
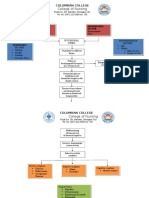
Meningitis
Meningitis
You might also like
- 2nd Term Biology Note For Ss2Document33 pages2nd Term Biology Note For Ss2Ukwuma Michael Chijioke100% (21)
- BEL Probationary Engineer Previous Papers & BEL PE Model PapersDocument6 pagesBEL Probationary Engineer Previous Papers & BEL PE Model Papersrakesh_200003No ratings yet
- I. Consciousness: State of AwarenessDocument3 pagesI. Consciousness: State of AwarenessAngeli Kristiana AlejandrinoNo ratings yet
- Case Study, Chapter 51, Assessment and Management of Patients With DiabetesDocument14 pagesCase Study, Chapter 51, Assessment and Management of Patients With DiabetesJake Yvan DizonNo ratings yet
- Chapter 5-6 Theories of AgingDocument54 pagesChapter 5-6 Theories of AgingGladz C CadaguitNo ratings yet
- Cicind Part 2Document23 pagesCicind Part 2tommaso100% (2)
- Acute Heart FailureDocument11 pagesAcute Heart FailureKhaireza KhairuddinNo ratings yet
- Acute GlomerulonephritisDocument14 pagesAcute GlomerulonephritisAnonymous D976HVjqcgNo ratings yet
- Cleviprex® (Clevidipine) Injectable Emulsion (eMC)Document7 pagesCleviprex® (Clevidipine) Injectable Emulsion (eMC)raju1559405No ratings yet
- Amniotic Fluid EmbolismDocument5 pagesAmniotic Fluid EmbolismDenim Embalzado MaghanoyNo ratings yet
- Acute Rheumatic FeverDocument9 pagesAcute Rheumatic FeverHarish Kumar KumawatNo ratings yet
- Drug Study KidneyDocument9 pagesDrug Study Kidneymcnover22No ratings yet
- Additives and Adjuvants in Animal Vaccines - Animal Wellness MagazineDocument9 pagesAdditives and Adjuvants in Animal Vaccines - Animal Wellness MagazineHansley Templeton CookNo ratings yet
- Drug Study 4C Case 2 Final PDFDocument18 pagesDrug Study 4C Case 2 Final PDFRegine Kate JuntoNo ratings yet
- Adrenal PathophysiologyDocument5 pagesAdrenal PathophysiologyditabokNo ratings yet
- Nclex Review Pneumonia COPD AsDocument11 pagesNclex Review Pneumonia COPD Asmj078No ratings yet
- Hallucinations and Hearing VoicesDocument5 pagesHallucinations and Hearing VoicesdevNo ratings yet
- Answer All The Following Short Essay Questions: (3 Questions)Document4 pagesAnswer All The Following Short Essay Questions: (3 Questions)Soad ShedeedNo ratings yet
- Complete Senses Induced Lucid Dreaming (SSILD) Guide - LDDocument10 pagesComplete Senses Induced Lucid Dreaming (SSILD) Guide - LDMarc MarcoNo ratings yet
- Type 1 Diabetes OutlineDocument2 pagesType 1 Diabetes OutlineDominique PorterNo ratings yet
- Atropine: Drug Study: NCM 106 PharmacologyDocument6 pagesAtropine: Drug Study: NCM 106 PharmacologyKevin RosalesNo ratings yet
- Drug Study TramadolDocument1 pageDrug Study Tramadolpius troy macapazNo ratings yet
- What Is AnxietyDocument13 pagesWhat Is AnxietyelaineNo ratings yet
- Burgers DiseaseDocument21 pagesBurgers DiseaseshaitabliganNo ratings yet
- Scleroza MultiplaDocument10 pagesScleroza MultiplaTudor VoinaNo ratings yet
- OBJECTIVES and PATHOPHYSIOLOGY of PHIMOSISDocument5 pagesOBJECTIVES and PATHOPHYSIOLOGY of PHIMOSISShane DamianNo ratings yet
- ArcoxiaDocument27 pagesArcoxiaClarissa Mundo OlmilloNo ratings yet
- Print Article - Glucose Tests - Glucose Test - Blood Sugar - Blood Glucose - Fasting Blood Glucose - Oral Glucose Tolerance Test - OGTT - GTT - Urine Glucose - Lab Tests OnlineDocument9 pagesPrint Article - Glucose Tests - Glucose Test - Blood Sugar - Blood Glucose - Fasting Blood Glucose - Oral Glucose Tolerance Test - OGTT - GTT - Urine Glucose - Lab Tests OnlineHinaRaviNo ratings yet
- Red EyeDocument6 pagesRed EyeafatNo ratings yet
- Thyroid StormDocument6 pagesThyroid StormCristina CenturionNo ratings yet
- Short Term Goal: After 1 Hour of Short Term Goal: After 1Document2 pagesShort Term Goal: After 1 Hour of Short Term Goal: After 1Jordz PlaciNo ratings yet
- Trans Urethral Resection of The ProstateDocument8 pagesTrans Urethral Resection of The ProstateKath RecNo ratings yet
- 1MENIEREDocument6 pages1MENIEREsunny_jr_No ratings yet
- Ms. Cynthia Bea: ProfessorDocument22 pagesMs. Cynthia Bea: ProfessorJohn Cedric Vale CruzNo ratings yet
- Basic Concept of OxygenationDocument50 pagesBasic Concept of OxygenationWiradianto PutroNo ratings yet
- Pathophysiology of ObesityDocument1 pagePathophysiology of ObesityPoldo Josef AngeloNo ratings yet
- Current Treatment of Schizoaffective Disorder According To A Neuralnetwork 2157 7099 1000441Document5 pagesCurrent Treatment of Schizoaffective Disorder According To A Neuralnetwork 2157 7099 1000441Akhsay ChandraNo ratings yet
- SchizopherniaDocument11 pagesSchizopherniaSa Ra Doh0% (1)
- The Effectiveness of Slow Deep Breathing To Decrease Blood Pressure in Hypertension - A Systematic ReviewDocument4 pagesThe Effectiveness of Slow Deep Breathing To Decrease Blood Pressure in Hypertension - A Systematic ReviewThalia NadiraNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
- PSYCHOLOGICAL ASSESSMENT REPORT (Confidential Material) : September 2018Document12 pagesPSYCHOLOGICAL ASSESSMENT REPORT (Confidential Material) : September 2018manar 9939No ratings yet
- NSG Man BulimiaDocument21 pagesNSG Man BulimiaMelodia Turqueza GandezaNo ratings yet
- Psychosis DraftDocument9 pagesPsychosis DraftCHRISTINE JOY. MOLINANo ratings yet
- CHICKEN POX Genesis CarandangDocument10 pagesCHICKEN POX Genesis CarandangGenEsis CarandangNo ratings yet
- Dissociative Identity Disorder Case Study W Mil W JeongDocument15 pagesDissociative Identity Disorder Case Study W Mil W JeongHomework PingNo ratings yet
- TBL2 - GangreneDocument53 pagesTBL2 - Gangreneyouservezeropurpose113No ratings yet
- A Meningioma Is ADocument20 pagesA Meningioma Is ASherry KingNo ratings yet
- Cerebrovascular Disease BleedDocument2 pagesCerebrovascular Disease BleedJogyBoyLunaNo ratings yet
- Nursing DiagnosisDocument16 pagesNursing DiagnosisShemie TutorNo ratings yet
- Pain in Older PatientsDocument66 pagesPain in Older PatientsmehranerezvaniNo ratings yet
- Icd 10 Kardiologi PDFDocument8 pagesIcd 10 Kardiologi PDFRestiKomalaNo ratings yet
- Nursing-Interventions MCN For Infertility MenDocument2 pagesNursing-Interventions MCN For Infertility MenRio DanteNo ratings yet
- NCM 112: Nursing Care of Sexually-Transmitted Infections, Hiv Infections & AidsDocument20 pagesNCM 112: Nursing Care of Sexually-Transmitted Infections, Hiv Infections & Aidsfebie pachecoNo ratings yet
- Polcystic Ovarian SyndromeDocument9 pagesPolcystic Ovarian SyndromeMelissa BrodoNo ratings yet
- If You Find Yourself Becoming Overly AnxiousDocument3 pagesIf You Find Yourself Becoming Overly Anxiousvoyager133100% (1)
- Sexual and Gender Identity DisorderDocument4 pagesSexual and Gender Identity DisordermalindaNo ratings yet
- Schizoaffective DisorderDocument6 pagesSchizoaffective DisorderJenish FitnessCoachNo ratings yet
- Guada A. Dumapit RN, ManDocument18 pagesGuada A. Dumapit RN, ManAnne B. BuenvenidaNo ratings yet
- Patho DSDocument10 pagesPatho DSJesselyn CampitNo ratings yet
- AcetaminophenDocument2 pagesAcetaminophendrugcardref100% (1)
- Acute Respiratory Distress SyndromeDocument2 pagesAcute Respiratory Distress Syndromemanish086No ratings yet
- Patho Unit 5Document37 pagesPatho Unit 5Shafiya ShaikNo ratings yet
- Case Scenario: Pre-Operative: Respiratory Rate Is 22 BPM, Blood Pressure Is 130/90 MMHG and His Temperature Is 37.9Document1 pageCase Scenario: Pre-Operative: Respiratory Rate Is 22 BPM, Blood Pressure Is 130/90 MMHG and His Temperature Is 37.9BiancaGabatinoAbarcaNo ratings yet
- First Line of DrugsDocument5 pagesFirst Line of DrugsBiancaGabatinoAbarcaNo ratings yet
- AsdfDocument2 pagesAsdfBiancaGabatinoAbarcaNo ratings yet
- Defense Mechanism: Abarca Dueñas Palafox VasquezDocument14 pagesDefense Mechanism: Abarca Dueñas Palafox VasquezBiancaGabatinoAbarcaNo ratings yet
- BSN-2A Vasquez, Ma. Ruth Orfiana, Joyce Anne Duque, Erika Roldan, Ryan Pacete, Ashlie AceDocument79 pagesBSN-2A Vasquez, Ma. Ruth Orfiana, Joyce Anne Duque, Erika Roldan, Ryan Pacete, Ashlie AceBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- Deficient NCPDocument2 pagesDeficient NCPBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale Expected OutcomeDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale Expected OutcomeBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- Diseases of The Cervix and The VaginaDocument42 pagesDiseases of The Cervix and The VaginaBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- Nursing Informatics: Health Care Data StandardDocument3 pagesNursing Informatics: Health Care Data StandardBiancaGabatinoAbarcaNo ratings yet
- Health Informatics: (An Illustrative Approach)Document81 pagesHealth Informatics: (An Illustrative Approach)BiancaGabatinoAbarcaNo ratings yet
- Electronic Health Records and Information TechnologyDocument7 pagesElectronic Health Records and Information TechnologyBiancaGabatinoAbarcaNo ratings yet
- 1 Pathophysiology of MeningitisDocument1 page1 Pathophysiology of MeningitisBiancaGabatinoAbarcaNo ratings yet
- Acute Glomerulonephritis PATHODocument2 pagesAcute Glomerulonephritis PATHOBiancaGabatinoAbarcaNo ratings yet
- Certificate of Registration: Tarlac State UniversityDocument1 pageCertificate of Registration: Tarlac State UniversityBiancaGabatinoAbarcaNo ratings yet
- Febrile Siezure: I. OverviewDocument15 pagesFebrile Siezure: I. OverviewBiancaGabatinoAbarcaNo ratings yet
- STS MidtermDocument41 pagesSTS MidtermBiancaGabatinoAbarcaNo ratings yet
- Pathoreal 1Document1 pagePathoreal 1BiancaGabatinoAbarcaNo ratings yet
- Ceftriaxone Sodium: Generic/Brand Name Classification Dosage / Stock Dose Action IndicationDocument11 pagesCeftriaxone Sodium: Generic/Brand Name Classification Dosage / Stock Dose Action IndicationBiancaGabatinoAbarcaNo ratings yet
- Pathoreal 1Document1 pagePathoreal 1BiancaGabatinoAbarcaNo ratings yet
- Reyes, Christine Mae BSN 2-B Rheumatic Fever IDocument23 pagesReyes, Christine Mae BSN 2-B Rheumatic Fever IBiancaGabatinoAbarcaNo ratings yet
- V-Belt DriveDocument9 pagesV-Belt DriveCHANDRASEKARANNo ratings yet
- Fenomenele Postvulcanice Utóvulkáni Mûködések Post Volcanic PhenomenaDocument1 pageFenomenele Postvulcanice Utóvulkáni Mûködések Post Volcanic PhenomenaCosmin FlorinNo ratings yet
- Biops JuliDocument13 pagesBiops Juliklinikutama KayoonNo ratings yet
- A Summary of Role and Reference GrammarDocument30 pagesA Summary of Role and Reference GrammarabarchanNo ratings yet
- Gagne VS BrunerDocument5 pagesGagne VS Bruner86mmc100% (1)
- English 4 Q1 WK1Document3 pagesEnglish 4 Q1 WK1Ace B. SilvestreNo ratings yet
- Abhishek Shukla Project Reporton (Power Purchase)Document57 pagesAbhishek Shukla Project Reporton (Power Purchase)beast singhNo ratings yet
- DC20D MKII Genset Controller Upgrade Version For Diesel - Gasoline Engine - EbayDocument2 pagesDC20D MKII Genset Controller Upgrade Version For Diesel - Gasoline Engine - EbayAliNo ratings yet
- Battered Pile Load CalculationDocument5 pagesBattered Pile Load Calculationovikbasu100% (1)
- NY CREATES IBM Board PacketDocument2 pagesNY CREATES IBM Board PacketSean MickeyNo ratings yet
- Comparative Study Between Public and Private InsuranceDocument21 pagesComparative Study Between Public and Private InsuranceNadeemNo ratings yet
- Danish Progressive RockDocument26 pagesDanish Progressive RockrpilNo ratings yet
- ComboFix Quarantined FilesDocument1 pageComboFix Quarantined FilesJoseph FoxNo ratings yet
- Gear Windage: A Review: Carol N. EastwickDocument6 pagesGear Windage: A Review: Carol N. EastwickR Prabhu SekarNo ratings yet
- English Holiday HomeworkDocument18 pagesEnglish Holiday Homeworkzainab.syed017No ratings yet
- Geometric Design Part I: Road Alignment - Principles & Factors Controlling Road AlignmentDocument10 pagesGeometric Design Part I: Road Alignment - Principles & Factors Controlling Road Alignmentsydney augustNo ratings yet
- AfunimawobeDocument14 pagesAfunimawobeAbdulsala100% (3)
- DM Unit-IvDocument134 pagesDM Unit-IvDwaarakesh RameshNo ratings yet
- EX - EX25 - Survey Items With Benchmark CoverageDocument17 pagesEX - EX25 - Survey Items With Benchmark CoveragePriscilla KosasihNo ratings yet
- A Circle of DistortionDocument20 pagesA Circle of DistortionfinityNo ratings yet
- Fifty Selected Piano-Studies v1 1000050100Document48 pagesFifty Selected Piano-Studies v1 1000050100Lizzie Allan60% (5)
- OP AMPS HughesDocument8 pagesOP AMPS Hughesmarkos_mylonas4152No ratings yet
- IB Annual Financial InformationDocument458 pagesIB Annual Financial InformationazaiahNo ratings yet
- AOF - Orcs v2.50Document2 pagesAOF - Orcs v2.50Emilio Domingo RodrigoNo ratings yet
- Celebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)Document8 pagesCelebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)RIZKINo ratings yet
- UT4000A Patient MonitorDocument5 pagesUT4000A Patient MonitorJuan Pablo MatadamazNo ratings yet
- Hf7/Hf9 Front Axle Spare Parts Catalog: SinotrukDocument9 pagesHf7/Hf9 Front Axle Spare Parts Catalog: SinotrukSamuel WilliamsNo ratings yet














































































































Download as docx, pdf, or txt
You might also like
- 2nd Term Biology Note For Ss2Document33 pages2nd Term Biology Note For Ss2Ukwuma Michael Chijioke100% (21)
- BEL Probationary Engineer Previous Papers & BEL PE Model PapersDocument6 pagesBEL Probationary Engineer Previous Papers & BEL PE Model Papersrakesh_200003No ratings yet
- I. Consciousness: State of AwarenessDocument3 pagesI. Consciousness: State of AwarenessAngeli Kristiana AlejandrinoNo ratings yet
- Case Study, Chapter 51, Assessment and Management of Patients With DiabetesDocument14 pagesCase Study, Chapter 51, Assessment and Management of Patients With DiabetesJake Yvan DizonNo ratings yet
- Chapter 5-6 Theories of AgingDocument54 pagesChapter 5-6 Theories of AgingGladz C CadaguitNo ratings yet
- Cicind Part 2Document23 pagesCicind Part 2tommaso100% (2)
- Acute Heart FailureDocument11 pagesAcute Heart FailureKhaireza KhairuddinNo ratings yet
- Acute GlomerulonephritisDocument14 pagesAcute GlomerulonephritisAnonymous D976HVjqcgNo ratings yet
- Cleviprex® (Clevidipine) Injectable Emulsion (eMC)Document7 pagesCleviprex® (Clevidipine) Injectable Emulsion (eMC)raju1559405No ratings yet
- Amniotic Fluid EmbolismDocument5 pagesAmniotic Fluid EmbolismDenim Embalzado MaghanoyNo ratings yet
- Acute Rheumatic FeverDocument9 pagesAcute Rheumatic FeverHarish Kumar KumawatNo ratings yet
- Drug Study KidneyDocument9 pagesDrug Study Kidneymcnover22No ratings yet
- Additives and Adjuvants in Animal Vaccines - Animal Wellness MagazineDocument9 pagesAdditives and Adjuvants in Animal Vaccines - Animal Wellness MagazineHansley Templeton CookNo ratings yet
- Drug Study 4C Case 2 Final PDFDocument18 pagesDrug Study 4C Case 2 Final PDFRegine Kate JuntoNo ratings yet
- Adrenal PathophysiologyDocument5 pagesAdrenal PathophysiologyditabokNo ratings yet
- Nclex Review Pneumonia COPD AsDocument11 pagesNclex Review Pneumonia COPD Asmj078No ratings yet
- Hallucinations and Hearing VoicesDocument5 pagesHallucinations and Hearing VoicesdevNo ratings yet
- Answer All The Following Short Essay Questions: (3 Questions)Document4 pagesAnswer All The Following Short Essay Questions: (3 Questions)Soad ShedeedNo ratings yet
- Complete Senses Induced Lucid Dreaming (SSILD) Guide - LDDocument10 pagesComplete Senses Induced Lucid Dreaming (SSILD) Guide - LDMarc MarcoNo ratings yet
- Type 1 Diabetes OutlineDocument2 pagesType 1 Diabetes OutlineDominique PorterNo ratings yet
- Atropine: Drug Study: NCM 106 PharmacologyDocument6 pagesAtropine: Drug Study: NCM 106 PharmacologyKevin RosalesNo ratings yet
- Drug Study TramadolDocument1 pageDrug Study Tramadolpius troy macapazNo ratings yet
- What Is AnxietyDocument13 pagesWhat Is AnxietyelaineNo ratings yet
- Burgers DiseaseDocument21 pagesBurgers DiseaseshaitabliganNo ratings yet
- Scleroza MultiplaDocument10 pagesScleroza MultiplaTudor VoinaNo ratings yet
- OBJECTIVES and PATHOPHYSIOLOGY of PHIMOSISDocument5 pagesOBJECTIVES and PATHOPHYSIOLOGY of PHIMOSISShane DamianNo ratings yet
- ArcoxiaDocument27 pagesArcoxiaClarissa Mundo OlmilloNo ratings yet
- Print Article - Glucose Tests - Glucose Test - Blood Sugar - Blood Glucose - Fasting Blood Glucose - Oral Glucose Tolerance Test - OGTT - GTT - Urine Glucose - Lab Tests OnlineDocument9 pagesPrint Article - Glucose Tests - Glucose Test - Blood Sugar - Blood Glucose - Fasting Blood Glucose - Oral Glucose Tolerance Test - OGTT - GTT - Urine Glucose - Lab Tests OnlineHinaRaviNo ratings yet
- Red EyeDocument6 pagesRed EyeafatNo ratings yet
- Thyroid StormDocument6 pagesThyroid StormCristina CenturionNo ratings yet
- Short Term Goal: After 1 Hour of Short Term Goal: After 1Document2 pagesShort Term Goal: After 1 Hour of Short Term Goal: After 1Jordz PlaciNo ratings yet
- Trans Urethral Resection of The ProstateDocument8 pagesTrans Urethral Resection of The ProstateKath RecNo ratings yet
- 1MENIEREDocument6 pages1MENIEREsunny_jr_No ratings yet
- Ms. Cynthia Bea: ProfessorDocument22 pagesMs. Cynthia Bea: ProfessorJohn Cedric Vale CruzNo ratings yet
- Basic Concept of OxygenationDocument50 pagesBasic Concept of OxygenationWiradianto PutroNo ratings yet
- Pathophysiology of ObesityDocument1 pagePathophysiology of ObesityPoldo Josef AngeloNo ratings yet
- Current Treatment of Schizoaffective Disorder According To A Neuralnetwork 2157 7099 1000441Document5 pagesCurrent Treatment of Schizoaffective Disorder According To A Neuralnetwork 2157 7099 1000441Akhsay ChandraNo ratings yet
- SchizopherniaDocument11 pagesSchizopherniaSa Ra Doh0% (1)
- The Effectiveness of Slow Deep Breathing To Decrease Blood Pressure in Hypertension - A Systematic ReviewDocument4 pagesThe Effectiveness of Slow Deep Breathing To Decrease Blood Pressure in Hypertension - A Systematic ReviewThalia NadiraNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
- PSYCHOLOGICAL ASSESSMENT REPORT (Confidential Material) : September 2018Document12 pagesPSYCHOLOGICAL ASSESSMENT REPORT (Confidential Material) : September 2018manar 9939No ratings yet
- NSG Man BulimiaDocument21 pagesNSG Man BulimiaMelodia Turqueza GandezaNo ratings yet
- Psychosis DraftDocument9 pagesPsychosis DraftCHRISTINE JOY. MOLINANo ratings yet
- CHICKEN POX Genesis CarandangDocument10 pagesCHICKEN POX Genesis CarandangGenEsis CarandangNo ratings yet
- Dissociative Identity Disorder Case Study W Mil W JeongDocument15 pagesDissociative Identity Disorder Case Study W Mil W JeongHomework PingNo ratings yet
- TBL2 - GangreneDocument53 pagesTBL2 - Gangreneyouservezeropurpose113No ratings yet
- A Meningioma Is ADocument20 pagesA Meningioma Is ASherry KingNo ratings yet
- Cerebrovascular Disease BleedDocument2 pagesCerebrovascular Disease BleedJogyBoyLunaNo ratings yet
- Nursing DiagnosisDocument16 pagesNursing DiagnosisShemie TutorNo ratings yet
- Pain in Older PatientsDocument66 pagesPain in Older PatientsmehranerezvaniNo ratings yet
- Icd 10 Kardiologi PDFDocument8 pagesIcd 10 Kardiologi PDFRestiKomalaNo ratings yet
- Nursing-Interventions MCN For Infertility MenDocument2 pagesNursing-Interventions MCN For Infertility MenRio DanteNo ratings yet
- NCM 112: Nursing Care of Sexually-Transmitted Infections, Hiv Infections & AidsDocument20 pagesNCM 112: Nursing Care of Sexually-Transmitted Infections, Hiv Infections & Aidsfebie pachecoNo ratings yet
- Polcystic Ovarian SyndromeDocument9 pagesPolcystic Ovarian SyndromeMelissa BrodoNo ratings yet
- If You Find Yourself Becoming Overly AnxiousDocument3 pagesIf You Find Yourself Becoming Overly Anxiousvoyager133100% (1)
- Sexual and Gender Identity DisorderDocument4 pagesSexual and Gender Identity DisordermalindaNo ratings yet
- Schizoaffective DisorderDocument6 pagesSchizoaffective DisorderJenish FitnessCoachNo ratings yet
- Guada A. Dumapit RN, ManDocument18 pagesGuada A. Dumapit RN, ManAnne B. BuenvenidaNo ratings yet
- Patho DSDocument10 pagesPatho DSJesselyn CampitNo ratings yet
- AcetaminophenDocument2 pagesAcetaminophendrugcardref100% (1)
- Acute Respiratory Distress SyndromeDocument2 pagesAcute Respiratory Distress Syndromemanish086No ratings yet
- Patho Unit 5Document37 pagesPatho Unit 5Shafiya ShaikNo ratings yet
- Case Scenario: Pre-Operative: Respiratory Rate Is 22 BPM, Blood Pressure Is 130/90 MMHG and His Temperature Is 37.9Document1 pageCase Scenario: Pre-Operative: Respiratory Rate Is 22 BPM, Blood Pressure Is 130/90 MMHG and His Temperature Is 37.9BiancaGabatinoAbarcaNo ratings yet
- First Line of DrugsDocument5 pagesFirst Line of DrugsBiancaGabatinoAbarcaNo ratings yet
- AsdfDocument2 pagesAsdfBiancaGabatinoAbarcaNo ratings yet
- Defense Mechanism: Abarca Dueñas Palafox VasquezDocument14 pagesDefense Mechanism: Abarca Dueñas Palafox VasquezBiancaGabatinoAbarcaNo ratings yet
- BSN-2A Vasquez, Ma. Ruth Orfiana, Joyce Anne Duque, Erika Roldan, Ryan Pacete, Ashlie AceDocument79 pagesBSN-2A Vasquez, Ma. Ruth Orfiana, Joyce Anne Duque, Erika Roldan, Ryan Pacete, Ashlie AceBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- Deficient NCPDocument2 pagesDeficient NCPBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale Expected OutcomeDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale Expected OutcomeBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- Diseases of The Cervix and The VaginaDocument42 pagesDiseases of The Cervix and The VaginaBiancaGabatinoAbarcaNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- Nursing Informatics: Health Care Data StandardDocument3 pagesNursing Informatics: Health Care Data StandardBiancaGabatinoAbarcaNo ratings yet
- Health Informatics: (An Illustrative Approach)Document81 pagesHealth Informatics: (An Illustrative Approach)BiancaGabatinoAbarcaNo ratings yet
- Electronic Health Records and Information TechnologyDocument7 pagesElectronic Health Records and Information TechnologyBiancaGabatinoAbarcaNo ratings yet
- 1 Pathophysiology of MeningitisDocument1 page1 Pathophysiology of MeningitisBiancaGabatinoAbarcaNo ratings yet
- Acute Glomerulonephritis PATHODocument2 pagesAcute Glomerulonephritis PATHOBiancaGabatinoAbarcaNo ratings yet
- Certificate of Registration: Tarlac State UniversityDocument1 pageCertificate of Registration: Tarlac State UniversityBiancaGabatinoAbarcaNo ratings yet
- Febrile Siezure: I. OverviewDocument15 pagesFebrile Siezure: I. OverviewBiancaGabatinoAbarcaNo ratings yet
- STS MidtermDocument41 pagesSTS MidtermBiancaGabatinoAbarcaNo ratings yet
- Pathoreal 1Document1 pagePathoreal 1BiancaGabatinoAbarcaNo ratings yet
- Ceftriaxone Sodium: Generic/Brand Name Classification Dosage / Stock Dose Action IndicationDocument11 pagesCeftriaxone Sodium: Generic/Brand Name Classification Dosage / Stock Dose Action IndicationBiancaGabatinoAbarcaNo ratings yet
- Pathoreal 1Document1 pagePathoreal 1BiancaGabatinoAbarcaNo ratings yet
- Reyes, Christine Mae BSN 2-B Rheumatic Fever IDocument23 pagesReyes, Christine Mae BSN 2-B Rheumatic Fever IBiancaGabatinoAbarcaNo ratings yet
- V-Belt DriveDocument9 pagesV-Belt DriveCHANDRASEKARANNo ratings yet
- Fenomenele Postvulcanice Utóvulkáni Mûködések Post Volcanic PhenomenaDocument1 pageFenomenele Postvulcanice Utóvulkáni Mûködések Post Volcanic PhenomenaCosmin FlorinNo ratings yet
- Biops JuliDocument13 pagesBiops Juliklinikutama KayoonNo ratings yet
- A Summary of Role and Reference GrammarDocument30 pagesA Summary of Role and Reference GrammarabarchanNo ratings yet
- Gagne VS BrunerDocument5 pagesGagne VS Bruner86mmc100% (1)
- English 4 Q1 WK1Document3 pagesEnglish 4 Q1 WK1Ace B. SilvestreNo ratings yet
- Abhishek Shukla Project Reporton (Power Purchase)Document57 pagesAbhishek Shukla Project Reporton (Power Purchase)beast singhNo ratings yet
- DC20D MKII Genset Controller Upgrade Version For Diesel - Gasoline Engine - EbayDocument2 pagesDC20D MKII Genset Controller Upgrade Version For Diesel - Gasoline Engine - EbayAliNo ratings yet
- Battered Pile Load CalculationDocument5 pagesBattered Pile Load Calculationovikbasu100% (1)
- NY CREATES IBM Board PacketDocument2 pagesNY CREATES IBM Board PacketSean MickeyNo ratings yet
- Comparative Study Between Public and Private InsuranceDocument21 pagesComparative Study Between Public and Private InsuranceNadeemNo ratings yet
- Danish Progressive RockDocument26 pagesDanish Progressive RockrpilNo ratings yet
- ComboFix Quarantined FilesDocument1 pageComboFix Quarantined FilesJoseph FoxNo ratings yet
- Gear Windage: A Review: Carol N. EastwickDocument6 pagesGear Windage: A Review: Carol N. EastwickR Prabhu SekarNo ratings yet
- English Holiday HomeworkDocument18 pagesEnglish Holiday Homeworkzainab.syed017No ratings yet
- Geometric Design Part I: Road Alignment - Principles & Factors Controlling Road AlignmentDocument10 pagesGeometric Design Part I: Road Alignment - Principles & Factors Controlling Road Alignmentsydney augustNo ratings yet
- AfunimawobeDocument14 pagesAfunimawobeAbdulsala100% (3)
- DM Unit-IvDocument134 pagesDM Unit-IvDwaarakesh RameshNo ratings yet
- EX - EX25 - Survey Items With Benchmark CoverageDocument17 pagesEX - EX25 - Survey Items With Benchmark CoveragePriscilla KosasihNo ratings yet
- A Circle of DistortionDocument20 pagesA Circle of DistortionfinityNo ratings yet
- Fifty Selected Piano-Studies v1 1000050100Document48 pagesFifty Selected Piano-Studies v1 1000050100Lizzie Allan60% (5)
- OP AMPS HughesDocument8 pagesOP AMPS Hughesmarkos_mylonas4152No ratings yet
- IB Annual Financial InformationDocument458 pagesIB Annual Financial InformationazaiahNo ratings yet
- AOF - Orcs v2.50Document2 pagesAOF - Orcs v2.50Emilio Domingo RodrigoNo ratings yet
- Celebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)Document8 pagesCelebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)RIZKINo ratings yet
- UT4000A Patient MonitorDocument5 pagesUT4000A Patient MonitorJuan Pablo MatadamazNo ratings yet
- Hf7/Hf9 Front Axle Spare Parts Catalog: SinotrukDocument9 pagesHf7/Hf9 Front Axle Spare Parts Catalog: SinotrukSamuel WilliamsNo ratings yet