Download as pdf or txt
You might also like
- (Download PDF) Dog Parasites Endangering Human Health Christina Strube Online Ebook All Chapter PDFDocument39 pages(Download PDF) Dog Parasites Endangering Human Health Christina Strube Online Ebook All Chapter PDFlee.hume439100% (10)
- Basic and Compulsory Registration of 2004 2016Document27 pagesBasic and Compulsory Registration of 2004 2016BA Ong50% (4)
- Lymph Node Pathology PDFDocument4 pagesLymph Node Pathology PDFKeserovic AdmirNo ratings yet
- Step1 Review TopicsDocument32 pagesStep1 Review TopicsAsif AbidiNo ratings yet
- Treatment of Chronic Heart FailureDocument2 pagesTreatment of Chronic Heart FailureShannon RamsumairNo ratings yet
- Uworld EndocrineDocument211 pagesUworld Endocrineهنادي رازمNo ratings yet
- Hyperthyroidism Deranged PhysiologyDocument11 pagesHyperthyroidism Deranged PhysiologyManisha Sekaran Muniandy100% (1)
- Respiratory Tract InfectionsDocument1 pageRespiratory Tract InfectionsShannon RamsumairNo ratings yet
- Pathogens of The Vagina-Annie Espinosa - This Is The Revised VersionDocument1 pagePathogens of The Vagina-Annie Espinosa - This Is The Revised VersionMicroposterNo ratings yet
- Adult Bradycardia Algorithm: Identify and Treat Underlying CauseDocument1 pageAdult Bradycardia Algorithm: Identify and Treat Underlying CausenebrasNo ratings yet
- Abnormal LFTsDocument2 pagesAbnormal LFTsRenu RosyNo ratings yet
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedNo ratings yet
- IKD9 - Radiological Evaluation of Renal CystsDocument26 pagesIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusNo ratings yet
- First Aid PharmacoDocument61 pagesFirst Aid PharmacogirNo ratings yet
- Gyne - Case 11 Lower Genital UTI PDFDocument2 pagesGyne - Case 11 Lower Genital UTI PDFcbac1990No ratings yet
- Kidney TumorsDocument15 pagesKidney TumorsJose SirittNo ratings yet
- PnemoniaDocument4 pagesPnemoniadhavalNo ratings yet
- Increased ICP: A) HeadacheDocument5 pagesIncreased ICP: A) Headachemohamed nagyNo ratings yet
- Week 7. Renal Pathology Continued.Document9 pagesWeek 7. Renal Pathology Continued.Amber LeJeuneNo ratings yet
- Respiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDocument12 pagesRespiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDoc JacqueNo ratings yet
- Heart SoundsDocument2 pagesHeart Soundsdanny_awwadNo ratings yet
- LeukemiasDocument8 pagesLeukemiasMoonyeen Jann Casera BalicNo ratings yet
- Respiratory PathophysDocument1 pageRespiratory PathophysTori IkeharaNo ratings yet
- Essentials of Respiratory SystemDocument138 pagesEssentials of Respiratory SystemMuhammad Ahmad bin makruf syammakuNo ratings yet
- Acute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmDocument1 pageAcute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmAudreySlitNo ratings yet
- Week 10 - Hypertension, Atherosclerosis, ArrhythmiaDocument14 pagesWeek 10 - Hypertension, Atherosclerosis, Arrhythmiashivani patel100% (1)
- ACLS AgorithmDocument55 pagesACLS AgorithmkpsuanNo ratings yet
- ENDOCRINE PATHOLOGY WebpathDocument35 pagesENDOCRINE PATHOLOGY Webpathapi-3766657No ratings yet
- LV RV FailureDocument118 pagesLV RV FailureMirza Thaariq HapsitoNo ratings yet
- Neurology Musculoskeletal (MedicalBooksVN - Com)Document4 pagesNeurology Musculoskeletal (MedicalBooksVN - Com)Jonathan AiresNo ratings yet
- Electrolyte DisordersDocument10 pagesElectrolyte DisordersSlavicaNo ratings yet
- Valvular Heart DseDocument8 pagesValvular Heart DseJane Pineda CuraNo ratings yet
- Vasculitis: Disorder Vessels Pathology Presentation Test TX OtherDocument3 pagesVasculitis: Disorder Vessels Pathology Presentation Test TX OthermcwnotesNo ratings yet
- Medicine Epidemiology (MedicalBooksVN - Com)Document34 pagesMedicine Epidemiology (MedicalBooksVN - Com)Jonathan AiresNo ratings yet
- ACLS Drug TherapyDocument8 pagesACLS Drug TherapySahrensNo ratings yet
- Renal SyndromeDocument13 pagesRenal SyndromeAndreas KristianNo ratings yet
- Enzyme Deficiencies of Glycolysis and TCA: D N D S /SDocument8 pagesEnzyme Deficiencies of Glycolysis and TCA: D N D S /SJordan WhiteNo ratings yet
- Cardio Day 3 TemplateDocument24 pagesCardio Day 3 TemplateMikeNo ratings yet
- Systemic Lupus Erythematosus Lecture Salah Abdel BakyDocument8 pagesSystemic Lupus Erythematosus Lecture Salah Abdel Bakyahmed gabrNo ratings yet
- VQ - O2 GradientDocument27 pagesVQ - O2 GradientIkbal NurNo ratings yet
- Abg InterpretationDocument1 pageAbg InterpretationPrincess EspadaNo ratings yet
- Antiarrhythmic Drugs: 1A: Prolong AP & Increase Refractory Period Moderate Effects On Conduction in Normal CellsDocument6 pagesAntiarrhythmic Drugs: 1A: Prolong AP & Increase Refractory Period Moderate Effects On Conduction in Normal CellsSaulNo ratings yet
- Disorders of Motility2Document46 pagesDisorders of Motility2valdomiroNo ratings yet
- Cardiovascular Nursing: Study Online atDocument7 pagesCardiovascular Nursing: Study Online atLilly DayeNo ratings yet
- Pathology of The Lung: Djumadi AchmadDocument26 pagesPathology of The Lung: Djumadi AchmadVivi DeviyanaNo ratings yet
- Nephrotic Syndrome WikipediaDocument10 pagesNephrotic Syndrome WikipediaJohn KevlarNo ratings yet
- 5MechanismsOfHypoxemia PDFDocument1 page5MechanismsOfHypoxemia PDFHanan ibrahimNo ratings yet
- Test LFTsDocument2 pagesTest LFTsostarburstoNo ratings yet
- Pneumothorax & Hemothorax: Farshid MokhberiDocument32 pagesPneumothorax & Hemothorax: Farshid MokhberiYan Sheng HoNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- SLE Pathogenesis, Clinical FeaturesDocument30 pagesSLE Pathogenesis, Clinical FeaturesJuwita PratiwiNo ratings yet
- AtelectasisDocument3 pagesAtelectasisLouis FortunatoNo ratings yet
- MIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenDocument8 pagesMIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenJosselle Sempio CalientaNo ratings yet
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 pagesClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiNo ratings yet
- Atypical PneumoniaDocument30 pagesAtypical PneumoniachandanNo ratings yet
- Hem/Onc USML Organization ChartDocument1 pageHem/Onc USML Organization ChartJJNo ratings yet
- Chronic Myelogenous Leukemia (CML) - Causes, Symptoms, TreatmentDocument10 pagesChronic Myelogenous Leukemia (CML) - Causes, Symptoms, Treatmentnurul auliaNo ratings yet
- Im-Ugib PudDocument6 pagesIm-Ugib PudTrisNo ratings yet
- Fluid and Electrolyte DisordersDocument47 pagesFluid and Electrolyte DisordersMarc Imhotep Cray, M.D.No ratings yet
- Therapeutic Hypothermia - Principles, Indications, Practical ApplicationFrom EverandTherapeutic Hypothermia - Principles, Indications, Practical ApplicationNo ratings yet
- The Leukotrienes: Chemistry and BiologyFrom EverandThe Leukotrienes: Chemistry and BiologyLawrence ChakrinNo ratings yet
- Seziures: Status Epilepticus Status EpilepticusDocument2 pagesSeziures: Status Epilepticus Status EpilepticusEna PaparićNo ratings yet
- Pathogenesis of DermatophytesDocument1 pagePathogenesis of DermatophytesEna PaparićNo ratings yet
- Hyperpitutiarism & Pituitary Adenmoas: Pathogenesis MorphologyDocument2 pagesHyperpitutiarism & Pituitary Adenmoas: Pathogenesis MorphologyEna PaparićNo ratings yet
- 1-Astrocytomas 2 - Oligodendrogliomas 3 - Ependymomas: GliomasDocument2 pages1-Astrocytomas 2 - Oligodendrogliomas 3 - Ependymomas: GliomasEna PaparićNo ratings yet
- Classification of AnemiaDocument4 pagesClassification of AnemiaEna PaparićNo ratings yet
- Fill Me UP - Angel - VIllaverdeDocument3 pagesFill Me UP - Angel - VIllaverdeGel MadrigalNo ratings yet
- LD Implant FailuresDocument152 pagesLD Implant Failureswasim hussainNo ratings yet
- Dopamine and Its Functions Dopamine Is A Neurotransmitter (Or Chemical Messenger) and "Feel GoodDocument3 pagesDopamine and Its Functions Dopamine Is A Neurotransmitter (Or Chemical Messenger) and "Feel Goodiqra asifNo ratings yet
- Group Case StudyDocument5 pagesGroup Case StudySiti SurayaNo ratings yet
- Literature Review of Obesity in MalaysiaDocument4 pagesLiterature Review of Obesity in Malaysiac5p0cd99100% (1)
- Cancers 14 04391 v2Document14 pagesCancers 14 04391 v2Arthur FreemanNo ratings yet
- Hemokromatosis PDFDocument32 pagesHemokromatosis PDFyogi gestiawanNo ratings yet
- Semi-Detailed Lesson Plan in MAPEH 7 (4a's Lesson Plan)Document7 pagesSemi-Detailed Lesson Plan in MAPEH 7 (4a's Lesson Plan)PatzAlzateParaguyaNo ratings yet
- Open - Oregonstate.education-Foundations of EpidemiologyDocument11 pagesOpen - Oregonstate.education-Foundations of EpidemiologyAMANE COTTAGE HOSPITALNo ratings yet
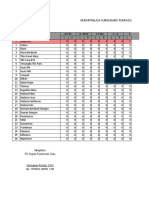
- Laporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuDocument37 pagesLaporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuVictoria YanersNo ratings yet
- Answer-Test 6-G7Document3 pagesAnswer-Test 6-G7Ly NguyenTong2512No ratings yet
- Aiims SkinDocument85 pagesAiims SkinSagar MukherjeeNo ratings yet
- BY: Reem Almutairi Amal Alanazi DR: SaraDocument7 pagesBY: Reem Almutairi Amal Alanazi DR: Sarareem almutairiNo ratings yet
- اسئلة تمريض البالغين - تجريبيDocument10 pagesاسئلة تمريض البالغين - تجريبيمحمد باقر -Mohammed paqierNo ratings yet
- 3 - Child AbuseDocument33 pages3 - Child AbuseAmmar AlnajjarNo ratings yet
- Stress DiffinitionDocument7 pagesStress DiffinitionNajib BaddouNo ratings yet
- 10.epidemiology of Malocclusion PDFDocument5 pages10.epidemiology of Malocclusion PDFhassankhan9849No ratings yet
- Raghav GuptaDocument1 pageRaghav GuptaLABNo ratings yet
- Down SyndromeDocument17 pagesDown SyndromeSarah Shine TorresNo ratings yet
- CRISPR Cas-9 and DMDocument19 pagesCRISPR Cas-9 and DMIbraheem KaisNo ratings yet
- CURB-65 Score For Pneumonia Score DescriptionDocument14 pagesCURB-65 Score For Pneumonia Score DescriptionMelvin CarewNo ratings yet
- Table of Content: Risk AssesmentDocument25 pagesTable of Content: Risk AssesmentvijayNo ratings yet
- Nekky ExselDocument217 pagesNekky ExselpokjarspkNo ratings yet
- Sindrome Cloccs RadiographicsDocument20 pagesSindrome Cloccs RadiographicsJEAN CARLOS GALLO VALVERDENo ratings yet
- Renal Function TestsDocument38 pagesRenal Function TestsSupriya NayakNo ratings yet
- Malaria Diagnosis (U.S.) - Rapid Diagnostic TestDocument3 pagesMalaria Diagnosis (U.S.) - Rapid Diagnostic TestAkindele O AdigunNo ratings yet
- Clinical Roundup Rheumatoid ArthritisDocument7 pagesClinical Roundup Rheumatoid ArthritisSrikesav SivakumarNo ratings yet
- SonapDocument3 pagesSonaped jireh nangcaNo ratings yet