Download as pdf or txt
You might also like
- Bone and Soft Tissue SarcomaDocument67 pagesBone and Soft Tissue SarcomaSalmanArifNo ratings yet
- Publishers Business Plan & Strategic Plan ELEVATE ConsultancyDocument70 pagesPublishers Business Plan & Strategic Plan ELEVATE ConsultancyTumim67% (3)
- Orion 10.6 - Getting StartedDocument25 pagesOrion 10.6 - Getting StartedM Jacksmerv SamuelNo ratings yet
- Classic D&D Races For D&D 5th EditionDocument7 pagesClassic D&D Races For D&D 5th EditionRyan Lowder100% (11)
- Template CT Scan (Amirul)Document5 pagesTemplate CT Scan (Amirul)Amirul MukminNo ratings yet
- 2012 VIN Kirberger CTDocument5 pages2012 VIN Kirberger CTNoSpamNo ratings yet
- Introduction To RadiologyDocument33 pagesIntroduction To Radiologyمركز ريلاكس للعلاج الطبيعيNo ratings yet
- MaxFac RadiologyDocument172 pagesMaxFac RadiologyDr. Debbie SabladaNo ratings yet
- Aneurisma IntracranealDocument13 pagesAneurisma IntracranealEdgar CorbiéreNo ratings yet
- NCM118 TransesDocument11 pagesNCM118 TransesAlejandro Saclolo, IIINo ratings yet
- AJR Teaching File: Intraventricular Mass: Clinical HistoryDocument4 pagesAJR Teaching File: Intraventricular Mass: Clinical HistoryDokdem AjaNo ratings yet
- Poster Case Report Revisi 1Document1 pagePoster Case Report Revisi 1Lalu Rizky AdipuraNo ratings yet
- 2.1 CD 2B Radio Introduction To Musculoskeletal Joints and Axial Spine Md2020Document9 pages2.1 CD 2B Radio Introduction To Musculoskeletal Joints and Axial Spine Md2020Eduardo Marco Villarama DayritNo ratings yet
- Large Cerebral Arachnoid CystDocument2 pagesLarge Cerebral Arachnoid CystAtiquzzaman RinkuNo ratings yet
- Nagar Et Al 2012 Reperfusion Phenomenon Masking Acute and Subacute Infarcts at Dynamic Perfusion CT Confirmation byDocument10 pagesNagar Et Al 2012 Reperfusion Phenomenon Masking Acute and Subacute Infarcts at Dynamic Perfusion CT Confirmation byAnonymous Bu43ZUNo ratings yet
- 2-3 BRAIN 4th YearDocument71 pages2-3 BRAIN 4th YearYosra —No ratings yet
- 6 Head and Neck Trauma - Thoracic and Cardiovascular TraumaDocument7 pages6 Head and Neck Trauma - Thoracic and Cardiovascular TraumaMyrtle Yvonne RagubNo ratings yet
- Imaging of Spine Trauma: Neuroradiology Review Series Neuroradiology Review SeriesDocument17 pagesImaging of Spine Trauma: Neuroradiology Review Series Neuroradiology Review SeriesSalman Alfarisy GaulNo ratings yet
- Spinal Cord Herniation Why Anterior ThoracicDocument5 pagesSpinal Cord Herniation Why Anterior ThoracicShahid KhanNo ratings yet
- Neurosurgery ReportingDocument63 pagesNeurosurgery ReportingMa. Jessa Victoria VallangcaNo ratings yet
- 4 BQ0053-A Clinical Consideration For Spine Procedures EU PDFDocument7 pages4 BQ0053-A Clinical Consideration For Spine Procedures EU PDFGame BelanjaNo ratings yet
- Brain Tumor - IntraExtra AxialDocument6 pagesBrain Tumor - IntraExtra AxialregarskidNo ratings yet
- Differentiation of True Anophthalmia From Clinical Anophthalmia Using Neuroradiological ImagingDocument6 pagesDifferentiation of True Anophthalmia From Clinical Anophthalmia Using Neuroradiological ImagingMarisol DíazNo ratings yet
- Mri BrainDocument74 pagesMri Brainagithia100% (1)
- Cabeza y Cuello PDFDocument24 pagesCabeza y Cuello PDFDavid ReyesNo ratings yet
- MRI Brain - Neurologist P Ed.VDocument58 pagesMRI Brain - Neurologist P Ed.Vnila choNo ratings yet
- Algorithm of C Spine Injuries (Langkawi)Document71 pagesAlgorithm of C Spine Injuries (Langkawi)PopyNo ratings yet
- Iris and Ciliary Body Tumors: Surgery VersusDocument4 pagesIris and Ciliary Body Tumors: Surgery VersusAnonymous syRbQm6No ratings yet
- Herniation of Uncus and Parahippocampal Gyrus: An Accidental Finding On Magnetic Resonance Imaging of CerebrumDocument3 pagesHerniation of Uncus and Parahippocampal Gyrus: An Accidental Finding On Magnetic Resonance Imaging of CerebrumDanaAmaranducaiNo ratings yet
- Approach To MRI Management in Stroke - PARI Kota MakassarDocument50 pagesApproach To MRI Management in Stroke - PARI Kota MakassarASMARNo ratings yet
- 01 Redalyc Martinez RizoDocument14 pages01 Redalyc Martinez RizoStefanie Valeria Espinoza TorrakaNo ratings yet
- Neuro Exam and Localization For The InternistDocument6 pagesNeuro Exam and Localization For The InternistOleOhhNo ratings yet
- Neurosonography in The Neonate FinalDocument9 pagesNeurosonography in The Neonate FinalCh RajeshNo ratings yet
- Radiology Imaging in Cochlear Implant Preparation PDFDocument50 pagesRadiology Imaging in Cochlear Implant Preparation PDFrizaNo ratings yet
- Spinal Cord TumorsDocument7 pagesSpinal Cord TumorsVALERIA TEJEDA SANCHEZNo ratings yet
- p2863 PDFDocument8 pagesp2863 PDFAnonymous jXRSb1No ratings yet
- Disadvantages of CT Advantages of MRI: Definitions of Neurologic FindingsDocument4 pagesDisadvantages of CT Advantages of MRI: Definitions of Neurologic FindingsAfif Al BaalbakiNo ratings yet
- Symmetry: Symmetry of The Brain Is The Key To RadiologicDocument7 pagesSymmetry: Symmetry of The Brain Is The Key To RadiologicVon HippoNo ratings yet
- Radio - MusculoskeletalDocument20 pagesRadio - MusculoskeletalVon HippoNo ratings yet
- A Rare Case of Optic Nerve Schwannoma: Case Report and Review of The LiteratureDocument5 pagesA Rare Case of Optic Nerve Schwannoma: Case Report and Review of The LiteratureloversockfulNo ratings yet
- Estimating The Position of The MiddleDocument1 pageEstimating The Position of The MiddleWIL CaseresNo ratings yet
- 2 2CDPDHeadacheVISIONDocument7 pages2 2CDPDHeadacheVISIONEduardo Marco Villarama DayritNo ratings yet
- GLOSSARY The Optic Nerve Head in GlaucomaDocument2 pagesGLOSSARY The Optic Nerve Head in GlaucomaChristine Yohana SianturiNo ratings yet
- Chapter 2 Introduction To Brain ImagingDocument3 pagesChapter 2 Introduction To Brain Imagingsybico.xray.abadclinicNo ratings yet
- Sella Turcica and Parasellar RegionDocument19 pagesSella Turcica and Parasellar RegionabdelmaksodNo ratings yet
- Brain TumorDocument1 pageBrain TumorChase XerolfNo ratings yet
- Imaging of Orbita and Ear FKDocument70 pagesImaging of Orbita and Ear FKAprilia Anggela100% (1)
- Bloqueos Miembro SuperiorDocument1 pageBloqueos Miembro SuperiorpimpollopittNo ratings yet
- Cranialnerveassessmentfinal 140501113414 Phpapp01 PDFDocument42 pagesCranialnerveassessmentfinal 140501113414 Phpapp01 PDFAlma Baterina100% (1)
- Cranial Nerve AssessmentDocument42 pagesCranial Nerve Assessmentmalik003100% (1)
- Basic Neuroimaging (CT and MRI)Document56 pagesBasic Neuroimaging (CT and MRI)Dave Cronin100% (3)
- Subspec Urology: GU TumorsDocument5 pagesSubspec Urology: GU TumorsThakoon TtsNo ratings yet
- Nervous System Path (MSN) PDFDocument150 pagesNervous System Path (MSN) PDFRodrigoMendozaNo ratings yet
- Interpretation B WDocument13 pagesInterpretation B Wmulya sfNo ratings yet
- Radiopaedia 2020 Virtual Conference June 22-25Document3 pagesRadiopaedia 2020 Virtual Conference June 22-25Prem Kumar BNo ratings yet
- 5 Paranasal Sinus VariantsDocument6 pages5 Paranasal Sinus VariantsMatheusDorigattiSoldatelliNo ratings yet
- Insignis Surgery NeurosurgeryDocument15 pagesInsignis Surgery NeurosurgeryAla'a Emerald AguamNo ratings yet
- CT Scan Head N BrainDocument45 pagesCT Scan Head N Brainaria tristayanthiNo ratings yet
- Mature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportDocument5 pagesMature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportHaribabuBabuNo ratings yet
- Frontal Sinus FracturesDocument15 pagesFrontal Sinus FracturesCatarine OttobeliNo ratings yet
- CT vs. Mri Compendium 2011 1 PDFDocument4 pagesCT vs. Mri Compendium 2011 1 PDFWaqas HaleemNo ratings yet
- Pathway For Management of Cerebral SOL V3 March 2018Document1 pagePathway For Management of Cerebral SOL V3 March 2018Muhammad NazrilNo ratings yet
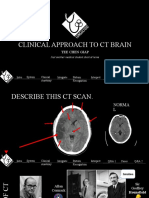
- Clinical Approach To CT BrainDocument34 pagesClinical Approach To CT BrainXiaoThoong LohNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoNo ratings yet
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocument7 pagesDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (2)
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoNo ratings yet
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoNo ratings yet
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoNo ratings yet
- Child PsychiatryDocument6 pagesChild PsychiatryVon HippoNo ratings yet
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoNo ratings yet
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoNo ratings yet
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoNo ratings yet
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoNo ratings yet
- 1) Any Medical Student or GraduateDocument27 pages1) Any Medical Student or GraduateVon HippoNo ratings yet
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- Abdominal: Al HerniaDocument3 pagesAbdominal: Al HerniaVon Hippo100% (1)
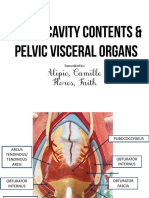
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoNo ratings yet
- Fluid and Electrolytes YMDocument8 pagesFluid and Electrolytes YMVon HippoNo ratings yet
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoNo ratings yet
- Book: - RecordingDocument8 pagesBook: - RecordingVon HippoNo ratings yet
- Compilation of Platings in MicrobiologyDocument6 pagesCompilation of Platings in MicrobiologyVon HippoNo ratings yet
- NEPHRO - Renal Stones PDFDocument3 pagesNEPHRO - Renal Stones PDFVon HippoNo ratings yet
- Internal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoDocument3 pagesInternal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoVon HippoNo ratings yet
- Biochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Document14 pagesBiochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Von HippoNo ratings yet
- 2013 Compiled para Exams and Shiftings PDFDocument27 pages2013 Compiled para Exams and Shiftings PDFVon HippoNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- Employee Data (Application) FormDocument2 pagesEmployee Data (Application) FormGlaneisia MitchellNo ratings yet
- Can You Lose Your Salvation - Hebrews 6Document5 pagesCan You Lose Your Salvation - Hebrews 6Sanjay SarkarNo ratings yet
- Pathophysiology of Patent Ductus Arteroisus (PDA)Document2 pagesPathophysiology of Patent Ductus Arteroisus (PDA)Rodel Yacas100% (1)
- Bucton Vs GabarDocument4 pagesBucton Vs GabarJustineNo ratings yet
- People v. CervantesDocument7 pagesPeople v. CervantesRodney AtibulaNo ratings yet
- AdvocacyDocument1 pageAdvocacyJustin DugangNo ratings yet
- Sacrament of Holy OrdersDocument20 pagesSacrament of Holy OrdersMatthew CortezNo ratings yet
- Children's Human Rights - An Interdisciplinary IntroductionDocument18 pagesChildren's Human Rights - An Interdisciplinary IntroductionKaren Álvarez VargasNo ratings yet
- ChallengesDocument2 pagesChallengesChinmae XanthineNo ratings yet
- Kazmarski-Mus149-Assignment 4Document5 pagesKazmarski-Mus149-Assignment 4api-510873791No ratings yet
- United States v. Aaron Headspeth, 852 F.2d 753, 4th Cir. (1988)Document9 pagesUnited States v. Aaron Headspeth, 852 F.2d 753, 4th Cir. (1988)Scribd Government DocsNo ratings yet
- Legend Situ BagenditDocument6 pagesLegend Situ BagenditFaika NabilaNo ratings yet
- Parts of The 1987 ConstitutionDocument6 pagesParts of The 1987 ConstitutionDESA GALE MARASIGANNo ratings yet
- Magdalo para Sa Pagbabago V ComelecDocument2 pagesMagdalo para Sa Pagbabago V ComelecCamille TapecNo ratings yet
- 2020 Immediate Care of The Newborn 3Document56 pages2020 Immediate Care of The Newborn 3Ellah PerenioNo ratings yet
- Methods of Statistical SurveyDocument2 pagesMethods of Statistical Surveyshailesh67% (3)
- Final Survey QuestionnaireDocument2 pagesFinal Survey QuestionnaireMichael AquinoNo ratings yet
- Bio MoleculesDocument27 pagesBio MoleculesMr XNo ratings yet
- English Grammar Test With AnswersDocument39 pagesEnglish Grammar Test With Answersmehari kirosNo ratings yet
- Susantha CV - NewDocument4 pagesSusantha CV - NewsusanthaNo ratings yet
- S2 May 2012 Part1Document7 pagesS2 May 2012 Part1Wahid Salauddin DiptaNo ratings yet
- Introduction To Metric SpacesDocument15 pagesIntroduction To Metric Spaceshyd arnes100% (1)
- Impacts of Imports, Exports and Foreign Direct Investment On The Gross Domestic Product (GDP) GrowthDocument2 pagesImpacts of Imports, Exports and Foreign Direct Investment On The Gross Domestic Product (GDP) Growthzee3000No ratings yet
- Baptist Today Sept 13Document4 pagesBaptist Today Sept 13hlimaralteNo ratings yet
- NovelApproachToAITrading Using GenotickDocument40 pagesNovelApproachToAITrading Using GenotickSenthil KumarNo ratings yet
- Lesson Plan For Hindu Ideals and Idols For Students - A Textbook For Introducing Hindu Values (Vishal Agarwal, 2012)Document5 pagesLesson Plan For Hindu Ideals and Idols For Students - A Textbook For Introducing Hindu Values (Vishal Agarwal, 2012)kalyan974696No ratings yet