Professional Documents
Culture Documents
Can We Conquer Pain?: Review
Can We Conquer Pain?: Review
Uploaded by
fernandoribeirojr98Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Can We Conquer Pain?: Review
Can We Conquer Pain?: Review
Uploaded by
fernandoribeirojr98Copyright:
Available Formats
review
Can we conquer pain?
Joachim Scholz and Clifford J. Woolf
© 2002 Nature Publishing Group http://www.nature.com/natureneuroscience
Neural Plasticity Research Group, Department of Anesthesia, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts 02129, USA
Correspondence should be addressed to C.J.W. (woolf.clifford@mgh.harvard.edu)
Published online 28 October 2002; doi:10.1038/nn942
Pain can be an adaptive sensation, an early warning to protect the body from tissue injury. By the
introduction of hypersensitivity to normally innocuous stimuli, pain may also aid in repair after tissue
damage. Pain can also be maladaptive, reflecting pathological function of the nervous system.
Multiple molecular and cellular mechanisms operate alone and in combination within the peripheral
and central nervous systems to produce the different forms of pain. Elucidation of these mechanisms
is key to the development of treatments that specifically target underlying causes rather than just
symptoms. This new approach promises to revolutionize pain diagnosis and management.
There is an extraordinary dichotomy in the pain field. Exciting The threshold for eliciting pain has to be high enough that it
progress is being made in dissecting out the molecular and cel- does not interfere with normal activities but low enough that it
lular mechanisms that operate in sensory pathways to generate can be evoked before frank tissue damage occurs. This threshold
those neural signals that we ultimately interpret as pain1,2. How- is not fixed and can be shifted either up or down, which may be
ever, for many patients, pain continues to produce severe dis- either adaptive or maladaptive. Shifts in pain threshold and
tress, dominating and disrupting the quality of their lives. Much responsiveness are an expression of neural plasticity, the neuro-
of currently available clinical treatment is only partially effective biological means by which changes in the nervous system can
and may be accompanied by distressing side effects or have abuse modulate the response to any stimulus. Such plasticity or modi-
potential3. Increasing numbers of elderly people in the popula- fiability of the sensory system essentially characterizes clinical
tion means a rising prevalence of age-related painful conditions pain syndromes2,6.
like osteoarthritis that require successful pain treatment 4 . Once tissue has been damaged mechanically or by infection,
Improvements in the management of cancer increase life ischemia, tumor growth or an autoimmune process, multiple
expectancy, but are accompanied by a rise in the cumulative inci- chemical mediators are released from damaged and inflamma-
dence of tumor-related pain syndromes as well as of pain asso- tory cells. The resulting ‘inflammatory soup’ is rich in cytokines,
ciated with therapy, such as chemotherapy-induced painful growth factors, kinins, purines, amines, prostanoids and ions,
polyneuropathy. The unmet clinical need, the personal suffer- including protons7,8. Some inflammatory mediators directly
ing and societal economic costs of pain are substantial. To bridge activate nociceptors, evoking pain. Others act together to pro-
the gap between the ever-advancing understanding of the neu- duce a sensitization of the somatosensory nervous system, which
robiology of pain and the lack of success in clinical pain thera- is characteristic for inflammatory pain, enabling easier activa-
py, a greater and more sophisticated effort needs to be directed to tion of the pain pathway until the tissue heals (Fig. 1b). Mal-
the discovery of targets for new analgesics. In addition, the clin- adaptive plasticity represents those changes that generate
ical approach to pain needs to be reevaluated: a change is spontaneous and exaggerated pain with no discernable protec-
required from an empirical management strategy to one where tive or reparative role. The pain becomes the pathology, typi-
the mechanisms responsible for pain in an individual patient are cally via damage to or dysfunction of the peripheral or central
identified and tackled with specific treatments5. nervous system, termed ‘neuropathic pain’ (Fig. 1c). A reduc-
tion in pain sensitivity by recruiting intrinsic inhibitory mech-
Why pain? anisms can also occur, particularly in those conditions where
Although we use a single word to describe any feeling that is an emergency reaction is a greater imperative than preventing
unpleasant and hurts, this does not mean that pain is a mono- tissue damage9.
lithic entity. There is pain as a sensory experience and pain as
perceptual metaphor of suffering or grief. We deal here only Pain mechanisms
with the former. Pain the sensation can be further split into dis- Nociceptive, inflammatory and neuropathic pain result from
tinct categories. Pain normally serves as a warning device, an diverse mechanisms. Some of these mechanisms are unique to
alarm system activated in response to impending damage to the one painful condition; others are present in multiple clinical syn-
organism. This nociceptive pain is activated only by noxious dromes, or may be expressed at different times during the nat-
stimuli acting on a specialized high-threshold sensory apparatus ural history of a syndrome. In some patients, a single mechanism
(Fig. 1a). Nociception is essential for the survival of organisms may produce their pain; in others, multiple mechanisms may
in a potentially hostile environment. Nociceptive pain, once it contribute. The same symptom (for example, pain in response
is present, once the alarm has gone off, so dominates attention to light touch of the skin) may be generated by a number of
that it is more like a motivational drive than a sensation, resem- mechanisms. Moreover, a single mechanism (for example, upreg-
bling hunger, thirst or sexual desire. ulation of a voltage-gated sodium channel) may potentially pro-
1062 nature neuroscience supplement • volume 5 • november 2002
review
a Nociceptive pain Pain
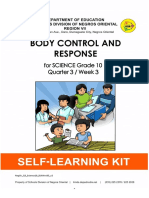
Fig. 1. Nociceptive, inflammatory and neuro-
pathic pain. (a) Noxious stimuli are transduced
Avoidance
into electrical activity at the peripheral termi-
Emotional
TRPV1 reaction nals of unmyelinated C-fiber and thinly myeli-
TRPV2 nated Aδ-fiber nociceptors by specific
TRPV3 DRG receptors or ion channels sensitive to heat,
TREK-1 (cell body) mechanical stimuli, protons and cold. This
activity is conducted to the spinal cord and,
© 2002 Nature Publishing Group http://www.nature.com/natureneuroscience
TRPV1 after transmission in central pathways, to the
ASIC cortex, where the sensation of pain is experi-
Acid DRASIC enced. (b) Damaged tissue, inflammatory and
tumor cells release chemical mediators creat-
Withdrawal
ing an ‘inflammatory soup’ that activates or
MDEG
modifies the stimulus response properties of
DRASIC nociceptor afferents. This, in turn, sets up
TREK-1 Spinal cord changes in the responsiveness of neurons in
the CNS (Fig. 2). (c) Neuropathic pain arises
from lesions to or dysfunction of the nervous
system. Conditions affecting the peripheral
TRPM8
nervous system, as in carpal tunnel syndrome,
the spinal cord after traumatic injuries or the
brain after stroke, can all cause neuropathic
pain, which is characterized by a combination
of neurological deficits and pain.
b Inflammatory pain Mast cell
to higher centers 11 . Activity in the
Neutrophil spinothalamic tract relays through the
Macrophage granulocyte thalamus to the somatosensory cortex
and associated areas. The parabrachial
nucleus of the brainstem has connec-
tions to the ventral medial nucleus of the
hippocampus and the central nucleus of
the amygdala, brain regions involved in
the affective response to pain. Impulses
Histamine H+ from supraspinal centers are integrated
Serotonin Nerve growth factor in the midbrain periaqueductal gray,
Bradykinin TNFα
Prostaglandins Endothelins Pain treatment options: which is pivotal in modulating descend-
ATP Interleukins Cox2 inhibitors ing facilitation and inhibition of noci-
Opioids ceptive input mainly via the nucleus
raphe magnus11.
Nociceptor function is substantially
c Neuropathic pain modified in response to tissue damage,
Spinal cord inflammation or injury of the nervous
injury system. Post-translational and tran-
scriptional changes can profoundly alter
the threshold, excitability and transmis-
sion properties of nociceptors, con-
Thalamic stroke tributing to pain hypersensitivity and
Carpal tunnel spontaneous pain (Fig. 2). Changes can
syndrome
be localized to the peripheral terminal
Pain treatment options: (peripheral sensitization), the site of
Tricyclic antidepressants axonal injury or the central synapse, or
Anticonvulsants
produce general alterations in mem-
Na+ channel blockers
NMDA receptor antagonists brane properties. Some of the changes
Opioids are rapid, as with a reduction in heat
pain threshold following phosphoryla-
Debbie Maizels
tion of the heat transducer receptors
duce different symptoms like spontaneous burning pain, shock- TRPV1 (VR1) and TRPV2 (VRL-1). Others require retrograde
like pain or paresthesias (pins and needles)10. transport of signals to the cell body, activation of signal trans-
Nociceptor Aδ and C somatosensory afferent terminals duction cascades, changes in transcription and then orthograde
transduce external noxious stimuli into electrical activity. The transport of proteins to the peripheral or central terminals12.
resultant action potentials are conducted to the dorsal horn of Activation of nociceptors is not, however, the only way to
the spinal cord, and the input is conveyed, after synaptic pro- trigger pain. After peripheral tissue injury or damage to the
cessing, via the spinothalamic and spinoparabrachial pathways nervous system, low-threshold sensory fibers, which normally
nature neuroscience supplement • volume 5 • november 2002 1063
review
a Nociceptive pain b Peripheral sensitization Fig. 2. Nociceptor-mediated pain repre-
TRPV1
sents those pain conditions driven by activa-
tion of peripheral nociceptor sensory fibers.
(a) Nociceptive pain is produced under physio-
Nav1.8/1.9 logical conditions only by noxious stimuli acting
Na+
Na+ Na+
Nav1.8/1.9 Ca2+ Kv Nav1.8/1.9 on high-threshold nociceptors. (b) With inflam-
Na+ PKA mation, components of the ‘inflammatory soup’,
Ca2+ Ca2+ 2+
PKC Ca such as bradykinin or prostaglandins, bind to
© 2002 Nature Publishing Group http://www.nature.com/natureneuroscience
Ca2+
TRPV3 TRPV1
B1/2
G-protein-coupled receptors and induce activa-
TRPV2 TRPM8 TRPV1 EP
ASIC P2X3 ASIC P2X3 tion of protein kinases A and C in nociceptor
peripheral terminals, which then phosphorylate
MDEG
Pg ion channels and receptors. As a result, the
BK
threshold of activation of transducer receptors
H+ ATP such as TRPV1 is reduced, and the excitability of
the peripheral terminal membrane increases,
c Ectopic activity d Transcriptional changes in the DRG producing a state of heightened sensitivity,
Nociceptor Voltage-gated NGF Inflammatory termed ‘peripheral sensitization’. (c) After injury
activity Ca2+ channels mediators to nociceptor neurons, increases in transcription
Nav
or altered trafficking of sodium channels as well
Trk A as a reduction in potassium channels increases
Kv membrane excitability sufficiently so that action
Nav Na+ Ca2+
Ca2+ potentials are generated spontaneously (ectopic
Ca2+ activity). (d) Activity-dependent signal transduc-
Nucleus
PKA Transcription factor tion cascades and signaling pathways down-
Nav CaMK IV P P stream to receptors bound by cytokines and
Kv RNA growth factors act to modify transcription in
Erk1/2
p38 nociceptor neurons. Altered production of
JNK numerous proteins modifies the phenotype of
the neurons, changing their transduction, con-
RNA polymerase II
Neuroma site duction and transmission properties.
Debbie Maizels
only produce innocuous sensations like light touch, can begin millennia—and non-steroidal anti-inflammatory drugs
to produce pain, a very substantial change in the normal func- (NSAIDs), a prototypic member of which is salicylic acid, the
tional specificity of the sensory system (Fig. 3). Although this active ingredient in willow bark, a folk remedy for inflamma-
pain obviously no longer represents the presence of a damaging tion and pain. The local anesthetic activity of cocaine was
external stimulus, to the individual it feels that the pain aris- reported one hundred years ago without any knowledge of sodi-
es in the periphery from a noxious stimulus. Such a shift in um channels. More recently, tricyclic antidepressants and anti-
the excitability of the CNS contributes to the hypersensi- convulsants, including carbamezepine and gabapentin, were
tivity to non-painful stimuli after surgery or during migraine found to produce analgesia empirically, not through any knowl-
attacks, as well as the diffuse muscle tenderness of myofas- edge of their molecular targets17. Triptans have substantially
cial syndromes, and sensory abnormalities of the gastro- improved the management of migraine. These 5-HT1B/1D ago-
intestinal tract in non-cardiac chest pain and irritable bowel nists were initially developed to produce cranial vasoconstric-
syndrome13,14. tion, but their inhibitory effects on trigeminal and second-order
Increases in synaptic transmission in the dorsal horn (central neurons may be more important18. One great success in mod-
sensitization) can begin almost immediately as a result of ern pain pharmacology has been the introduction of Cox2-spe-
activity-dependent phosphorylation and trafficking of receptors cific inhibitors, but rather than possessing improved efficacy,
or ion channels. Central sensitization can be sustained for some these drugs produce less gastric and bleeding side effects by not
time by transcriptional changes, including induction of genes inhibiting Cox1 (ref. 19).
such as Cox2 to generate PGE2, which alters the excitability of Genetic background affects nociceptive pain sensitivity in
neurons. Structural alterations in the synaptic contacts of low- animals and may influence susceptibility to the development of
threshold afferents with pain transmission neurons, or a reduc- persistent pain20. A patient’s gender or genes may also interfere
tion of inhibitory mechanisms due to a loss of interneurons, with the response to analgesic drugs. Different expression pat-
represent persistent changes in the CNS that eventually result in terns of opioid receptors may explain why some patients are
a fixed state of sensitization (Fig. 3). insensitive to opioids. The metabolism and biological availabili-
Immune cells may be involved in inflammatory pain, cancer ty of numerous drugs, including tricyclic antidepressants,
pain and pain after nerve injury. They are activated both in the codeine, tramadol and the NMDA antagonist dextromethor-
periphery and within the central nervous system in response to phan 21, depend on the allelic polymorphism of the hepatic
tissue damage, inflammation or mechanical nerve lesions15. The cytochrome P450 monooxygenase system.
immune reaction may increase nociception through the release of The mechanisms that individually or collectively produce pain
cytokines, but granulocytes and monocytes can also promote now need to be seen as representing the targets for the rational
analgesia by secreting β-endorphin and enkephalin16. development of novel analgesics. Two general approaches for the
discovery of novel pain targets have evolved: either evaluation in
A need for smarter drugs depth after a focused search of the particular role of an individ-
Current analgesics have been discovered by empirical observa- ual protein in producing pain1,2,11, or mass screening using high-
tion or serendipity. These include opiates—the analgesic activ- throughput mRNA or proteomic screens22. The former has been
ity of opium poppy extracts that have been recognized for used with great effectiveness to unravel many of those receptors
1064 nature neuroscience supplement • volume 5 • november 2002
review
a Immediate central sensitization b Delayed central sensitization
Nociceptive TrkB Dorsal horn EP/IP
afferent, neuron Inhibitory
central interneuron +
BDNF
terminal src Nociceptive
afferent IL-1
NMDA-R EP
PKC
© 2002 Nature Publishing Group http://www.nature.com/natureneuroscience
Glutamate
Cox2 PKA
+ Erk1/2
AMPA-R Ca2+ EP
ERK
+ PGE2
p38
JNK
SP mGlu-R
PKA Transcription
P P RNA
p38 – factor
Glycine
IP3 receptor
NK1 RNA polymerase II
Dorsal DREAM
RNA
horn
neuron Nucleus
c Changes in synaptic connectivity d Loss of inhibition
Nociceptive afferent
Pain
transmission
neuron
Non-nociceptive afferent
(Aβ-fiber)
Excitatory
interneuron
Sprouting after
nerve injury
Debbie Maizels
Fig. 3. Non-nociceptor-mediated pain is generated by sensory inputs that would normally produce an innocuous sensation, and reflects a change in
the functioning of central neurons. (a) Activity-dependent central sensitization. An immediate and relatively short-lasting increase in the excitability
and responsiveness of pain transmission dorsal horn neurons, which is due to phosphorylation of ion channels and receptors and follows nociceptor-
driven transmitter release and activation of intracellular kinases. Eventually, the response to normally subthreshold inputs is increased.
(b) Transcription-dependent central sensitization. Enhanced gene expression due to the activation of transcription factors, as well as the removal of
repressors like DREAM, results in long-lasting changes in the function of dorsal horn neurons. Cox2 induction leads to PGE2 production, which acts
pre- and postsynaptically to facilitate excitatory and reduce inhibitory transmission. (c) After peripheral nerve injury, the central terminals of myeli-
nated non-nociceptive Aβ-afferents sprout in the dorsal horn and form new connections with nociceptive neurons in laminae I and II. This re-wiring
of the circuitry of the spinal cord may contribute to persistent pain hypersensitivity. (d) Disinhibition. Normal sensory inflow is actively controlled by
inhibitory interneurons. Reduced synthesis of the inhibitory neurotransmitters GABA and glycine or loss of these inhibitory interneurons after
excessive release of the excitotoxic amino acid glutamate following peripheral nerve injury increases the excitability of pain transmission neurons
such that they begin to respond to normally innocuous inputs.
and ion channels responsible for transducing noxious stimuli in Targeting pain mechanisms
the periphery and for modulating sensory processing in the dor- The notion that there is a class of drug, a universal analgesic, that
sal horn of the spinal cord (Fig. 4). The latter has only begun to can intrinsically reduce all pain, is obsolete and has to be aban-
be applied, but is revealing that many hundreds of genes change doned. Pain is heterogeneous in terms of etiological factors,
their expression in sensory neurons after damage to a peripher- mechanisms and temporal characteristics. Consequently, treat-
al nerve or exposure to inflamed tissue. These include genes never ment must be targeted not at the general symptom, the pain, or
before described in the nervous system, whose function is its temporal properties, acute or chronic, but rather at the under-
presently unknown. lying neurobiological mechanisms responsible (Fig. 5).
nature neuroscience supplement • volume 5 • november 2002 1065
review
Fig. 4. Key molecular elements The second need is to develop therapeutic tools to specifical-
Transduction
in the transduction, transmis-
TRPV1, TRPV2, TRPV3, TRPM8 ly interrupt the particular pain mechanisms. This will require
ASIC, DRASIC sion and signal processing of
MDEG, TREK-1
nociceptive input in the periph-
identifying the key molecular targets involved in the manifestation
BK1, BK2
P2X3 eral and central nervous sys- of the mechanism and finding specific activators or inhibitors,
tem represent potential targets whatever appropriate, by high-throughput pharmaceutical
Peripheral sensitization for the development of new screens with proof-of-concept trials in patients. One problem is
NGF, TrkA
analgesics. what clinical outcome measures should be applied to evaluate
© 2002 Nature Publishing Group http://www.nature.com/natureneuroscience
TRPV1
Nav1.8 effects on pain mechanisms. Current clinical analgesic trials select
Peripheral
PKA, PKC isoforms, CaMK IV
Erk1/2, p38, JNK patients on the basis of disease and use crude global outcome
IL-1β, cPLA2, COX2, EP1, EP3, EP4
TNFα The first need, clearly, is measures; no effort is made to identify mechanisms. Symptoms,
to identify the major mech- signs and special investigations should be used to define mecha-
Membrane excitability anisms that participate in nisms participating in the generation of a painful condition. The
of primary afferents
Nav1.8, Nav1.9 producing clinical pain syn- number needed to treat (NNT), a measure of how many patients
K+ channel dromes. The validation of have to be treated to see a 50% response, varies from 1.7 to over
animal models, showing 10 for the analgesics currently available for neuropathic pain3.
Synaptic transmission
Presynaptic that they are actually surro- This reflects the lack of efficacy of empirically administered anal-
VGCC
Adenosine-R
gates for mechanisms pre- gesics, some of which are aimed at targets that may not be
(mGlu-R) sent in human patients, is a expressed in a given patient. Cox2 inhibitors will only work, for
Postsynaptic
AMPA/kainate-R, NMDA-R, mGlu-R key issue. Although it is example, if Cox2 has been induced.
NK1
Nav1.3
possible to produce a Although this decade has been dedicated the “Decade of Pain
K+ channels stereotyped pain-like Control and Research” by the US Congress, too little attention
behavior in animals, this continues to be directed at pain research, and success at control-
Central inhibition does not mean that the ling pain remains limited. However, conquering pain, using the
GABA, GABAA-R, GABAB-R
Glycine-R mechanisms involved in understanding of its nature, mechanisms and molecular com-
NE, 5-HT
Central
Opioid receptors these models are identical ponents to drive the pharmaceutical screening and development
CB1 to those found in patients, of new analgesic drugs, is at last a realistic prospect, albeit a
where the complexity, onset daunting challenge.
Signal transduction
PKA, PKC isoforms and persistence of pain tend
ERK, p38, JNK
to be very different. Some RECEIVED 10 JULY; ACCEPTED 3 SEPTEMBER 2002
Debbie Maizels
Gene expression
conventional outcome
c-fos, c-jun, CREB measures in animal nerve
DREAM 1. Julius, D. & Basbaum, A. I. Molecular mechanisms of nociception. Nature
injury models, like heat 413, 203–210 (2001).
pain hypersensitivity, are 2. Woolf, C. J. & Salter, M. W. Neuronal plasticity—increasing the gain in pain.
not features of clinical neuropathic pain. Moreover, sponta- Science 288, 1765–1768 (2000).
3. Sindrup, S. H. & Jensen, T. S. Efficacy of pharmacological treatments of
neous pain, a major clinical problem, cannot be directly mea- neuropathic pain: an update and effect related to mechanism of drug action.
sured in animals23. Although functional imaging reveals the Pain 83, 389–400 (1999).
regions in the human brain activated during pain and may pro- 4. Lynch, D. in Practical Management of Pain 3rd edn. (ed. Raj, P.P.) 270–293
(Mosby, St. Louis, Missouri, 2000).
vide an objective way of assessing pain and its response to treat- 5. Woolf, C. J. & Mannion, R. J. Neuropathic pain: aetiology, symptoms,
ment24, it does not disclose mechanisms. mechanisms, and management. Lancet 353, 1959–1964 (1999).
6. Porreca, F., Ossipov, M. H. & Gebhart, G. F. Chronic pain and medullary
descending facilitation. Trends Neurosci. 25, 319–325 (2002).
7. Boddeke, E. W. Involvement of chemokines in pain. Eur. J. Pharmacol. 429,
Fig. 5. Rational treatment of pain requires identification of pain mecha- 115–119 (2001).
nisms as targets of drug therapy. Conventionally therapeutic interven- 8. Mantyh, P. W., Clohisy, D. R., Koltzenburg, M. & Hunt, S. P. Molecular
tions are aimed at disease mechanisms (disease modifying) or providing mechanisms of cancer pain. Nature Rev.Cancer 2, 201–209 (2002).
symptomatic pain relief, based on empirical knowledge and evidence 9. Fields, H. L. Pain modulation: expectation, opioid analgesia and virtual pain.
from drug trials. However, pain is driven not by disease but by pain Prog. Brain Res. 122, 245–253 (2000).
10. Woolf, C. J. & Max, M. B. Mechanism-based pain diagnosis: issues for
mechanisms. A standardized assessment of pain-related symptoms and analgesic drug development. Anesthesiol. 95, 241–249 (2001).
signs is required to determine the pain mechanisms present in an indi- 11. Hunt, S. P. & Mantyh, P. W. The molecular dynamics of pain control. Nat.
vidual patient, and management of pain needs to be targeted at these Rev. Neurosci. 2, 83–91 (2001).
mechanisms. Outcome measures should reflect changes in pain mecha- 12. Svensson, C. I. & Yaksh, T. L. The spinal phospholipase-cyclooxygenase-
prostanoid cascade in nociceptive processing. Annu. Rev. Pharmacol. Toxicol.
nisms instead of the overall intensity of pain. 42, 553–583 (2002).
13. Burstein, R., Yarnitsky, D., Goor-Aryeh, I., Ransil, B. J. & Bajwa, Z. H. An
association between migraine and cutaneous allodynia. Ann. Neurol. 47,
Etiological factors
614–624 (2000).
14. Sarkar, S., Aziz, Q., Woolf, C. J., Hobson, A. R. & Thompson, D. G.
Contribution of central sensitisation to the development of non-cardiac chest
pain. Lancet 356, 1154–1159 (2000).
Clinical entity 15. Watkins, L. R., Milligan, E. D. & Maier, S. F. Glial activation: a driving force
for pathological pain. Trends Neurosci. 24, 450–455 (2001).
16. Rittner, H. L. et al. Opioid peptide-expressing leukocytes: identification,
recruitment, and simultaneously increasing inhibition of inflammatory pain.
Mechanism-oriented Anesthesiology 95, 500–508 (2001).
Disease mechanisms Pain mechanisms
pain treatment
17. Rose, M. A. & Kam, P. C. Gabapentin: pharmacology and its use in pain
management. Anaesthesia 57, 451–462 (2002).
18. Goadsby, P. J., Lipton, R. B. & Ferrari, M. D. Migraine—current
Pain-related Mechanism-specific understanding and treatment. N. Engl. J. Med. 346, 257–270 (2002).
Symptoms and signs
symptoms and signs outcome measures 19. FitzGerald, G. A. & Patrono, C. The coxibs, selective inhibitors of
cyclooxygenase-2. N. Engl. J. Med. 345, 433–442 (2001).
Debbie Maizels
1066 nature neuroscience supplement • volume 5 • november 2002
review
20. Flores, C. M. & Mogil, J. S. The pharmacogenetics of analgesia: toward a 22. Wood, J. N. II. Genetic approaches to pain therapy. Am. J. Physiol.
genetically-based approach to pain management. Pharmacogenomics 2, Gastrointest. Liver Physiol. 278, G507–G512 (2000).
177–194 (2001). 23. Mogil, J. S. The genetic mediation of individual differences in sensitivity to
21. Desmeules, J. A., Oestreicher, M. K., Piguet, V., Allaz, A. F. & Dayer, P. pain and its inhibition. Proc. Natl. Acad. Sci. USA 96, 7744–7751 (1999).
Contribution of cytochrome P-4502D6 phenotype to the neuromodulatory 24. Becerra, L., Breiter, H. C., Wise, R., Gonzalez, R. G. & Borsook, D. Reward
effects of dextromethorphan. J. Pharmacol. Exp. Ther. 288, 607–612 (1999). circuitry activation by noxious thermal stimuli. Neuron 32, 927–946 (2001).
© 2002 Nature Publishing Group http://www.nature.com/natureneuroscience
nature neuroscience supplement • volume 5 • november 2002 1067
You might also like
- EF English TestDocument11 pagesEF English TestRobert Florez29% (17)
- BIO ELSWB English Language Skills Workbook Answers 5pDocument23 pagesBIO ELSWB English Language Skills Workbook Answers 5pnghaochen329100% (1)
- Running Head: FIELD NOTES 1Document4 pagesRunning Head: FIELD NOTES 1Swapnika Chava50% (2)
- The Senses. Comprehensive Reference (NeuroscienDocument4,112 pagesThe Senses. Comprehensive Reference (NeuroscienIndira EspitiaNo ratings yet
- 3Document5 pages3Jonathan HewittNo ratings yet
- ManualDocument81 pagesManualmumtonagNo ratings yet
- 120 207 1 SMDocument12 pages120 207 1 SMDwilia RismayantiNo ratings yet
- Baumann 2013Document184 pagesBaumann 2013sekar alifaNo ratings yet
- Management of Acute PainDocument7 pagesManagement of Acute PainEstefaniSabrinaSandovalNo ratings yet
- Anesthesiology 250 Learning Modules: Page 1 of 32Document32 pagesAnesthesiology 250 Learning Modules: Page 1 of 32Niña AvilaNo ratings yet
- Mechanisms of Pain MUIRDocument11 pagesMechanisms of Pain MUIRLorena B-iNo ratings yet
- NIH Public Access: Author ManuscriptDocument31 pagesNIH Public Access: Author Manuscriptvicente gaticaNo ratings yet
- Factorii de Risc În Vulnerabilitatea Durerii CroniceDocument9 pagesFactorii de Risc În Vulnerabilitatea Durerii Cronicecj_catalinaNo ratings yet
- Neuropathic Pain A Maladaptive Response of The NerDocument34 pagesNeuropathic Pain A Maladaptive Response of The NerMayNo ratings yet
- Ananad2 PDFDocument8 pagesAnanad2 PDFmustafasacarNo ratings yet
- Biomedicine & Pharmacotherapy: S. Ronchetti, G. Migliorati, D.V. Del FinoDocument8 pagesBiomedicine & Pharmacotherapy: S. Ronchetti, G. Migliorati, D.V. Del FinoPutri Aswariyah RamliNo ratings yet
- Pathological Pain and The Neuroimmune InterfaceDocument36 pagesPathological Pain and The Neuroimmune InterfacecontatofornazaNo ratings yet
- Assessment and Treatment of Pain in Pediatric PatientsDocument10 pagesAssessment and Treatment of Pain in Pediatric PatientsAnonymous zd0Bwj4nNo ratings yet
- Pain Management and Wound Care: Kari Bechert, MPT, Steve E. Abraham, DPMDocument7 pagesPain Management and Wound Care: Kari Bechert, MPT, Steve E. Abraham, DPMmayaNo ratings yet
- Neuropathic Pain: Mechanisms and Their Clinical ImplicationsDocument12 pagesNeuropathic Pain: Mechanisms and Their Clinical Implicationsfahri azwarNo ratings yet
- Pain Management in Patients Receiving Palliative CareDocument9 pagesPain Management in Patients Receiving Palliative CareelbaNo ratings yet
- What Is This Thing Called Pain (2010)Document3 pagesWhat Is This Thing Called Pain (2010)Hugo FalquetoNo ratings yet
- 2014 Chronic Pain. The Role of Learning and Brain PlasticityDocument12 pages2014 Chronic Pain. The Role of Learning and Brain PlasticityCristian OyarzoNo ratings yet
- Dor NeuropaticaDocument4 pagesDor NeuropaticaRoderley ReisNo ratings yet
- Assessment and Treathment of Pain in Pediatric PatientsDocument11 pagesAssessment and Treathment of Pain in Pediatric Patientsfuka priesleyNo ratings yet
- 2015 - Nociception and Role of Immune System in PainDocument8 pages2015 - Nociception and Role of Immune System in PainDumitritaNo ratings yet
- Pain Basic Consideration PDFDocument4 pagesPain Basic Consideration PDFCiprian CorneaNo ratings yet
- AnalgesiaDocument6 pagesAnalgesiajoyceereiisNo ratings yet
- Mechanisms of PainDocument3 pagesMechanisms of PainPembaca sejatiNo ratings yet
- The Management of Chronic Pain in Older PersonsDocument17 pagesThe Management of Chronic Pain in Older PersonsyurikhanNo ratings yet
- ENDOMETRIOSE X FISIOTERAPIA PDFDocument19 pagesENDOMETRIOSE X FISIOTERAPIA PDFLuiza GusmãoNo ratings yet
- Greene, S. A. Chronic Pain Pathophysiology and Treatment Implications. Topics in Companion Animal Medicine, v.25, n.1, p.5-9. 2010 PDFDocument5 pagesGreene, S. A. Chronic Pain Pathophysiology and Treatment Implications. Topics in Companion Animal Medicine, v.25, n.1, p.5-9. 2010 PDFFran WermannNo ratings yet
- For Nasari 2012Document8 pagesFor Nasari 2012basma adianaNo ratings yet
- Nre 208007Document11 pagesNre 208007Soledad CáceresNo ratings yet
- Assessment of Acute and Chronic Pai 2019 Anaesthesia Intensive Care MediciDocument5 pagesAssessment of Acute and Chronic Pai 2019 Anaesthesia Intensive Care MedicipollodearrozNo ratings yet
- Pain 11thDocument79 pagesPain 11thseptiman zebuaNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Pain Key Points Magnitude of Pain ProblemDocument7 pagesLewis: Medical-Surgical Nursing, 10 Edition: Pain Key Points Magnitude of Pain ProblemAmber Nicole HubbardNo ratings yet
- Central Mechanisms of Pathological PainDocument9 pagesCentral Mechanisms of Pathological PainRocio DominguezNo ratings yet
- Woolf1998-Towards A Mechanism-Based Classification of PainDocument3 pagesWoolf1998-Towards A Mechanism-Based Classification of PainLetícia AlmeidaNo ratings yet
- Curcumin and Boswelia For Pain ReliefDocument10 pagesCurcumin and Boswelia For Pain ReliefSusan FNo ratings yet
- PCT 2Document20 pagesPCT 2Wialda Dwi rodyahNo ratings yet
- AliliDocument3 pagesAliliSaf Tanggo DiampuanNo ratings yet
- Manajemen NyeriDocument2 pagesManajemen Nyeriscan resepNo ratings yet
- Pain Classifitation 2 PDFDocument11 pagesPain Classifitation 2 PDFAnnisa BrilianNo ratings yet
- Pain PathwaysDocument45 pagesPain PathwaysKabirNo ratings yet
- Central Sensitization A Generator of Pain HypersensitivityDocument32 pagesCentral Sensitization A Generator of Pain HypersensitivityEvaNo ratings yet
- TL 4Document4 pagesTL 4ĐôngNo ratings yet
- Psychology of PainDocument8 pagesPsychology of PainRana KoshhaNo ratings yet
- Nihms 396443Document12 pagesNihms 396443kickinghorse892No ratings yet
- Pain ProcessingDocument12 pagesPain ProcessingKunal KatyayanNo ratings yet
- Treatment of Chronic Non Cancer Pain Lancet 2011Document10 pagesTreatment of Chronic Non Cancer Pain Lancet 2011jhonjrodriNo ratings yet
- What Is This Thing Called Pain?: Review Series IntroductionDocument3 pagesWhat Is This Thing Called Pain?: Review Series Introductionluis bulnesNo ratings yet
- Topicalmedicationsastreatment Ofneuropathicorofacialpain: Cibele Nasri-Heir,, Junad Khan,, Gary M. HeirDocument13 pagesTopicalmedicationsastreatment Ofneuropathicorofacialpain: Cibele Nasri-Heir,, Junad Khan,, Gary M. HeirMarco Antonio Morales OsorioNo ratings yet
- Sensibiliza o Central Nas Dores CR Nicas REVIEW LANCET 2021 - Open AccessDocument10 pagesSensibiliza o Central Nas Dores CR Nicas REVIEW LANCET 2021 - Open AccessRichard Mezadri ViebrantzNo ratings yet
- Physiotherapy Management of Fibromyalgia 2000Document8 pagesPhysiotherapy Management of Fibromyalgia 2000PranjalNo ratings yet
- 1.the Biology of Pain Through The Rheumatology LensDocument11 pages1.the Biology of Pain Through The Rheumatology Lensmorena19932308No ratings yet
- Palmitoylethanolamide in The Treatment of Chronic Pain Caused by Different EtiopathogenesisDocument10 pagesPalmitoylethanolamide in The Treatment of Chronic Pain Caused by Different EtiopathogenesisSpore FluxNo ratings yet
- Nijs Et Al 2021 LANCET RheumatologyDocument10 pagesNijs Et Al 2021 LANCET RheumatologyVicaroNo ratings yet
- NRN 2533Document14 pagesNRN 2533黃聖涵No ratings yet
- Pain Management in Palliative Care - Art or ScienceDocument6 pagesPain Management in Palliative Care - Art or ScienceArmando José MaldonadoNo ratings yet
- AAHAAAFP Pain Management GuidelinesDocument15 pagesAAHAAAFP Pain Management GuidelinesMr. questionNo ratings yet
- FSP DolorDocument15 pagesFSP DoloranyNo ratings yet
- Physrev 00045 2019Document44 pagesPhysrev 00045 2019gck85fj8pnNo ratings yet
- نسخة Lecture - PAIN Assessment & ManagementDocument52 pagesنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)
- An Overview of The Physiology of Pain For The VeterinarianDocument5 pagesAn Overview of The Physiology of Pain For The VeterinarianMr. questionNo ratings yet
- PhysioEx 2 Skeletal Muscle Physiology Worksheet Act 1 To 7Document8 pagesPhysioEx 2 Skeletal Muscle Physiology Worksheet Act 1 To 7ZHAREIGHNEILE C. MAMOLONo ratings yet
- The Role of Locus Coeruleus in The Regulation of Cognitive Performance Marius Usher, Et Al. Science 283, 549 (1999)Document7 pagesThe Role of Locus Coeruleus in The Regulation of Cognitive Performance Marius Usher, Et Al. Science 283, 549 (1999)Ed Landau Add SolNo ratings yet
- Gilles Deleuze Gilles Deleuze From AzDocument92 pagesGilles Deleuze Gilles Deleuze From AzConrad MerkelNo ratings yet
- 1bsn2 - Module 6Document16 pages1bsn2 - Module 6Kiana Ramosa100% (1)
- Atar Notes Endorcine SystemDocument12 pagesAtar Notes Endorcine Systembella.wenman6No ratings yet
- AQA Homeostasis and Response Knowledge OrganiserDocument6 pagesAQA Homeostasis and Response Knowledge OrganiserDan LiNo ratings yet
- Stretch ReflexDocument31 pagesStretch ReflexTots Enriquez Navarro100% (1)
- Gibson 1962 Observations On Active TouchDocument15 pagesGibson 1962 Observations On Active TouchNatalia MoraNo ratings yet
- Seminar ON Sensory Deprevation: Prepared By: P.Manojkumar. MSC (N) 1St Yr, VmconDocument29 pagesSeminar ON Sensory Deprevation: Prepared By: P.Manojkumar. MSC (N) 1St Yr, VmconManoj Bala0% (1)
- Coordination & Response 3 QP - Marking SchemeDocument10 pagesCoordination & Response 3 QP - Marking SchemeSiti FairuzNo ratings yet
- Worksheet For Nervous Systems-KeyDocument5 pagesWorksheet For Nervous Systems-KeyNazarine Torres100% (2)
- Altered Cognitive-Perceptual Patterns: Clients With Neuroligic DisordersDocument96 pagesAltered Cognitive-Perceptual Patterns: Clients With Neuroligic DisordersJobelle AcenaNo ratings yet
- Vergara Et Al., 2003Document14 pagesVergara Et Al., 2003SONo ratings yet
- Gabriela Goldschmidt Anat Litan Sever - Inspiring Design Ideas With TextsDocument17 pagesGabriela Goldschmidt Anat Litan Sever - Inspiring Design Ideas With TextsOmega ZeroNo ratings yet
- OT Practice FrameworkDocument12 pagesOT Practice Frameworkenrico_aguila100% (2)
- 1 - Action & Graded Potentials LecDocument21 pages1 - Action & Graded Potentials LecMohamedHossamNo ratings yet
- Wa0003.Document23 pagesWa0003.maykoljacksonpNo ratings yet
- Genesis of Resting Membrane PotentialDocument9 pagesGenesis of Resting Membrane PotentialSyauqat AthirNo ratings yet
- 2J Coordination: Time: 1 Hour 5 Minutes Total Marks Available: 65 Total Marks AchievedDocument26 pages2J Coordination: Time: 1 Hour 5 Minutes Total Marks Available: 65 Total Marks AchievedRabia RafiqueNo ratings yet
- BED 4107 Gerontology Lecture Notes MARCH 2020Document40 pagesBED 4107 Gerontology Lecture Notes MARCH 2020SHARON KIHORONo ratings yet
- Chapter 3 Consumer BehaviorDocument61 pagesChapter 3 Consumer BehaviorFatima AbboudNo ratings yet
- Mark Scheme (Results) Summer 2021Document25 pagesMark Scheme (Results) Summer 2021Gaia PhyllisNo ratings yet
- Chapter 14 - The Somatic Nervous SystemDocument55 pagesChapter 14 - The Somatic Nervous SystemTH TNo ratings yet
- Science 10 Q3 Week 3Document14 pagesScience 10 Q3 Week 3Crislan D. VillalonNo ratings yet