Download as pdf or txt
You might also like
- Control of Microbial GrowthDocument21 pagesControl of Microbial GrowthLeeShauran100% (7)
- Phenyl MakingDocument4 pagesPhenyl MakingVikram Ullal100% (6)
- United States Air Force Afva 32-4022 - 1 April 1999Document1 pageUnited States Air Force Afva 32-4022 - 1 April 1999marshall, of courseNo ratings yet
- FM 3-4 Nuclear and Biological Contamination ProtectionDocument123 pagesFM 3-4 Nuclear and Biological Contamination ProtectionAndrew WilliamsNo ratings yet
- Fuel Air (Thermobaric) Weapons PDFDocument2 pagesFuel Air (Thermobaric) Weapons PDFsorinartistuNo ratings yet
- Bomb Threat ManuscriptDocument2 pagesBomb Threat ManuscriptAl-ajim HadjiliNo ratings yet
- WIRTZ, James J. Weapons of Mass DestructionDocument17 pagesWIRTZ, James J. Weapons of Mass DestructionMarta RochaNo ratings yet
- VMR3 LeafletDocument7 pagesVMR3 LeafletAnton KsendzNo ratings yet
- Revision - Revision - Eyewear CatalogDocument15 pagesRevision - Revision - Eyewear CatalogЖеня АлександровNo ratings yet
- 093-401-5040 React To Unexploded Ordnance HazardsDocument11 pages093-401-5040 React To Unexploded Ordnance HazardsMarcus BranhamNo ratings yet
- Stanag A231Document54 pagesStanag A231Ahmet ÖztemürNo ratings yet
- CBRN Glossary: HOME-CBRN-AG@ec - Europa.euDocument51 pagesCBRN Glossary: HOME-CBRN-AG@ec - Europa.eublue4nightNo ratings yet
- Trijicon: Features and BenefitsDocument7 pagesTrijicon: Features and Benefitsjorge celyNo ratings yet
- Eurados Report 201202Document194 pagesEurados Report 201202Laurentiu RadoiNo ratings yet
- TN 09.30 04 2001 FAE V.10 Amd 1 01Document20 pagesTN 09.30 04 2001 FAE V.10 Amd 1 01KhaledMadridi100% (1)
- Rocket SteelDocument48 pagesRocket Steelsmith willNo ratings yet
- A Review of Recent Evidence For UtilizingDocument5 pagesA Review of Recent Evidence For Utilizingsseagal_2No ratings yet
- Patel 2007Document6 pagesPatel 2007bw2801381No ratings yet
- Ijerph 16 03572Document10 pagesIjerph 16 03572Cassie AbernathNo ratings yet
- HVAC Systems For Environmental Control To Minimize The COVID-19 InfectionDocument7 pagesHVAC Systems For Environmental Control To Minimize The COVID-19 Infectiongrady janitraNo ratings yet
- Biological Monitoring: Lichens As Bioindicators of Air Pollution Assessment Ð A ReviewDocument22 pagesBiological Monitoring: Lichens As Bioindicators of Air Pollution Assessment Ð A ReviewXuân Hoàng ĐinhNo ratings yet
- v2 Guide Points - Gad and Environment - June 23Document32 pagesv2 Guide Points - Gad and Environment - June 23ajrevillaNo ratings yet
- HVAC Systems For Environmental Control To Minimize The COVID-19 InfectionDocument7 pagesHVAC Systems For Environmental Control To Minimize The COVID-19 InfectionRAMESH KRISHNAN LNo ratings yet
- Autonomous Disinfection System (Unfinish)Document7 pagesAutonomous Disinfection System (Unfinish)IvanAlabaNo ratings yet
- Biological Monitoring: Lichens As Bioindicators of Air Pollution Assessment - A ReviewDocument23 pagesBiological Monitoring: Lichens As Bioindicators of Air Pollution Assessment - A ReviewTri MardianiNo ratings yet
- European Infectious Disease: Volume 6 - Issue 2 - Winter 2012 - ExtractDocument7 pagesEuropean Infectious Disease: Volume 6 - Issue 2 - Winter 2012 - Extractkasu s reddyNo ratings yet
- Ecotoxicology and Environmental Safety: Aline D. Gonçalves, Tayene G. Martins, Ricardo J. CassellaDocument6 pagesEcotoxicology and Environmental Safety: Aline D. Gonçalves, Tayene G. Martins, Ricardo J. CassellaYoselin GomezNo ratings yet
- Correlation of Antibacterial Performance To Electrostatic 2022 Journal of ElDocument7 pagesCorrelation of Antibacterial Performance To Electrostatic 2022 Journal of ElNilesh NarkhedeNo ratings yet
- Environmental Hygiene - The Importance of Process, Product and Practice PDFDocument18 pagesEnvironmental Hygiene - The Importance of Process, Product and Practice PDFAnsh KunalNo ratings yet
- Scientific Paper On Air Pollution Detection by Use of Digital ImagesDocument4 pagesScientific Paper On Air Pollution Detection by Use of Digital ImagesIsaac KimaruNo ratings yet
- UVGI Design Basics PDFDocument10 pagesUVGI Design Basics PDFMeduNo ratings yet
- Ezzati Kammen 2001 Quantifying The Effects of Exposure To Indoor Air Pollution From Biomass CombustDocument8 pagesEzzati Kammen 2001 Quantifying The Effects of Exposure To Indoor Air Pollution From Biomass CombustsabriNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Atmospheric Environment: XDocument11 pagesAtmospheric Environment: XIon CorbuNo ratings yet
- Methods To Quantify Particle Air Pollution Removal by Urban VegetationDocument25 pagesMethods To Quantify Particle Air Pollution Removal by Urban VegetationferdzacNo ratings yet
- 1 s2.0 S0160412022001994 MainDocument10 pages1 s2.0 S0160412022001994 MainEduardo FernandezNo ratings yet
- 20231122AI02 - Antimicrobial Treatment Effect On FiberglassDocument7 pages20231122AI02 - Antimicrobial Treatment Effect On FiberglassMlx HoNo ratings yet
- UntitledDocument25 pagesUntitledomar ahmedNo ratings yet
- EnE 317Document13 pagesEnE 317Lianne PeñalosaNo ratings yet
- Effectiveness of Manual Terminal Cleaning Varies On High To - 2022 - ArthroplastDocument5 pagesEffectiveness of Manual Terminal Cleaning Varies On High To - 2022 - ArthroplastSanty OktavianiNo ratings yet
- Airborne Particle Monitoring in Clean Room Environments For Stem Cell CulturesDocument10 pagesAirborne Particle Monitoring in Clean Room Environments For Stem Cell Culturesrobson.brunoNo ratings yet
- 2021 - Article - 9693 ThesisDocument19 pages2021 - Article - 9693 ThesisNew Certificate001No ratings yet
- Saravanan 2021Document6 pagesSaravanan 2021VenkatNo ratings yet
- Medical Waste Management and Design of a Low-Cost Incinerator for ReductionDocument10 pagesMedical Waste Management and Design of a Low-Cost Incinerator for ReductionazidcmeNo ratings yet
- Ajehe 9 124Document6 pagesAjehe 9 124hendri sutrisnoNo ratings yet
- Missirlis, Katsikogianni, Missirlis. 2004. CONCISE REVIEW OF MECHANISMS OF BACTERIAL ADHESION TO BIOMATERIALS AND OF TECHNIQUES USED INDocument21 pagesMissirlis, Katsikogianni, Missirlis. 2004. CONCISE REVIEW OF MECHANISMS OF BACTERIAL ADHESION TO BIOMATERIALS AND OF TECHNIQUES USED INAzb 711No ratings yet
- IJPEST Vol10 No1 03 pp011-015Document5 pagesIJPEST Vol10 No1 03 pp011-015NandisetaNo ratings yet
- Recomendaciones Aep Sobre Alimentacio N Complementaria Nov2018 v3 FinalDocument6 pagesRecomendaciones Aep Sobre Alimentacio N Complementaria Nov2018 v3 FinalMatìas GamarraNo ratings yet
- The Making of A Contactless Sanitation System Out of Arduino Interface and Ion GeneratorsDocument6 pagesThe Making of A Contactless Sanitation System Out of Arduino Interface and Ion GeneratorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration-Control Pekan Ke 2Document11 pagesIntegration-Control Pekan Ke 2RahmaNo ratings yet
- Referencia 9. (2008) PDFDocument52 pagesReferencia 9. (2008) PDFF. SALVADOR SANDOVALNo ratings yet
- Othman Et Al.,2014 PDFDocument8 pagesOthman Et Al.,2014 PDFIzzSyie ViruszNo ratings yet
- IMRAD UltrasonicDocument4 pagesIMRAD UltrasonicJan Jericho MentoyNo ratings yet
- Photocatalysis of B-Blockers - An Overview: Arabian Journal of ChemistryDocument8 pagesPhotocatalysis of B-Blockers - An Overview: Arabian Journal of Chemistrypetru apopeiNo ratings yet
- Metabolism Based Ventilation Monitoring and Control Meth - 2022 - Sustainable CiDocument11 pagesMetabolism Based Ventilation Monitoring and Control Meth - 2022 - Sustainable CiDaniel WismanNo ratings yet
- 2022 in Vitro Effect of Different Implant Decontamination Methods in Three Intraosseous Defect ConfigurationsDocument11 pages2022 in Vitro Effect of Different Implant Decontamination Methods in Three Intraosseous Defect Configurationsmatias cofreNo ratings yet
- How Do Biofilms Affect Surface Cleaning-2Document4 pagesHow Do Biofilms Affect Surface Cleaning-2dyatlovvadim65No ratings yet
- Particle Control Reduces Fine and Ultrafine Particles Greater Than HEPADocument4 pagesParticle Control Reduces Fine and Ultrafine Particles Greater Than HEPAzubairiNo ratings yet
- Desain Ruang DekontaminasiDocument8 pagesDesain Ruang Dekontaminasiisni maftuhahNo ratings yet
- Desain Ruang DekontaminasiDocument8 pagesDesain Ruang Dekontaminasiisni maftuhahNo ratings yet
- Effect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFDocument17 pagesEffect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFValerika GurschiNo ratings yet
- Estudio de Limpieza de Superficie en InglesDocument2 pagesEstudio de Limpieza de Superficie en Inglesstefanymoreno22No ratings yet
- Journal Pre-Proof: Microbes and InfectionDocument23 pagesJournal Pre-Proof: Microbes and InfectionDavid Adolfo Paez MolinaNo ratings yet
- Microbes and Infection: Xingchen Pan, David M. Ojcius, Tianyue Gao, Zhongsheng Li, Chunhua Pan, Chungen PanDocument6 pagesMicrobes and Infection: Xingchen Pan, David M. Ojcius, Tianyue Gao, Zhongsheng Li, Chunhua Pan, Chungen PanDavid Adolfo Paez MolinaNo ratings yet
- Evaluation of An Automatic Fogging Disinfection UnitDocument5 pagesEvaluation of An Automatic Fogging Disinfection UnitDavid Adolfo Paez MolinaNo ratings yet
- Applications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDocument12 pagesApplications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDavid Adolfo Paez MolinaNo ratings yet
- 12 PDFDocument3 pages12 PDFDavid Adolfo Paez MolinaNo ratings yet
- 1 PDFDocument7 pages1 PDFDavid Adolfo Paez MolinaNo ratings yet
- Additive Manufacturing Technologies For Biomedical Engineering Applications: Research Trends and Scientific ImpactDocument22 pagesAdditive Manufacturing Technologies For Biomedical Engineering Applications: Research Trends and Scientific ImpactDavid Adolfo Paez MolinaNo ratings yet
- Correspondence: Alcohol Use and Misuse During The COVID-19 Pandemic: A Potential Public Health Crisis?Document1 pageCorrespondence: Alcohol Use and Misuse During The COVID-19 Pandemic: A Potential Public Health Crisis?David Adolfo Paez MolinaNo ratings yet
- Industry 4.0 and Digital Manufacturing: A Design Method Applying Reverse EngineeringDocument23 pagesIndustry 4.0 and Digital Manufacturing: A Design Method Applying Reverse EngineeringDavid Adolfo Paez MolinaNo ratings yet
- NANOGOTADocument9 pagesNANOGOTADavid Adolfo Paez MolinaNo ratings yet
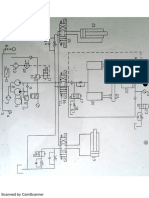
- Plano ElectroleohidráulicoDocument1 pagePlano ElectroleohidráulicoDavid Adolfo Paez MolinaNo ratings yet
- Rhinomanometer NR6: User ManualDocument24 pagesRhinomanometer NR6: User ManualAlonso ConchaNo ratings yet
- Acr On Modular Learning SimulationDocument4 pagesAcr On Modular Learning SimulationAbba JoyNo ratings yet
- CHEMDocument13 pagesCHEMAhmed AbdulmajeedNo ratings yet
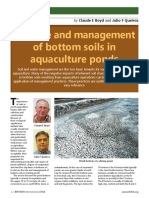
- The Role and Management of Bottom Soils in Aquaculture PondsDocument6 pagesThe Role and Management of Bottom Soils in Aquaculture Pondsristiawan nugrohoNo ratings yet
- Microplasma OzonatorDocument16 pagesMicroplasma Ozonatoranurag jhaNo ratings yet
- The Effect of Cyanuric Acid On The Disinfection Rate of Cryptosporidium Parvum in 20-ppm Free ChlorineDocument7 pagesThe Effect of Cyanuric Acid On The Disinfection Rate of Cryptosporidium Parvum in 20-ppm Free ChlorinePriya Vijay kumaarNo ratings yet
- Tle9 He Beauty Care Nail Care q1 Module 6 Wilnelia P. BigayDocument12 pagesTle9 He Beauty Care Nail Care q1 Module 6 Wilnelia P. BigayElaeca AbenNo ratings yet
- #4 - 2ND Day NPS03 Microparas Lec Finals ReviewerDocument74 pages#4 - 2ND Day NPS03 Microparas Lec Finals ReviewerYzobel Phoebe ParoanNo ratings yet
- Product ListDocument9 pagesProduct ListSudhir TripathiNo ratings yet
- Commercial Cooking: What Is This Module About?Document56 pagesCommercial Cooking: What Is This Module About?Sophie De VillaNo ratings yet
- Areas of Responsibilty of Housekeeping Department:: Housekeeping Refers To The Management of Duties and Chores InvolvedDocument13 pagesAreas of Responsibilty of Housekeeping Department:: Housekeeping Refers To The Management of Duties and Chores InvolvedKarissa Joy AgkisNo ratings yet
- Manual of Laboratory Animals Basic Facilities, Handling and CareDocument24 pagesManual of Laboratory Animals Basic Facilities, Handling and CareHajrah SuhardiNo ratings yet
- Microbial Resistance To DisinfectantsDocument7 pagesMicrobial Resistance To DisinfectantssyarifuddinNo ratings yet
- PHD Skibinski 20180219 Clean PdfaDocument187 pagesPHD Skibinski 20180219 Clean PdfaHersh F. HawramyNo ratings yet
- Postharvest Disease of TomatoDocument15 pagesPostharvest Disease of TomatomissyuezNo ratings yet
- A Level Biology A Core Practical 15 - Effects of AntibioticsDocument5 pagesA Level Biology A Core Practical 15 - Effects of AntibioticsAlfred SangNo ratings yet
- Food Safety PDFDocument11 pagesFood Safety PDFMaria AnnieskaNo ratings yet
- Materials Compatibility List: Chemicals For Processing Endoscopes and Endoscopic InstrumentsDocument24 pagesMaterials Compatibility List: Chemicals For Processing Endoscopes and Endoscopic InstrumentsarimudaNo ratings yet
- Nadca White Paper On Chemical Applications in Hvac Systems 0Document11 pagesNadca White Paper On Chemical Applications in Hvac Systems 0Luis RodasNo ratings yet
- Handfoot Spa Machine Tools Supplies and Equipment Steps in Giving Hand Foot Spa Pre Hand Spa Tratment Hand Spa TreatmentDocument6 pagesHandfoot Spa Machine Tools Supplies and Equipment Steps in Giving Hand Foot Spa Pre Hand Spa Tratment Hand Spa TreatmentCris Cali EspeNo ratings yet
- Alcohol Hand SanitizerDocument5 pagesAlcohol Hand SanitizerJohn SnowNo ratings yet
- How To Clean Effectively: A Cleaning Guide For Food Business Operators, Owners and Managers of Food BusinessesDocument24 pagesHow To Clean Effectively: A Cleaning Guide For Food Business Operators, Owners and Managers of Food Businesseshiba JamalNo ratings yet
- Masimo Emma Capnograph ManualDocument66 pagesMasimo Emma Capnograph ManualJef RobboNo ratings yet
- Commercial Dog Breeders Housing Part 2 SlidesDocument68 pagesCommercial Dog Breeders Housing Part 2 Slidesraj kiranNo ratings yet
- Post Hand Spa ActivityDocument16 pagesPost Hand Spa Activityma cleah ramosNo ratings yet
- T.L.E 7 4QDocument61 pagesT.L.E 7 4QyaelNo ratings yet
- SC160Document8 pagesSC160Ebenezer EffisahNo ratings yet
- Chemical Feed & DisinfectionDocument30 pagesChemical Feed & DisinfectionJohn MiklaNo ratings yet