Download as pdf or txt
You might also like
- NBME 14 - AnswersDocument208 pagesNBME 14 - Answersmerontesfaye5150% (2)
- Importance of OHSDocument45 pagesImportance of OHSChloe OlazoNo ratings yet
- Chronic Benign Paroxysmal Positional Vertigo (BPPVDocument2 pagesChronic Benign Paroxysmal Positional Vertigo (BPPVicarosalernoNo ratings yet
- Jurnal AE 2Document3 pagesJurnal AE 2Mira Mariana UlfahNo ratings yet
- Abdominal EpilepsyDocument4 pagesAbdominal EpilepsyErnesto Ochoa MonroyNo ratings yet
- 19-Year-Old Female With Abdominal PainDocument7 pages19-Year-Old Female With Abdominal PainAdrian Florin DobrescuNo ratings yet
- Epileptic Disorders - 2023 - Tena Cucala - Eating Induced Seizures A Semiological Sign of The Right Temporal PoleDocument12 pagesEpileptic Disorders - 2023 - Tena Cucala - Eating Induced Seizures A Semiological Sign of The Right Temporal PoleMoileon2011No ratings yet
- Hiccup Due To Gastroesophageal Reflux Disease: Cem Koçkar, Mehmet İşler, Erkan Cüre, Altuğ Şenol, Abdulkadir BaştürkDocument3 pagesHiccup Due To Gastroesophageal Reflux Disease: Cem Koçkar, Mehmet İşler, Erkan Cüre, Altuğ Şenol, Abdulkadir Baştürkelisabeth stefaniNo ratings yet
- General Medicine - 2013 - Shikino - Chest Pain The Only Symptom of Gastric UlcerDocument3 pagesGeneral Medicine - 2013 - Shikino - Chest Pain The Only Symptom of Gastric UlcerDavid UkaegbuNo ratings yet
- Sacral Neuromodulation For Bowel Dysfunction: Weledji EP and Marti LDocument11 pagesSacral Neuromodulation For Bowel Dysfunction: Weledji EP and Marti LPetrina Theda PhilothraNo ratings yet
- Ictal Urinary Urge Indicates Seizure Onset in The Nondominant Temporal LobeDocument5 pagesIctal Urinary Urge Indicates Seizure Onset in The Nondominant Temporal LobejerejerejereNo ratings yet
- Approach To Acute Abdominal Pain: Robert Mcnamara,, Anthony J. DeanDocument15 pagesApproach To Acute Abdominal Pain: Robert Mcnamara,, Anthony J. DeanNataly VanesaNo ratings yet
- Surg 02 Manifestations of Gastrointestinal Diseases 2016 PDFDocument85 pagesSurg 02 Manifestations of Gastrointestinal Diseases 2016 PDFMarian Dane PunzalanNo ratings yet
- 7914 Chap01 PDFDocument21 pages7914 Chap01 PDFdoctordilafrozaNo ratings yet
- PaparDocument7 pagesPaparishitaNo ratings yet
- CT Mesenteroaxial GVDocument6 pagesCT Mesenteroaxial GVkueputuNo ratings yet
- Gastrointestinal Manifestations in ChildDocument5 pagesGastrointestinal Manifestations in ChildSwathi GeethaNo ratings yet
- Dr. Arun Aggarwal Gastroenterologist Explains The Electrogastrogram (EGG) Which Is The Graphic Producer of StomachDocument45 pagesDr. Arun Aggarwal Gastroenterologist Explains The Electrogastrogram (EGG) Which Is The Graphic Producer of StomachDr. Arun Aggarwal GastroenterologistNo ratings yet
- J Neurol Neurosurg Psychiatry 1987 Torrealba 1539 41Document4 pagesJ Neurol Neurosurg Psychiatry 1987 Torrealba 1539 41Mihaela LitovcencoNo ratings yet
- Abdominal PainDocument15 pagesAbdominal PainLina E. ArangoNo ratings yet
- Pub Med 1Document4 pagesPub Med 1Kaouther KiouaneNo ratings yet
- Bab 1Document31 pagesBab 1PandeNo ratings yet
- DM Hiperestesia 4 PDFDocument6 pagesDM Hiperestesia 4 PDFSyahrul Hamidi NasutionNo ratings yet
- Vestibular Neuronitis: Basic Information DiagnosisDocument2 pagesVestibular Neuronitis: Basic Information DiagnosisKamilah HaniyahNo ratings yet
- Acute Unilateral Vestibulopathy Strupp & Magnusson (2015)Document17 pagesAcute Unilateral Vestibulopathy Strupp & Magnusson (2015)J WNo ratings yet
- MainDocument3 pagesMainUaga FerigeNo ratings yet
- Pathologic and Paralytic Ileus: Ackie OODDocument2 pagesPathologic and Paralytic Ileus: Ackie OODwafasahilahNo ratings yet
- 631-Article Text-2378-1-10-20180830Document6 pages631-Article Text-2378-1-10-20180830azizhamoudNo ratings yet
- Clinical Evaluation of Acute Appendicitis 2014Document8 pagesClinical Evaluation of Acute Appendicitis 2014maithamNo ratings yet
- Nursing AssessmentDocument10 pagesNursing AssessmentDian WidyaNo ratings yet
- Sleep and Epilepsy: Sejal V. Jain, MD, and Sanjeev V. Kothare, MDDocument7 pagesSleep and Epilepsy: Sejal V. Jain, MD, and Sanjeev V. Kothare, MDRezky 'kiki' Oktarianti SyahputriNo ratings yet
- HP 200706 CausesDocument4 pagesHP 200706 CausesDALIA USAMANo ratings yet
- HP 200706 CausesDocument4 pagesHP 200706 CausesDALIA USAMANo ratings yet
- BiofeedbackDocument17 pagesBiofeedbackDavid Andrés Bessalle ReyesNo ratings yet
- Wernicke'S Encephalopathy: A Case Report and Mri Findings: Key-Words: Pregnancy, Complications - Brain, DiseasesDocument2 pagesWernicke'S Encephalopathy: A Case Report and Mri Findings: Key-Words: Pregnancy, Complications - Brain, DiseasesebrozanNo ratings yet
- Vagal Tone Effects On Sensitivity, Motility, and InflammationDocument8 pagesVagal Tone Effects On Sensitivity, Motility, and InflammationGuillermo923No ratings yet
- Ni Hms 815992Document18 pagesNi Hms 815992Taufik 81No ratings yet
- Seizure PathophysiologyDocument26 pagesSeizure PathophysiologyNarianne Mae Solis Bedoy100% (1)
- Case 1Document4 pagesCase 1Irsanti SasmitaNo ratings yet
- CBD NeuropediatriDocument34 pagesCBD NeuropediatriyayanaryanNo ratings yet
- Gastric Volvulus: Bang Chau, Susan DufelDocument2 pagesGastric Volvulus: Bang Chau, Susan DufelmustikaarumNo ratings yet
- ACNS Neonatal EEG GuidelinesDocument40 pagesACNS Neonatal EEG Guidelinesseemee23820No ratings yet
- Use of Dr. Tans Chinese Balance AcupunctDocument9 pagesUse of Dr. Tans Chinese Balance AcupunctrendaoNo ratings yet
- Case Report ASMIHA 2022Document1 pageCase Report ASMIHA 2022Ghina NinditasariNo ratings yet
- Amalia Lystiana Dewi Syarief Mahmud MakkaDocument20 pagesAmalia Lystiana Dewi Syarief Mahmud MakkaamieNo ratings yet
- Acute Encephalopathy Preceding Infection: ShigellaDocument2 pagesAcute Encephalopathy Preceding Infection: ShigellaOasis LimitedNo ratings yet
- Late-Onset Rasmussen's Encephalitis and Long-Term Remission: Clinical CommentaryDocument4 pagesLate-Onset Rasmussen's Encephalitis and Long-Term Remission: Clinical CommentarySana ShafeeqNo ratings yet
- Acute Abdomen: DR Teamir Negussie Assistant Professor Dept of SurgeryDocument69 pagesAcute Abdomen: DR Teamir Negussie Assistant Professor Dept of SurgeryteamirNo ratings yet
- Non-Epileptic Paroxysmal Manifestations During Sleep in Infancy and ChildhoodDocument5 pagesNon-Epileptic Paroxysmal Manifestations During Sleep in Infancy and ChildhoodSimina SerbanNo ratings yet
- GB SyndromDocument5 pagesGB Syndromavinash dhameriyaNo ratings yet
- 1 s2.0 S1389945717302496 Main PDFDocument3 pages1 s2.0 S1389945717302496 Main PDFvalentinaNo ratings yet
- 2014 Calcium Channel Proteins Mediate Trigeminal Neuropathic Pain States Associated With Aberrant Excitatory SynaptogenesisDocument13 pages2014 Calcium Channel Proteins Mediate Trigeminal Neuropathic Pain States Associated With Aberrant Excitatory SynaptogenesisCristian OyarzoNo ratings yet
- Vertigo: A Review of Common Peripheral and Central Vestibular DisordersDocument7 pagesVertigo: A Review of Common Peripheral and Central Vestibular DisordersPutra ImanullahNo ratings yet
- Obstructive Sleep Apnoea SyndromeDocument72 pagesObstructive Sleep Apnoea SyndromeArjun SainiNo ratings yet
- A Middle Aged Woman With Nausea Weight Loss and Orthostatic HypotensionDocument7 pagesA Middle Aged Woman With Nausea Weight Loss and Orthostatic Hypotensioniri_balNo ratings yet
- Review Article The Management of Pelvic Floor DisordersDocument15 pagesReview Article The Management of Pelvic Floor DisordersYvonne MedinaNo ratings yet
- Seizures in Pregnancy: Epilepsy, Eclampsia, and Stroke: Laura A. Hart, MD, and Baha M. Sibai, MDDocument18 pagesSeizures in Pregnancy: Epilepsy, Eclampsia, and Stroke: Laura A. Hart, MD, and Baha M. Sibai, MDFannyZamoraGranielNo ratings yet
- IICBS Summaries: Nausea, Vomiting, and Indigestion by William HaslerDocument42 pagesIICBS Summaries: Nausea, Vomiting, and Indigestion by William HaslerRaymond Lorenzo N. RacelaNo ratings yet
- L2 Worksheet For Online Discussion - Qns - 13.2.2020 v3Document8 pagesL2 Worksheet For Online Discussion - Qns - 13.2.2020 v3CHUN TO HONo ratings yet
- 2000 Brain ALSDocument16 pages2000 Brain ALSSultan TarlacıNo ratings yet
- Profopol Vs KTMDocument7 pagesProfopol Vs KTMAuliaRusdiAllmuttaqienNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Mohammed Ismail VaseemNo ratings yet
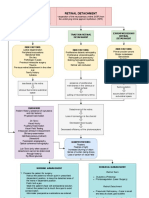
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- AlcoholismDocument30 pagesAlcoholism1S VILLEGAS GabrielNo ratings yet
- 纽约时报 New York TimesDocument6 pages纽约时报 New York TimesMauricio PadronNo ratings yet
- Human Biology & Frequency Healing - POOR MAN'S ZAPPER - Low-Tech Rife Generator AlternativeDocument2 pagesHuman Biology & Frequency Healing - POOR MAN'S ZAPPER - Low-Tech Rife Generator AlternativeJulio LoraNo ratings yet
- 7.stool Examination - Morphology of Eggs, Cysts, LarvaeDocument9 pages7.stool Examination - Morphology of Eggs, Cysts, LarvaeKowshik AvulaNo ratings yet
- 526 PDFDocument11 pages526 PDFMilton CrutchfieldNo ratings yet
- Nursing Diagnosis Nursing Intervention Rationale Ineffective Airway ClearanceDocument2 pagesNursing Diagnosis Nursing Intervention Rationale Ineffective Airway ClearanceJoshua VillarbaNo ratings yet
- Hemşirelik Bölümü Ders İçerikleri (İngilizce)Document52 pagesHemşirelik Bölümü Ders İçerikleri (İngilizce)teomanbilimNo ratings yet
- The Association Between Diabetic Retinopathy, Cognitive Impairment, and Quality of Life A Cross Sectional StudyDocument5 pagesThe Association Between Diabetic Retinopathy, Cognitive Impairment, and Quality of Life A Cross Sectional StudyppdsretinaNo ratings yet
- Eating Behaviors Vol.08 Issue 1 200701 14710153 PDFDocument143 pagesEating Behaviors Vol.08 Issue 1 200701 14710153 PDFdolores silviaNo ratings yet
- DNB Final Theory Papers Ophthalmology 2011 2020Document160 pagesDNB Final Theory Papers Ophthalmology 2011 2020Rekha JakharNo ratings yet
- 2 Davao City Health - Case Investigation FormDocument3 pages2 Davao City Health - Case Investigation FormRobee Camille Desabelle-SumatraNo ratings yet
- CPHP HO Kathmandu 2080Document98 pagesCPHP HO Kathmandu 2080bibek karkiNo ratings yet
- Phenytoin: Phenytoin (PHT), Sold Under The Brand Name Dilantin AmongDocument13 pagesPhenytoin: Phenytoin (PHT), Sold Under The Brand Name Dilantin AmongMunna SahaniNo ratings yet
- Report 18 38Document22 pagesReport 18 38Abhisek PattnaikNo ratings yet
- Allergy MahmoudiDocument992 pagesAllergy MahmoudiDiana SNo ratings yet
- Occupational English Test Listening Test - 2Document6 pagesOccupational English Test Listening Test - 2Jojelyn Yanez BaliliNo ratings yet
- Inflammatory Disorders PDFDocument41 pagesInflammatory Disorders PDFMoon KillerNo ratings yet
- Hirac Installation Panel FPV SubstationDocument3 pagesHirac Installation Panel FPV SubstationekapadwiNo ratings yet
- Nasal Polyps Treatment Miracle - The Natural Nasal Polyps CureDocument23 pagesNasal Polyps Treatment Miracle - The Natural Nasal Polyps CureSpencer ClineNo ratings yet
- Training Module MerkchemDocument110 pagesTraining Module MerkchemArila Roberts100% (1)
- HA-Midterms LabDocument13 pagesHA-Midterms LabMa. Daniela De la CernaNo ratings yet
- I. General ObjectiveDocument4 pagesI. General ObjectiveKeon RicoNo ratings yet
- Cilia 2018Document1 pageCilia 2018Anna Beatriz Silva EspindolaNo ratings yet
- BADBREATHDocument23 pagesBADBREATHBilly TrầnNo ratings yet
- 24744Document149 pages24744John FaustorillaNo ratings yet