus: Engine ControlAlanNo ratings yet
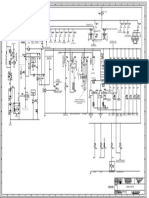
- c15 ldn01610 SchematicDocument4 pagesc15 ldn01610 SchematicJacques Van Niekerk50% (2)
- Andrew J. Cutler - Valbenazine and DeutetrabenazineDocument1 pageAndrew J. Cutler - Valbenazine and DeutetrabenazineSanty P Vásconez CalderónNo ratings yet
- HPLC FenitoinaDocument32 pagesHPLC FenitoinaJhon Murga SNo ratings yet
- PMKP Juni-Desember 19Document256 pagesPMKP Juni-Desember 19Dini RizkyNo ratings yet
- c15 Main Schematic ECM PDFDocument4 pagesc15 Main Schematic ECM PDFWill ?No ratings yet
- Night Scan Powerlite ECDDocument2 pagesNight Scan Powerlite ECDSUNIL MISHRANo ratings yet
- Batteries: Color Code For Schematic LinesDocument2 pagesBatteries: Color Code For Schematic LinesIsaac NewtonNo ratings yet
- 23 - Preoperative Patient Assessment and ManagementDocument1 page23 - Preoperative Patient Assessment and ManagementHenrique MachadoNo ratings yet
- Post-Traumatic Stress DisorderDocument1 pagePost-Traumatic Stress DisorderJoan MonzonesNo ratings yet
- Cardiovascular Pharmacology) 03 Heparin - KeyDocument1 pageCardiovascular Pharmacology) 03 Heparin - Keyhasanatiya41No ratings yet
- Amala Wellness Guide SML 922d96d0 6f29 4b8c 856e b26ff73d360fDocument2 pagesAmala Wellness Guide SML 922d96d0 6f29 4b8c 856e b26ff73d360fdouglasknight2No ratings yet
- Neuroinflammation and Alzheimers Disease PosterDocument1 pageNeuroinflammation and Alzheimers Disease PosterVincent Mora GarcisNo ratings yet
- Case PresentationDocument1 pageCase PresentationGLORY MI SHANLEY CARUMBANo ratings yet
- Siemens Healthcare Diagnostics Inc.: ADVIA Centaur XP Version 1.0.EC and 1.0.ED Test DefinitionsDocument12 pagesSiemens Healthcare Diagnostics Inc.: ADVIA Centaur XP Version 1.0.EC and 1.0.ED Test DefinitionsОлександрNo ratings yet
- De - Mavenclad - Actrims 2024 Cladrina p481Document1 pageDe - Mavenclad - Actrims 2024 Cladrina p481magdecanedaNo ratings yet
- Sample Matrix 1Document6 pagesSample Matrix 1eastNo ratings yet
- DQC24 Tableau Medicaments EN WEBDocument1 pageDQC24 Tableau Medicaments EN WEBcococooleNo ratings yet
- Ka1 Ebp 00a d7086 Iom Manual GCBDocument261 pagesKa1 Ebp 00a d7086 Iom Manual GCBLaura Callista AzahraNo ratings yet
- R&D Hazards Eval Form Ver 3.3Document13 pagesR&D Hazards Eval Form Ver 3.3dleggett5147No ratings yet
- C15 and C18 Industrial Engine Electrical System: View ADocument4 pagesC15 and C18 Industrial Engine Electrical System: View AOecox Cah Djadoel100% (2)
- PDF Hoja de Registro Anestesico Gava CompressDocument2 pagesPDF Hoja de Registro Anestesico Gava CompressEDITH NATHALY CUMBAJIN PANELUISANo ratings yet
- Fully Programmable. Ultra-Portable.: Made in ItalyDocument2 pagesFully Programmable. Ultra-Portable.: Made in ItalypsychpostersNo ratings yet
- 01 Control Structures PDFDocument22 pages01 Control Structures PDFJeff RobertNo ratings yet
- Biological PosterDocument1 pageBiological PosterAsad UllahNo ratings yet
- Cardiovascular Pharmacology] 03 Heparin - KeyDocument1 pageCardiovascular Pharmacology] 03 Heparin - KeyRubie Ann TillorNo ratings yet
- Combination Meter Combination Meter Combination MeterDocument1 pageCombination Meter Combination Meter Combination MeterDannyDDannyDNo ratings yet
- HIRADC - Pekerjaan 20 KV - PLTGU - Update 5 March 2018Document5 pagesHIRADC - Pekerjaan 20 KV - PLTGU - Update 5 March 2018ghieee100% (2)
- Dokumen - Tips Samsung GT E1200 SchematicsDocument7 pagesDokumen - Tips Samsung GT E1200 SchematicsHogir DoskyNo ratings yet
- ECU de 4 ConectoresDocument1 pageECU de 4 ConectoresHarold Rodriguez CastilloNo ratings yet
- Crt-Npc-Dmm-Hva-Dwg-Sd-Gn-33501 - Equipment Capacity Schedule 1-6Document1 pageCrt-Npc-Dmm-Hva-Dwg-Sd-Gn-33501 - Equipment Capacity Schedule 1-6Shah MuzzamilNo ratings yet
- Compare Vivix With Noni Xango MonavieDocument1 pageCompare Vivix With Noni Xango MonaviecustomhealthNo ratings yet
- DNA Repair Pathways PosterDocument1 pageDNA Repair Pathways Posterdyk2100% (1)
- Lanoxic Aps From Lanoxin DosageDocument4 pagesLanoxic Aps From Lanoxin Dosageelvie21No ratings yet
- M.4-1-001a - Mall Mechanical Services Panel Diagram P-CH-4THDocument1 pageM.4-1-001a - Mall Mechanical Services Panel Diagram P-CH-4THdiki anggriawanNo ratings yet
- Empagliflozin Metformin HCL: Jardiance Duo®Document2 pagesEmpagliflozin Metformin HCL: Jardiance Duo®Lord Carlo CabangalNo ratings yet
- ECT and A/T Indicator (1AZ-FSE) ECT and A/T Indicator (1AZ-FSE) ECT and A/T Indicator (1AZ-FSE)Document1 pageECT and A/T Indicator (1AZ-FSE) ECT and A/T Indicator (1AZ-FSE) ECT and A/T Indicator (1AZ-FSE)Luis100% (1)
- CD Radio Cassette-Corder: Specifications Troubleshooting PrecautionsDocument2 pagesCD Radio Cassette-Corder: Specifications Troubleshooting PrecautionsAliseNo ratings yet
- Oxaliplatin For Injection (Preservative-Free) 50 MG Per Vial and 100 MG Per Vial Package Leaflet - Taj PharmaDocument1 pageOxaliplatin For Injection (Preservative-Free) 50 MG Per Vial and 100 MG Per Vial Package Leaflet - Taj PharmaTAJ PHARMA — A Health Care ProviderNo ratings yet
- 994F Wheel Loader Electrical System: Cab Harness Connector and Component Location GridDocument4 pages994F Wheel Loader Electrical System: Cab Harness Connector and Component Location GridAlexis MikeNo ratings yet
- Frac Moa Poster FungicidasDocument1 pageFrac Moa Poster Fungicidaskelvin horna guiopNo ratings yet
- Frac Moa Poster March FRACDocument1 pageFrac Moa Poster March FRACEliana Garcia ValenciaNo ratings yet
- Microbiology Homework Unit III N IVDocument7 pagesMicrobiology Homework Unit III N IVYazmin CoatlNo ratings yet
- Spectrum WhiteDocument1 pageSpectrum WhitethebigfishxNo ratings yet
- Instant Assessments for Data Tracking, Grade 1: Language ArtsFrom EverandInstant Assessments for Data Tracking, Grade 1: Language ArtsNo ratings yet
- Instant Assessments for Data Tracking, Grade 1: MathFrom EverandInstant Assessments for Data Tracking, Grade 1: MathRating: 4 out of 5 stars4/5 (1)
- Inpatient Pocket Card SetDocument9 pagesInpatient Pocket Card SetJohnny BeeNo ratings yet
- Head / Hair Face Eyes Nose Oral / Throat Ears Neck: Physical Exam (Heent)Document1 pageHead / Hair Face Eyes Nose Oral / Throat Ears Neck: Physical Exam (Heent)Johnny BeeNo ratings yet
- GI Signs and SymptomsDocument40 pagesGI Signs and SymptomsJohnny BeeNo ratings yet
- Velocity-DIet 3.5.1Document75 pagesVelocity-DIet 3.5.1Johnny BeeNo ratings yet
- Ab Crunch Machine: Exercise DataDocument27 pagesAb Crunch Machine: Exercise DataJohnny BeeNo ratings yet
- ArachnidsDocument1 pageArachnidsJohnny BeeNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaDesyari SusantiNo ratings yet
- Clinical Screening Form - AgriSafe NetworkDocument4 pagesClinical Screening Form - AgriSafe NetworkAgriSafeNo ratings yet
- The Indian Journal of Pediatrics: OntentsDocument6 pagesThe Indian Journal of Pediatrics: OntentsPoldo ReinaldoNo ratings yet
- BuzzwordsDocument35 pagesBuzzwordstesta21100% (1)
- Pediatric Readiness Guidelines ChecklistDocument4 pagesPediatric Readiness Guidelines ChecklistsabirNo ratings yet
- Haematology and Biochemistry in Alpacas and Llamas: Red Blood CellsDocument6 pagesHaematology and Biochemistry in Alpacas and Llamas: Red Blood CellsDarwin Antezana De la RosaNo ratings yet
- Chapter 20bDocument6 pagesChapter 20baexillisNo ratings yet
- Impulse Control DisordersDocument20 pagesImpulse Control DisordersKenth June GenobisNo ratings yet
- SNS 1 (Circulation)Document7 pagesSNS 1 (Circulation)Dheeraj Kumar100% (1)
- 1st Internal Assessment Examination. Dept of PhysiologyDocument2 pages1st Internal Assessment Examination. Dept of PhysiologyIshan KalraNo ratings yet
- Application of The MASCC and CISNE Risk-Strati Fication Scores To Identify Low-Risk Febrile Neutropenic Patients in The Emergency DepartmentDocument10 pagesApplication of The MASCC and CISNE Risk-Strati Fication Scores To Identify Low-Risk Febrile Neutropenic Patients in The Emergency DepartmentwiraNo ratings yet
- Lactated RingersDocument3 pagesLactated RingersE100% (5)
- Healthcare Insurance From A To Z - AnderzorgDocument86 pagesHealthcare Insurance From A To Z - AnderzorgJeremySitorusNo ratings yet
- Liberty University BIOL 101 Individual Assignment 3 Complete Solutions Correct Answers KeyDocument3 pagesLiberty University BIOL 101 Individual Assignment 3 Complete Solutions Correct Answers KeyLiberty0% (1)
- Thalidomide AssignmentDocument2 pagesThalidomide AssignmentMorganNo ratings yet
- ABC of Intensive CareDocument49 pagesABC of Intensive CareCurro MirallesNo ratings yet
- Psychological DisordersDocument6 pagesPsychological DisordersDiaиa DiazNo ratings yet
- Diagnosis of Autoimmune Diseases: Presented By, S.Nagaraj, M.Sc. 3 YearDocument51 pagesDiagnosis of Autoimmune Diseases: Presented By, S.Nagaraj, M.Sc. 3 YearAzhar Clinical Laboratory TubeNo ratings yet
- AcinobacterDocument2 pagesAcinobacterAllyson Layaoen CollierNo ratings yet
- Nursing Care Plan ColostomyDocument5 pagesNursing Care Plan ColostomyCarissa Mae Tapec EstradaNo ratings yet
- Herbal MedicineDocument5 pagesHerbal MedicineParth RathodNo ratings yet
- Pharmacy Daily For Wed 05 Oct 2016 - WA Pharmacy Vax Success, End Med Review Cap Call, NSAID Heart Risk Link, Health AMPERSAND Beauty and Much MoreDocument4 pagesPharmacy Daily For Wed 05 Oct 2016 - WA Pharmacy Vax Success, End Med Review Cap Call, NSAID Heart Risk Link, Health AMPERSAND Beauty and Much MorepharmacydailyNo ratings yet
- Work Related Low Back Pain in Sedentary Railway Officials of The Age Group 30 To 60 Years at Chhatrapati Shivaji Maharaj Terminus Mumbai - A Survey StudyDocument30 pagesWork Related Low Back Pain in Sedentary Railway Officials of The Age Group 30 To 60 Years at Chhatrapati Shivaji Maharaj Terminus Mumbai - A Survey StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Anti ParkinsonsDocument4 pagesAnti ParkinsonsMichaela BernadasNo ratings yet
- Case Study - MentalDocument13 pagesCase Study - Mentalapi-353370932No ratings yet
- Medication Safety PDFDocument95 pagesMedication Safety PDFMangayarkarasi ChandrakasanNo ratings yet
- Iv Drip IsoxilanDocument1 pageIv Drip IsoxilannierbobierNo ratings yet








































![Cardiovascular Pharmacology] 03 Heparin - Key](https://imgv2-1-f.scribdassets.com/img/document/747791383/149x198/8cd3843a2c/1720070291?v=1)





















































