Download as pdf or txt
You might also like
- BR COVID Detox - Reversing Vaccine Injuries Spike Protein SheddingDocument24 pagesBR COVID Detox - Reversing Vaccine Injuries Spike Protein SheddingDaz100% (5)
- Scanter 2001Document4 pagesScanter 2001anteysNo ratings yet
- High Rise Concrete Construction Vs High Rise Steel ConstructionDocument4 pagesHigh Rise Concrete Construction Vs High Rise Steel ConstructionnanamallowNo ratings yet
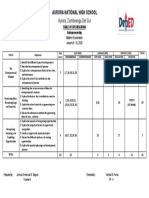
- TOS ENTREPRENEURSHIP Midterm ExamDocument1 pageTOS ENTREPRENEURSHIP Midterm Examjoshua baguio100% (2)
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal MedicineSuwandi ChangNo ratings yet
- 18th PsychiatryDocument4 pages18th PsychiatryN RoNo ratings yet
- Psychoanalysis and The Pandemic: Editor's Introduction: XX/X Mitchell WilsonDocument3 pagesPsychoanalysis and The Pandemic: Editor's Introduction: XX/X Mitchell WilsonFernanda SepulvedaNo ratings yet
- COVID-19: Tbi in Intimate Partner ViolenceDocument24 pagesCOVID-19: Tbi in Intimate Partner ViolenceAmir AliNo ratings yet
- Eng 1201 ResearchdraftpdfDocument11 pagesEng 1201 Researchdraftpdfapi-455636662No ratings yet
- Nursing Care Plan: Objective: Admission DiagnosisDocument4 pagesNursing Care Plan: Objective: Admission DiagnosisJe ZalNo ratings yet
- Fournier Gangrene in The Emergency Department: Diagnostic Dilemmas, Treatments and Current PerspectivesDocument12 pagesFournier Gangrene in The Emergency Department: Diagnostic Dilemmas, Treatments and Current PerspectivesBison_sonNo ratings yet
- Trinidad Guardian 30.10.21Document64 pagesTrinidad Guardian 30.10.21cvasurNo ratings yet
- NCP CervicalDocument4 pagesNCP CervicalZaira Kim93% (14)
- ONCO Lung Cancer PDFDocument8 pagesONCO Lung Cancer PDFkrismaevelNo ratings yet
- MR-13 LampropoulosBLHealth2003Document19 pagesMR-13 LampropoulosBLHealth2003BillalNo ratings yet
- CCChat Magazine Issue 15Document96 pagesCCChat Magazine Issue 15Min GrobNo ratings yet
- News 2010 08Document4 pagesNews 2010 08Geoff BondNo ratings yet
- Blaylock Forced0415 130Document13 pagesBlaylock Forced0415 130RAMO STEF SZEKERESNo ratings yet
- News 2010 07Document4 pagesNews 2010 07Geoff BondNo ratings yet
- The Body Economic Why Austerity Kills by David Stuckler and Sanjay Basu Allen Lane 2013 2000 HB 216pp Isbn 9781846147838Document1 pageThe Body Economic Why Austerity Kills by David Stuckler and Sanjay Basu Allen Lane 2013 2000 HB 216pp Isbn 9781846147838MedicinaNo ratings yet
- Iatrogenic Creation of New AltersDocument9 pagesIatrogenic Creation of New Altersluisrobles1977No ratings yet
- Cannabis and Schizophrenia - GrinspoonDocument1 pageCannabis and Schizophrenia - GrinspoonprojectcbdNo ratings yet
- Neuro Oncology 2023Document319 pagesNeuro Oncology 2023rvzmrkngv9No ratings yet
- Antiviral Agents: StructureDocument29 pagesAntiviral Agents: Structurevijay100% (2)
- MMfearless ForecastDocument8 pagesMMfearless ForecastKathrineMikaelaNo ratings yet
- How To Tell Patients Bad News: The Strategy of "Forecasting"Document3 pagesHow To Tell Patients Bad News: The Strategy of "Forecasting"Daniela AndradeNo ratings yet
- JURSW v7 05 DriskillDocument14 pagesJURSW v7 05 DriskillLibrary ZNo ratings yet
- Volume 8 - Superbowl WeekendDocument12 pagesVolume 8 - Superbowl WeekendpantufoNo ratings yet
- Nursing Care Plan: Precipitating FactorDocument5 pagesNursing Care Plan: Precipitating FactorJe ZalNo ratings yet
- The Carcinosin Drug Picture Donald Foubister.00248 2Document4 pagesThe Carcinosin Drug Picture Donald Foubister.00248 2Dr amit kuma50% (2)
- HIV Fear NCP - Castillo - RevisedDocument4 pagesHIV Fear NCP - Castillo - RevisedCastillo MikaellaNo ratings yet
- Neprinol StudyDocument9 pagesNeprinol StudyDadoBabylobasNo ratings yet
- 2020-04-04 New ScientistDocument62 pages2020-04-04 New ScientistSamNo ratings yet
- Respondent 1Document1 pageRespondent 1bokuto's buttcheeksNo ratings yet
- Contemporary: AgoraphobiaDocument3 pagesContemporary: AgoraphobiaArleta FordNo ratings yet
- GridDocument6 pagesGridapi-550381835No ratings yet
- The Emperor's New Drugs - Exploding The Antidepressant Myth. Irving Kirsch, PHDDocument21 pagesThe Emperor's New Drugs - Exploding The Antidepressant Myth. Irving Kirsch, PHDChrisDanger275% (4)
- Hep Foc401Document8 pagesHep Foc401samuelNo ratings yet
- Article 3Document5 pagesArticle 3VAIDEHI AGARWALNo ratings yet
- Gabbard Patients Who Hate PDFDocument12 pagesGabbard Patients Who Hate PDFBakos BenceNo ratings yet
- Research ChartDocument4 pagesResearch Chartapi-419671795No ratings yet
- PSY1020 EzineDocument54 pagesPSY1020 EzineNiela Alcelyn DeeNo ratings yet
- Manu Depression Harpers PDFDocument12 pagesManu Depression Harpers PDFluzyarmonia1No ratings yet
- Second Opinion AllDocument27 pagesSecond Opinion AllEmette E. MasseyNo ratings yet
- Case 3Document4 pagesCase 3Joselyn M. LachicaNo ratings yet
- The Luckiest People On Earth?: PsychiatristsDocument39 pagesThe Luckiest People On Earth?: Psychiatristsأيهم غزالNo ratings yet
- Nej MP 2011418Document3 pagesNej MP 2011418The Dark DreamerNo ratings yet
- Nejmp 1917203Document2 pagesNejmp 1917203Jorge RoblesNo ratings yet
- Get Your Facts, Make Your Choice: For The Health NSDocument8 pagesGet Your Facts, Make Your Choice: For The Health NSluizdasilvaazevedoNo ratings yet
- Insider Cures Jan2014Document8 pagesInsider Cures Jan2014WalterNo ratings yet
- New Generation Vaccines Seminar19Document4 pagesNew Generation Vaccines Seminar19Nerma0% (1)
- Telemedicine Neurologic Examination - American Headache SocietyDocument3 pagesTelemedicine Neurologic Examination - American Headache Societytaek123No ratings yet
- Screenshot 2021-10-18 at 09.44.27Document39 pagesScreenshot 2021-10-18 at 09.44.27Wa Ode Yulianti Asrar JayaNo ratings yet
- Mental Health Status Differences Based On Introversion Extroversion LevelsDocument1 pageMental Health Status Differences Based On Introversion Extroversion Levelsapi-551489955No ratings yet
- Books and Other Media Livres Et Autres DocumentsDocument1 pageBooks and Other Media Livres Et Autres DocumentsElena ElenaaNo ratings yet
- What To Do When Your DepressedDocument8 pagesWhat To Do When Your DepressedsiralkNo ratings yet
- Eyez2C (3) Memo - Confirmed False PositiveDocument10 pagesEyez2C (3) Memo - Confirmed False PositiveDrew GibbsNo ratings yet
- Mycoplasma and Lyme DiseaseDocument16 pagesMycoplasma and Lyme Diseaserws70100% (1)
- Evaluating Rational Fears and Bizarre Delusions in ParanoiaDocument7 pagesEvaluating Rational Fears and Bizarre Delusions in ParanoiaSandraNo ratings yet
- Smoke Mirrors and The "Disappearance" of Polio International Medical CouncilDocument11 pagesSmoke Mirrors and The "Disappearance" of Polio International Medical CouncilbNo ratings yet
- Proof The Covid-19 Jabs Should Be Stopped NowDocument2 pagesProof The Covid-19 Jabs Should Be Stopped NowDiogo MiguelNo ratings yet
- STC 2020 May 11 News A01Document1 pageSTC 2020 May 11 News A01Jessica McAllisterNo ratings yet
- 02.06.05 3-Way Valve 1240 6519 - enDocument6 pages02.06.05 3-Way Valve 1240 6519 - enabuya3kubmNo ratings yet
- Class 10 ICSE PROJECTS (SESSION 2020-2021) : Rehmat Singh)Document19 pagesClass 10 ICSE PROJECTS (SESSION 2020-2021) : Rehmat Singh)AnanyaNo ratings yet
- JeopardyDocument51 pagesJeopardyapi-509133063No ratings yet
- 18 - Creating The Persistence Layer With TopLinkDocument42 pages18 - Creating The Persistence Layer With TopLinksuresh1130No ratings yet
- D. A Framework For Every Stage of The Collection and Analysis of DataDocument4 pagesD. A Framework For Every Stage of The Collection and Analysis of DataShenna LimNo ratings yet
- Eonomics Class 6Document12 pagesEonomics Class 6mubin.pathan765No ratings yet
- Lista de Errores Tajima All ModelsDocument10 pagesLista de Errores Tajima All ModelsCesar EspinozaNo ratings yet
- Op CdmaDocument19 pagesOp Cdmarosev15No ratings yet
- Conexión para Programación de Memorias de Forma ExternaDocument24 pagesConexión para Programación de Memorias de Forma ExternaAntonii SoliizsNo ratings yet
- Hive Fleet Leviathan v3Document16 pagesHive Fleet Leviathan v3CarlosFerraoNo ratings yet
- Bosch HGS7282Document1 pageBosch HGS7282PurcellMurrayNo ratings yet
- Varivent Seat Valves Catalog 262492Document380 pagesVarivent Seat Valves Catalog 262492Thái Đạo Phạm LêNo ratings yet
- Reflective EssayDocument5 pagesReflective Essayapi-673517017No ratings yet
- Willcocks 2021b Chapter 1 PDFDocument20 pagesWillcocks 2021b Chapter 1 PDFMarc SeignarbieuxNo ratings yet
- Byk-Silclean 3700 TDS (En)Document2 pagesByk-Silclean 3700 TDS (En)feby nurvinandaNo ratings yet
- Thread Data ChartsDocument2 pagesThread Data ChartsVisan GheorgheNo ratings yet
- Risk Assessment of HVACDocument9 pagesRisk Assessment of HVACApurv Goyal100% (2)
- Nuclear ULTROL 60 CatalogDocument64 pagesNuclear ULTROL 60 CatalogRolando Sergio D'Amico InzirilloNo ratings yet
- Liebert - CRV Series Air Conditioner User Manual: V1.4 Revision Date May 28, 2012 BOM 31011886Document79 pagesLiebert - CRV Series Air Conditioner User Manual: V1.4 Revision Date May 28, 2012 BOM 31011886Dam Ngoc KienNo ratings yet
- PolB91 Lecture I IntroductionDocument13 pagesPolB91 Lecture I Introductionwqh1106515822No ratings yet
- Biofuels Annual - Tokyo - Japan - JA2022-0109Document19 pagesBiofuels Annual - Tokyo - Japan - JA2022-0109magijNo ratings yet
- MAN - CH - 2 - MCQsDocument6 pagesMAN - CH - 2 - MCQsSaquibh ShaikhNo ratings yet
- Driveline InformationDocument43 pagesDriveline InformationRodman7770% (1)
- Basic Concepts of Public Policy and TheoriesDocument36 pagesBasic Concepts of Public Policy and Theoriessaad aliNo ratings yet
- Radiative Sky Cooling: Fundamental Principles, Materials, and ApplicationsDocument41 pagesRadiative Sky Cooling: Fundamental Principles, Materials, and ApplicationsZacarias iturrietaNo ratings yet
- Aqa A Level History Coursework Mark SchemeDocument6 pagesAqa A Level History Coursework Mark Schemesyn0wok0pym3100% (2)
- Resume (Narendra Naidu)Document2 pagesResume (Narendra Naidu)venkateshNo ratings yet