Download as docx, pdf, or txt
You might also like
- John Bird Published by Taylor and FrancisDocument9 pagesJohn Bird Published by Taylor and FrancisromwamaNo ratings yet
- Concise Definitive Review: Stress Ulcer ProphylaxisDocument11 pagesConcise Definitive Review: Stress Ulcer ProphylaxisMuhammad Umar RazaNo ratings yet
- Creating and Configuring A BACnet Network With b3 BACnet Devices Tutorial GuideDocument212 pagesCreating and Configuring A BACnet Network With b3 BACnet Devices Tutorial GuideDGG50% (2)
- 80k+ Priv8 IPTV (Userpass) CombolistDocument1,472 pages80k+ Priv8 IPTV (Userpass) CombolistJohn AndresNo ratings yet
- Stress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewDocument9 pagesStress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewIkrima MuhdarmuhallyNo ratings yet
- Proton Pump Inhibitors To Prevent Gastrointestinal Bleeding - AnDocument13 pagesProton Pump Inhibitors To Prevent Gastrointestinal Bleeding - AnRielc zemartinNo ratings yet
- Oral Presentations: Résumés Scientifique 2020Document1 pageOral Presentations: Résumés Scientifique 2020JOHN ALEC FORTONo ratings yet
- Stress Ulcer Prophylaxis in The New Millennium A20Document7 pagesStress Ulcer Prophylaxis in The New Millennium A20ellenasbNo ratings yet
- Biomedical Res 2019 30 1 6-10Document5 pagesBiomedical Res 2019 30 1 6-10Fernando SousaNo ratings yet
- Pi Is 0016508520300184Document12 pagesPi Is 0016508520300184ntnquynhproNo ratings yet
- Ni 2016 (2) (CRE)Document10 pagesNi 2016 (2) (CRE)Nattawat TeerawattanapongNo ratings yet
- CX VS No CXDocument9 pagesCX VS No CXJeimy CarvajalNo ratings yet
- Journal Pmed 1003501Document28 pagesJournal Pmed 1003501Abi HinojosaNo ratings yet
- Favilla 2015Document2 pagesFavilla 2015DavorIvanićNo ratings yet
- Singh2020 Colitis UlseratifDocument19 pagesSingh2020 Colitis UlseratifFriska AirynNo ratings yet
- Ournal of Linical Ncology: PurposeDocument11 pagesOurnal of Linical Ncology: PurposeRicky Cornelius TariganNo ratings yet
- PB3 7820 R2Document10 pagesPB3 7820 R2Lissaberti AmaliahNo ratings yet
- Anticoagulation Versus No Anticoagulation For.25Document2 pagesAnticoagulation Versus No Anticoagulation For.25Dr WittyNo ratings yet
- 10 1016@j Clinthera 2020 01 008Document19 pages10 1016@j Clinthera 2020 01 008skripsi kapNo ratings yet
- American College of Gastroenterology Guidelines: Management of Acute PancreatitisDocument16 pagesAmerican College of Gastroenterology Guidelines: Management of Acute PancreatitisCarinka VidañosNo ratings yet
- 158 Nausea - Vomiting ScaleDocument9 pages158 Nausea - Vomiting ScaleMas Indra ShuNo ratings yet
- Khan 2004Document8 pagesKhan 2004BENNY MAHENDRANo ratings yet
- Samrt 2Document9 pagesSamrt 2Zai RojasNo ratings yet
- Aliment Pharmacol Ther - 2024 - Shung - Review Article Upper Gastrointestinal Bleeding Review of Current Evidence andDocument20 pagesAliment Pharmacol Ther - 2024 - Shung - Review Article Upper Gastrointestinal Bleeding Review of Current Evidence andDiana AvilesNo ratings yet
- Rapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of LifeDocument8 pagesRapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of Lifejamie carpioNo ratings yet
- ACG Clinical Guideline: Management of Acute PancreatitisDocument8 pagesACG Clinical Guideline: Management of Acute PancreatitisNick ANo ratings yet
- Art 16Document3 pagesArt 16Arenita°°°No ratings yet
- Revision Bibliografica JUNIO 2022Document12 pagesRevision Bibliografica JUNIO 2022Sergio Herrero BermejoNo ratings yet
- Liu Et Al 2015 Comparison of Multislice Computed Tomography and Clinical Scores For Diagnosing Acute AppendicitisDocument9 pagesLiu Et Al 2015 Comparison of Multislice Computed Tomography and Clinical Scores For Diagnosing Acute AppendicitisNovi OktaviantiNo ratings yet
- Sadeghi 2019Document12 pagesSadeghi 2019Nejc KovačNo ratings yet
- Art2 HT3Document3 pagesArt2 HT3Glenda MaríaNo ratings yet
- Prolonged Effects of A Home-Based Intervention in Patients With Chronic IllnessDocument6 pagesProlonged Effects of A Home-Based Intervention in Patients With Chronic IllnessmartingomezrNo ratings yet
- Intervenciones para El Reflujo Primario VesicoureteralDocument12 pagesIntervenciones para El Reflujo Primario VesicoureteralArmando FigueroaNo ratings yet
- ForrestDocument4 pagesForrestAbulHasan Idrus IstarNo ratings yet
- Thrombosis Research: Siavash Piran, MD, MSC, Sam Schulman, MD, PHDDocument5 pagesThrombosis Research: Siavash Piran, MD, MSC, Sam Schulman, MD, PHDYANNo ratings yet
- Acute Appendicitis in Adults - Diagnostic Evaluation - UpToDateDocument16 pagesAcute Appendicitis in Adults - Diagnostic Evaluation - UpToDateJuanCarlosNúñezNo ratings yet
- Iarjmsr 1 (3) 106-108Document2 pagesIarjmsr 1 (3) 106-108jinuNo ratings yet
- Prevalence and Risk FactorsDocument7 pagesPrevalence and Risk FactorsFlick Jr Jr.No ratings yet
- Chapter 3 - Evidence-Based Endocrinology and Clinical EpidemiologyDocument32 pagesChapter 3 - Evidence-Based Endocrinology and Clinical Epidemiology張宏軒No ratings yet
- Point-Of-Care Diagnostic Tests For Influenza in The Emergency DepartmentDocument15 pagesPoint-Of-Care Diagnostic Tests For Influenza in The Emergency DepartmentCristiano NogueiraNo ratings yet
- The Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisDocument4 pagesThe Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisAracelyAcostaNo ratings yet
- Prognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumDocument14 pagesPrognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumChris El HadiNo ratings yet
- Noninvasive Monitoring 2016Document6 pagesNoninvasive Monitoring 2016Maria LaiaNo ratings yet
- Articulo 3Document4 pagesArticulo 3Ricardo Sanchez MontoyaNo ratings yet
- HPV Vaccine Programmes - Current Scenario and Recommendations in IndiaDocument3 pagesHPV Vaccine Programmes - Current Scenario and Recommendations in Indiash19782001No ratings yet
- A Prospective Randomized Controlled Trial On The Value of Prophylactic Supplementation Pral NutritionDocument7 pagesA Prospective Randomized Controlled Trial On The Value of Prophylactic Supplementation Pral NutritionOkky IrawanNo ratings yet
- A Systematic Overview of Chemotherapy Effects inDocument22 pagesA Systematic Overview of Chemotherapy Effects inRutuja KuhikarNo ratings yet
- Huang 2019Document10 pagesHuang 2019blume diaNo ratings yet
- Delayed Vs Immediate Umbilical Cord ClampingDocument37 pagesDelayed Vs Immediate Umbilical Cord ClampingAndi DeviriyantiNo ratings yet
- The Clinical Outcomes and Predictive Factors For.24Document5 pagesThe Clinical Outcomes and Predictive Factors For.24KeziaNo ratings yet
- Early Referral To A Palliative Team Improves End-Of-life Care Among Gynecological Cancer PatientsDocument11 pagesEarly Referral To A Palliative Team Improves End-Of-life Care Among Gynecological Cancer PatientsArmando José MaldonadoNo ratings yet
- CC 9312Document10 pagesCC 9312Fitrianto Dwi UtomoNo ratings yet
- Early Enteral Nutrition Compared With Parenteral Nutrition For Esophageal Cancer Patients After Esophagectomy: A Meta-AnalysisDocument9 pagesEarly Enteral Nutrition Compared With Parenteral Nutrition For Esophageal Cancer Patients After Esophagectomy: A Meta-AnalysisEndah Rahayu MulyaniNo ratings yet
- Relationship Between CRP and A Lin Routine Abdominal Procedures A Systematic AnalysisDocument7 pagesRelationship Between CRP and A Lin Routine Abdominal Procedures A Systematic AnalysisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 847-Article Text-1307-1-10-20180513Document4 pages847-Article Text-1307-1-10-20180513sf228No ratings yet
- Ramirez 2013Document10 pagesRamirez 2013Nadia Farah FadhilaNo ratings yet
- Terapia de Vacio en TraumaDocument11 pagesTerapia de Vacio en TraumaImha MikanersandsmashblastNo ratings yet
- International Wound Journal - 2023 - Gao - The Effects of Evidence Based Nursing Interventions On Pressure Ulcers inDocument8 pagesInternational Wound Journal - 2023 - Gao - The Effects of Evidence Based Nursing Interventions On Pressure Ulcers inahmadalipoland25No ratings yet
- Asia-Pacific Consensus Statements On Crohn's Disease. Part 2: ManagementDocument13 pagesAsia-Pacific Consensus Statements On Crohn's Disease. Part 2: ManagementtiaraNo ratings yet
- Prevención de Ulceras de Estrés en El Paciente NeurocriticoDocument14 pagesPrevención de Ulceras de Estrés en El Paciente NeurocriticoVlady78No ratings yet
- Abdominal Sepsis Prognostic FactorDocument6 pagesAbdominal Sepsis Prognostic FactorPrasojo JojoNo ratings yet
- Lammers 2014Document9 pagesLammers 2014DavorIvanićNo ratings yet
- Gas/Liquid Separators: Quantifying Separation Performance - Part 1Document10 pagesGas/Liquid Separators: Quantifying Separation Performance - Part 1sara25dec689288No ratings yet
- LSP 401 Ip S1 12-13Document4 pagesLSP 401 Ip S1 12-13Mary TeohNo ratings yet
- Promotion Safe Med ChildrensDocument64 pagesPromotion Safe Med ChildrensAbdul khodir jaelani100% (1)
- Microsoft - Testinises.az 900.vce - Download.2021 May 25.by - Max.132q.vceDocument10 pagesMicrosoft - Testinises.az 900.vce - Download.2021 May 25.by - Max.132q.vceGowri Prasanth ChaduvulaNo ratings yet
- 1sem-Tata Motors-Emerging MarketsDocument25 pages1sem-Tata Motors-Emerging MarketsAayush SisodiaNo ratings yet
- Schindler Escalator 9700AE - Brake MaintenanceDocument4 pagesSchindler Escalator 9700AE - Brake MaintenanceHùng VĩNo ratings yet
- Pa2200-Series ManualDocument178 pagesPa2200-Series ManualtatfutureNo ratings yet
- Yashoda Singh Indian Coins Lots 1001-1242Document29 pagesYashoda Singh Indian Coins Lots 1001-1242Ashwin SevariaNo ratings yet
- Dubai Workshop RegistrationDocument2 pagesDubai Workshop RegistrationmfkmughalNo ratings yet
- Important Questions For MID I CNDocument14 pagesImportant Questions For MID I CN20H51A0540-NAKKA SREEKAR B.Tech CSE (2020-24)No ratings yet
- Pre Board POL - SCI Paper 2Document6 pagesPre Board POL - SCI Paper 2harsh jatNo ratings yet
- Intermediate Accounting Reporting and Analysis 3Rd Edition James Wahlen Full ChapterDocument67 pagesIntermediate Accounting Reporting and Analysis 3Rd Edition James Wahlen Full Chapterwilliam.rodriquez579100% (6)
- A Review of Jet Mixing Enhancement For Aircraft Propulsion ApplicationsDocument25 pagesA Review of Jet Mixing Enhancement For Aircraft Propulsion ApplicationsJINU CHANDRANNo ratings yet
- PPE Lab ManualDocument27 pagesPPE Lab ManualDinesh Chavhan100% (1)
- Gerund NounDocument15 pagesGerund NounNanda PutriNo ratings yet
- PSS5000-USGU LicenseKey Installation 80558701Document10 pagesPSS5000-USGU LicenseKey Installation 80558701LongNo ratings yet
- MIT Insight Report On (Chemistry) Industry DigitalizationDocument21 pagesMIT Insight Report On (Chemistry) Industry DigitalizationEllezah Dela CruzNo ratings yet
- Bendix Actuator Competitive Cross Reference ListDocument1 pageBendix Actuator Competitive Cross Reference ListFernando PadillaNo ratings yet
- Asterisk For Dumb MeDocument164 pagesAsterisk For Dumb MeAndy CockroftNo ratings yet
- Chapter 3 CVPDocument26 pagesChapter 3 CVPshuhadaNo ratings yet
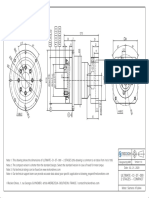
- ULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Document1 pageULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Francesco SchioppaNo ratings yet
- Hardness TestDocument8 pagesHardness TestlvasuthavanNo ratings yet
- Financial Summary Statement Period 03/10/23 - 04/09/23: Deposit Accounts Total DepositsDocument14 pagesFinancial Summary Statement Period 03/10/23 - 04/09/23: Deposit Accounts Total DepositsLuis RodríguezNo ratings yet
- ABLRFD v1403 Summary RevisionsDocument2 pagesABLRFD v1403 Summary RevisionsMiguel AngelNo ratings yet
- 2021 YISS - INTRODUCTION TO COMPUTER GRAPHICS - Hyunjung KimDocument3 pages2021 YISS - INTRODUCTION TO COMPUTER GRAPHICS - Hyunjung KimFung AlexNo ratings yet
- Veritas NetBackup 6.5 Vault Administrator's GuideDocument268 pagesVeritas NetBackup 6.5 Vault Administrator's GuideS LS ChanNo ratings yet
- Introduction To Time and Frequency MetrologyDocument30 pagesIntroduction To Time and Frequency MetrologyJBSfanNo ratings yet