Download as pdf or txt
You might also like
- Statement From Head of School John McWilliamsDocument5 pagesStatement From Head of School John McWilliamsMontgomery AdvertiserNo ratings yet
- OSTEORADIONECROSISDocument38 pagesOSTEORADIONECROSISAbel AbrahamNo ratings yet
- Affidavit EnglishDocument3 pagesAffidavit EnglishPicococoNo ratings yet
- Tops Bankruptcy DocumentsDocument83 pagesTops Bankruptcy DocumentsAnonymous vhwDL2u100% (1)
- Project Report On RTS Juice PlantDocument7 pagesProject Report On RTS Juice PlantEIRI Board of Consultants and PublishersNo ratings yet
- Form 1 Science NotesDocument19 pagesForm 1 Science NotesQQLove93% (14)
- Pensatory Damages Fall 2014 Prof. George W. ConkFordham Law Schoolgconk@law - Fordham.eduDocument80 pagesPensatory Damages Fall 2014 Prof. George W. ConkFordham Law Schoolgconk@law - Fordham.eduGeorge ConkNo ratings yet
- A Clog On The Equity of RedemptDocument27 pagesA Clog On The Equity of Redemptamit dipankarNo ratings yet
- Affidavit Mortgagee Bank PDFDocument1 pageAffidavit Mortgagee Bank PDFRanie DelaventeNo ratings yet
- World Bitcoin Association LLCDocument7 pagesWorld Bitcoin Association LLCChapter 11 DocketsNo ratings yet
- Affidavit of No ComplaintDocument1 pageAffidavit of No ComplaintAdrian CabahugNo ratings yet
- Client Family Confidentiality and Non-Disclosure AgreementDocument2 pagesClient Family Confidentiality and Non-Disclosure AgreementJuan ArellanoNo ratings yet
- Instructions For Form 1066: U.S. Real Estate Mortgage Investment Conduit (REMIC) Income Tax ReturnDocument6 pagesInstructions For Form 1066: U.S. Real Estate Mortgage Investment Conduit (REMIC) Income Tax ReturnIRSNo ratings yet
- Fred and Wilma FlintstoneDocument3 pagesFred and Wilma Flintstoneapi-270699969No ratings yet
- Agencies Incorporated in DelawareDocument1 pageAgencies Incorporated in DelawareAkil BeyNo ratings yet
- Bonded Bill of Exchange TemplateDocument1 pageBonded Bill of Exchange Template94successfulNo ratings yet
- Suntrust Bank v. John H. Ruiz, 11th Cir. (2016)Document12 pagesSuntrust Bank v. John H. Ruiz, 11th Cir. (2016)Scribd Government DocsNo ratings yet
- Lady Bird Deed (1) (1) - 1Document5 pagesLady Bird Deed (1) (1) - 1Shane BougeNo ratings yet
- Tda066 PDFDocument13 pagesTda066 PDFjuanNo ratings yet
- Ejectment ActionDocument22 pagesEjectment ActionOxigyneNo ratings yet
- First National Bank of Emlenton, Pennsylvania v. United States, 265 F.2d 297, 1st Cir. (1959)Document4 pagesFirst National Bank of Emlenton, Pennsylvania v. United States, 265 F.2d 297, 1st Cir. (1959)Scribd Government DocsNo ratings yet
- Rescission IDocument60 pagesRescission Ierica.oreilly59No ratings yet
- "COMPANY NAME" Business Plan: (Tagline or Philosophy) Add A Photo or Personal Design (Optional)Document12 pages"COMPANY NAME" Business Plan: (Tagline or Philosophy) Add A Photo or Personal Design (Optional)moNo ratings yet
- Durable Power of Attorney DocumentDocument2 pagesDurable Power of Attorney DocumentQuincy Von Wildbeast100% (1)
- Petitioners: Appeals Most Respectfully StatesDocument3 pagesPetitioners: Appeals Most Respectfully StatesCyrill L. MarkNo ratings yet
- California Limited Special Power of Attorney FormDocument3 pagesCalifornia Limited Special Power of Attorney FormHager FaroukNo ratings yet
- CBV Collections Notice of Demand To Cease and Desist To All CreditorsDocument3 pagesCBV Collections Notice of Demand To Cease and Desist To All CreditorskrystalmarienymannNo ratings yet
- I Do Not Accept This Offer To Contract and I Do Not Consent To These ProceedingsDocument1 pageI Do Not Accept This Offer To Contract and I Do Not Consent To These ProceedingsNat WilliamsNo ratings yet
- Broke Brothers PetitionDocument22 pagesBroke Brothers PetitionZerohedgeNo ratings yet
- Hocus Pocus?: Converting Real Property Into Personal PropertyDocument14 pagesHocus Pocus?: Converting Real Property Into Personal PropertyLEBJ100% (1)
- ADS Chapter 625 Accounts Receivable and Debt CollectionDocument48 pagesADS Chapter 625 Accounts Receivable and Debt CollectionShabbir BukhariNo ratings yet
- 2-1-2021 Response To LandlordDocument2 pages2-1-2021 Response To LandlordJessica SwarnerNo ratings yet
- Stop The PiratesDocument4 pagesStop The Pirateskatia100% (1)
- Trust ReceiptDocument3 pagesTrust ReceiptMaFatimaP.LeeNo ratings yet
- Surety BondDocument3 pagesSurety BondRenz Dela Cruz100% (1)
- Fair Lending Notice PDFDocument2 pagesFair Lending Notice PDFJesse100% (1)
- UntitledDocument1 pageUntitledCarlosNo ratings yet
- Government Claim Filing Instructions: State of California - Department of General Services DGS ORIM 06 (Rev. 05/2017)Document5 pagesGovernment Claim Filing Instructions: State of California - Department of General Services DGS ORIM 06 (Rev. 05/2017)Gucci LouieNo ratings yet
- Contracts OutlineDocument25 pagesContracts OutlineErica LindsayNo ratings yet
- 3 Blank Notice of DefaultDocument3 pages3 Blank Notice of DefaultKristin Cantley SnellNo ratings yet
- Substitution of Attorney-Civil Non Conformed State Case ONLYDocument2 pagesSubstitution of Attorney-Civil Non Conformed State Case ONLYtmccand100% (1)
- Black Service Request FormDocument1 pageBlack Service Request FormAtikah Alia AqeelahNo ratings yet
- United States District CourtDocument36 pagesUnited States District CourtMike SiscoNo ratings yet
- Application For Drivers License RenewalDocument2 pagesApplication For Drivers License RenewalJames neteruNo ratings yet
- Gahler Opposition To FroshDocument27 pagesGahler Opposition To FroshRohan MNo ratings yet
- The General Relationship Between Bank and Its CustomerDocument9 pagesThe General Relationship Between Bank and Its CustomerAnkit AgarwalNo ratings yet
- Village of Goodfield Annexation ProcedureDocument2 pagesVillage of Goodfield Annexation ProcedureHelpin HandNo ratings yet
- Jannett Spence Lawsuit Against Eric Readon.Document47 pagesJannett Spence Lawsuit Against Eric Readon.Amanda RojasNo ratings yet
- Training Material ContractsDocument308 pagesTraining Material ContractsRachel SibandaNo ratings yet
- Breach of ContractDocument6 pagesBreach of Contractbharti35No ratings yet
- Law On Sales AssignmentDocument13 pagesLaw On Sales AssignmentGennia Mae MartinezNo ratings yet
- Department of Probation, Parole and Pardon Services: Henry Mcmaster Jerry B. AdgerDocument4 pagesDepartment of Probation, Parole and Pardon Services: Henry Mcmaster Jerry B. Adgerashish14321100% (1)
- Foreign Person's U.S. Source Income Subject To Withholding: Copy BDocument6 pagesForeign Person's U.S. Source Income Subject To Withholding: Copy BAshot KHACHATOURIAN100% (1)
- (D.E.1) Complaint NCUA V Bear Sterns & Co N/k/a JPMorgan Chase Securities 13-cv-06707 (S.D.N.Y.)Document155 pages(D.E.1) Complaint NCUA V Bear Sterns & Co N/k/a JPMorgan Chase Securities 13-cv-06707 (S.D.N.Y.)larry-612445No ratings yet
- Bill of ParticularsDocument2 pagesBill of ParticularsMeng GoblasNo ratings yet
- Florida Rules of Appellate Procedure ...Document170 pagesFlorida Rules of Appellate Procedure ...Judicial_FraudNo ratings yet
- ICCForm Reparation 2 enDocument14 pagesICCForm Reparation 2 enEmpressInINo ratings yet
- BFRReportImage AspxDocument2 pagesBFRReportImage Aspxscottk929No ratings yet
- Help To Pay RentDocument2 pagesHelp To Pay RenttscottbuysNo ratings yet
- You Are My Servant and I Have Chosen You: What It Means to Be Called, Chosen, Prepared and Ordained by God for MinistryFrom EverandYou Are My Servant and I Have Chosen You: What It Means to Be Called, Chosen, Prepared and Ordained by God for MinistryNo ratings yet
- Student Handbook AcknowledgementDocument1 pageStudent Handbook AcknowledgementKevin CardosoNo ratings yet
- Photo PermissionDocument1 pagePhoto PermissionKevin CardosoNo ratings yet
- Social Security Verification FormDocument1 pageSocial Security Verification FormKevin CardosoNo ratings yet
- Parent Permission Form - Field Trip: Miami-Dade County Public SchoolsDocument1 pageParent Permission Form - Field Trip: Miami-Dade County Public SchoolsKevin CardosoNo ratings yet
- Emergency Student Data FormDocument1 pageEmergency Student Data FormKevin CardosoNo ratings yet
- Summer School Registration FormDocument1 pageSummer School Registration FormKevin CardosoNo ratings yet
- Walking AidsDocument2 pagesWalking AidsSofia P. PanlilioNo ratings yet
- DR Physique Lean Bulking Series II 2015Document121 pagesDR Physique Lean Bulking Series II 2015Vlad Alexandru50% (2)
- 1.1 - Monitor de Aterramento - 8030Document2 pages1.1 - Monitor de Aterramento - 8030Denis MarcosNo ratings yet
- MCN KweenDocument4 pagesMCN KweenAngelo SigueNo ratings yet
- Safeway SWOT AnalysisDocument9 pagesSafeway SWOT AnalysisAlbertWhatmoughNo ratings yet
- Materials Chemistry A: Journal ofDocument7 pagesMaterials Chemistry A: Journal ofFamiloni LayoNo ratings yet
- Statement of Account: State Bank of IndiaDocument1 pageStatement of Account: State Bank of Indiavishalasharma0% (1)
- Product Manual 26361V1 (Revision F) : 505DE Digital Governor For Steam TurbinesDocument198 pagesProduct Manual 26361V1 (Revision F) : 505DE Digital Governor For Steam TurbinesGuilherme Marquezin100% (1)
- OlanzapineDocument1 pageOlanzapineKallie ChartrandNo ratings yet
- Case Study Booklet 2 PDFDocument43 pagesCase Study Booklet 2 PDFguddu yadavNo ratings yet
- OSH SeminarDocument2 pagesOSH SeminarSahar Ulu JeruasNo ratings yet
- Food and Nutrition Multiple Choice Questions With AnswersDocument6 pagesFood and Nutrition Multiple Choice Questions With AnswersMark Busalpa40% (5)
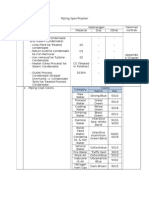
- Piping SpecificationDocument5 pagesPiping SpecificationShandi Hasnul FarizalNo ratings yet
- Lock Out Tag Out: Review QuestionsDocument37 pagesLock Out Tag Out: Review QuestionsMansoor AliNo ratings yet
- SRHR - FGD With Young PeopleDocument3 pagesSRHR - FGD With Young PeopleMandira PrakashNo ratings yet
- Chicken BellagioDocument4 pagesChicken BellagioJagr MaddoxNo ratings yet
- Bio OhDocument3 pagesBio OhEmmaNo ratings yet
- Dan Sof TG 0122Document30 pagesDan Sof TG 0122Erick Trujillo100% (1)
- Barcode v1Document31 pagesBarcode v1Desinta OctavianiNo ratings yet
- Module 7: Health Care Delivery SystemDocument9 pagesModule 7: Health Care Delivery SystemDanz KieNo ratings yet
- Is Your Body Infested With Self-Replicating Nano-FibersDocument4 pagesIs Your Body Infested With Self-Replicating Nano-Fibersthisdraft100% (3)
- Starkville Dispatch Eedition 7-29-20Document16 pagesStarkville Dispatch Eedition 7-29-20The DispatchNo ratings yet
- Surface Anatomy Lungs Group 2bDocument8 pagesSurface Anatomy Lungs Group 2bapi-323356666No ratings yet
- MASB7 Construction Contract7Document3 pagesMASB7 Construction Contract7hyraldNo ratings yet
- Why Aws Is Even Better With CloudcheckrDocument7 pagesWhy Aws Is Even Better With CloudcheckrPardha SaradhiNo ratings yet
- Economics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Document8 pagesEconomics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Yvette LimNo ratings yet