Download as docx, pdf, or txt
You might also like
- 8.4 HW PropertiesRectRhomSquPracticeDocument2 pages8.4 HW PropertiesRectRhomSquPracticeERVIN DANCANo ratings yet
- Nursing Care Plan Diabetes Mellitus Type 2Document2 pagesNursing Care Plan Diabetes Mellitus Type 2deric88% (76)
- Nursing Care Plan San LuisDocument11 pagesNursing Care Plan San LuisRyan MirandaNo ratings yet
- Objective: Short Term Objectives: Diagnostic: Sto: Fully Met, TheDocument3 pagesObjective: Short Term Objectives: Diagnostic: Sto: Fully Met, TheWayne LoriaNo ratings yet
- Risk For Infection - NCP 3Document5 pagesRisk For Infection - NCP 3Daphne Cayaba BeltranNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanJehan Lois QuinesNo ratings yet
- Ob Topic 1 - Pprom - NCPDocument2 pagesOb Topic 1 - Pprom - NCPThelly MargalloNo ratings yet
- AshleyDocument2 pagesAshleyReihann EdresNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationJamie Haravata0% (1)
- B. Surgical ManagementDocument20 pagesB. Surgical ManagementNickaela CalalangNo ratings yet
- NCP Case Pre Nichole SarioDocument2 pagesNCP Case Pre Nichole SarioJoule PeirreNo ratings yet
- Planning Intervention Rationale Evaluation: Nursing Care Plan Problem DiagnosisDocument2 pagesPlanning Intervention Rationale Evaluation: Nursing Care Plan Problem DiagnosisRicardo Dela CruzNo ratings yet
- NCP Not FinishDocument3 pagesNCP Not FinishJay VillasotoNo ratings yet
- Far East Ern University: Nursing Care PlanDocument6 pagesFar East Ern University: Nursing Care PlanmharieeeNo ratings yet
- University of The East: Assessmen T Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesUniversity of The East: Assessmen T Diagnosis Planning Intervention Rationale EvaluationPATRICIA JEANNE JABIANNo ratings yet
- Congenital Megacolon: (Hirschsprung'SDocument20 pagesCongenital Megacolon: (Hirschsprung'STni JolieNo ratings yet
- Data Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale EvaluationDocument5 pagesData Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale EvaluationsteffiNo ratings yet
- Nursing Care Plan On Foul-Smelling LochiaDocument3 pagesNursing Care Plan On Foul-Smelling LochiaNE Tdr100% (1)
- "Ni-Raspa Ako Dahil Nalalag Yung Baby Ko." As Verbalized byDocument1 page"Ni-Raspa Ako Dahil Nalalag Yung Baby Ko." As Verbalized byMary AgorillaNo ratings yet
- Risk For Infection: Objective: - Fever - Lower Back Pain - Pain in Urinating For 1 WeekDocument8 pagesRisk For Infection: Objective: - Fever - Lower Back Pain - Pain in Urinating For 1 WeekJamie HaravataNo ratings yet
- Risk For Infection Related To High Glucose LevelsDocument2 pagesRisk For Infection Related To High Glucose LevelsDanica Kate GalleonNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationFrank Jomari MurilloNo ratings yet
- Kozier FundamentalDocument50 pagesKozier FundamentalgkixNo ratings yet
- Assessment Nursing Diagnosis Planning Implemantation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Implemantation Rationale EvaluationChloie Marie Rosalejos100% (1)
- PCDS NCP Surgery Ward DSPHDocument2 pagesPCDS NCP Surgery Ward DSPHJhomines NialaNo ratings yet
- Dhan Chan NCPDocument3 pagesDhan Chan NCPDhaneanne Marie ChanNo ratings yet
- Topics Included AreDocument31 pagesTopics Included ArepzeNo ratings yet
- Cebu Institute of Technology - University College of NursingDocument2 pagesCebu Institute of Technology - University College of NursingSergi Lee OrateNo ratings yet
- NCM 102: Gynecology Nursing ManagementDocument7 pagesNCM 102: Gynecology Nursing ManagementdubhieNo ratings yet
- Nursing Care Plan: IndependentDocument1 pageNursing Care Plan: IndependentJay Mar BabateNo ratings yet
- Nursing Care Plan TemplateDocument4 pagesNursing Care Plan TemplatetonnifritzcutamoraNo ratings yet
- A Postpartum Complication-Puerperal Infections Learning OutcomesDocument7 pagesA Postpartum Complication-Puerperal Infections Learning OutcomesDuchess Juliane Jose MirambelNo ratings yet
- Subjective: Long Term Objective: Long Term ObjectiveDocument1 pageSubjective: Long Term Objective: Long Term ObjectiveRAFNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationFredie O HadjimudinNo ratings yet
- ME Best Practices BrochureDocument3 pagesME Best Practices BrochureSachinNo ratings yet
- INFLAMATORY AND STDsDocument28 pagesINFLAMATORY AND STDsSasha BeyaoNo ratings yet
- Safari - 19 Apr 2020 at 18:27Document1 pageSafari - 19 Apr 2020 at 18:27Dream Big PrincessNo ratings yet
- C. Difficle Lay Summary PosterDocument1 pageC. Difficle Lay Summary PostermcwmckrackenNo ratings yet
- Nursing Care Plan - PROMDocument1 pageNursing Care Plan - PROMMarceline VueenNo ratings yet
- Depolonia NCPDocument6 pagesDepolonia NCPMary AllizaNo ratings yet
- NCP ManenDocument5 pagesNCP ManenArdiene Shallouvette GamosoNo ratings yet
- Ob2 Sas 14Document5 pagesOb2 Sas 14Ralph Louie ManagoNo ratings yet
- Potential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Document2 pagesPotential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Karl KiwisNo ratings yet
- Infection Control in The Outpatient Setting: Practice AlertDocument3 pagesInfection Control in The Outpatient Setting: Practice AlertYenny YuliantiNo ratings yet
- NCP (Revised)Document7 pagesNCP (Revised)Mary AllizaNo ratings yet
- After 4 Hours of Nursing Interventions, The Desired Outcomes of The Goals Are As FollowsDocument3 pagesAfter 4 Hours of Nursing Interventions, The Desired Outcomes of The Goals Are As FollowsPrancheska Abigayle Peneyra SantiagoNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationMeena KoushalNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationMeena KoushalNo ratings yet
- STI&STDDocument5 pagesSTI&STDRica Joy Sulicipan FiestaNo ratings yet
- Pedia Ward Chapter 4dDocument4 pagesPedia Ward Chapter 4dJohn Edward EscoteNo ratings yet
- Case Study ON Hodgkin LymphomaDocument8 pagesCase Study ON Hodgkin LymphomaMeena KoushalNo ratings yet
- Case Study ON Hodgkin LymphomaDocument8 pagesCase Study ON Hodgkin LymphomaMeena KoushalNo ratings yet
- NCP AidsDocument4 pagesNCP AidsMelvin D. RamosNo ratings yet
- 2 Nursing Care PlanDocument1 page2 Nursing Care PlanPauline AnesNo ratings yet
- Nature's Answer to Viral Threats: Understanding the Potency of Plant-Based AntiviralsFrom EverandNature's Answer to Viral Threats: Understanding the Potency of Plant-Based AntiviralsNo ratings yet
- The Science of Herbal Antivirals: Emerging Trends in Natural Viral Defense MechanismsFrom EverandThe Science of Herbal Antivirals: Emerging Trends in Natural Viral Defense MechanismsNo ratings yet
- Coronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowFrom EverandCoronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowNo ratings yet
- Corona Virus: Information You Need and How to Protect Yourself and Your Fellow Human BeingsFrom EverandCorona Virus: Information You Need and How to Protect Yourself and Your Fellow Human BeingsNo ratings yet
- Drug Mechanism of Action/ Side Effects Indication/ Contraindication Nursing Responsibilities Brand Name: Mechanism of Action IndicationDocument2 pagesDrug Mechanism of Action/ Side Effects Indication/ Contraindication Nursing Responsibilities Brand Name: Mechanism of Action IndicationRyan MirandaNo ratings yet
- Cues Nursing Diagnosis Goals/Outcomes Nursing Intervention Implementation Evaluation SubjectiveDocument5 pagesCues Nursing Diagnosis Goals/Outcomes Nursing Intervention Implementation Evaluation SubjectiveRyan MirandaNo ratings yet
- Plantable PencilDocument2 pagesPlantable PencilRyan MirandaNo ratings yet
- Responsible Use of Social MediaDocument8 pagesResponsible Use of Social MediaRyan MirandaNo ratings yet
- Guiwan Main Health Center and Lying-In Clinic, Zamboanga CityDocument17 pagesGuiwan Main Health Center and Lying-In Clinic, Zamboanga CityRyan MirandaNo ratings yet
- Guiwan Main Health Center and Lying-In Clinic, Zamboanga CityDocument17 pagesGuiwan Main Health Center and Lying-In Clinic, Zamboanga CityRyan MirandaNo ratings yet
- Nursing Care Plan San LuisDocument11 pagesNursing Care Plan San LuisRyan MirandaNo ratings yet
- Guia de Aprendizaje-QuantifiersDocument8 pagesGuia de Aprendizaje-Quantifiersangelita berdugoNo ratings yet
- Peugeot 206 P Dag Owners ManualDocument119 pagesPeugeot 206 P Dag Owners ManualAlex Rojas AguilarNo ratings yet
- Oh S Risk RegisterDocument83 pagesOh S Risk RegisterJacob YeboaNo ratings yet
- Assignment 2 Inorganic ChemistryDocument2 pagesAssignment 2 Inorganic Chemistryinam ullahNo ratings yet
- The Baldur's Gate Series 2 - Shadows of AmnDocument99 pagesThe Baldur's Gate Series 2 - Shadows of AmnJustin Moore100% (1)
- M8 Sensor UGuide 96-00001 REV H 073117Document50 pagesM8 Sensor UGuide 96-00001 REV H 073117Ashish KundapurNo ratings yet
- Project Proposal - BSMA 1202 byDocument19 pagesProject Proposal - BSMA 1202 byFabbi FababairNo ratings yet
- C10 CBSEPhy QueDocument4 pagesC10 CBSEPhy QueGeneric nameNo ratings yet
- Far Trek Continue VoyagesDocument148 pagesFar Trek Continue Voyageswintermute57100% (2)
- Sistemas de Refrigeracion Industrial en AmoniacoDocument102 pagesSistemas de Refrigeracion Industrial en AmoniacoDiego Trinidad100% (8)
- Гирокомпас 1 SPERRY REPEATERS - RUSDocument20 pagesГирокомпас 1 SPERRY REPEATERS - RUSVadim KiselevNo ratings yet
- Summary Sheet: Client Consultant Contractor Project: Package Ii: Document Name: Document No. 2 REVDocument42 pagesSummary Sheet: Client Consultant Contractor Project: Package Ii: Document Name: Document No. 2 REVPramod B.Wankhade100% (1)
- The Elephant and FriendsDocument2 pagesThe Elephant and FriendsENGLISHCLASS SMKN1SRKNo ratings yet
- Chemistry Project PDFDocument30 pagesChemistry Project PDFyash hiraniNo ratings yet
- The Hamburger Ate Boy Isn't Acceptable (Odd) But The Boy Ate The Hamburger Is Hamburger Doesn't Have This Property and The Noun Boy DoesDocument6 pagesThe Hamburger Ate Boy Isn't Acceptable (Odd) But The Boy Ate The Hamburger Is Hamburger Doesn't Have This Property and The Noun Boy DoesDania SaviraNo ratings yet
- Industry Alloted Property NoidaDocument193 pagesIndustry Alloted Property Noidaavinashtyagi0% (1)
- Foundation Fieldbus Manual (Allen Bradley)Document184 pagesFoundation Fieldbus Manual (Allen Bradley)Thia Dewi Ratnasari100% (1)
- Sample Question Paper - 3: Class - XDocument17 pagesSample Question Paper - 3: Class - XRehan AlamNo ratings yet
- Things That Make You Go HMMDocument2 pagesThings That Make You Go HMMmckee_jemNo ratings yet
- KW 18KWH Canada Interim Letters - KWUSDocument2 pagesKW 18KWH Canada Interim Letters - KWUSMecano PadNo ratings yet
- 2020 79th PNWIMC Annual Conference AnnouncementDocument2 pages2020 79th PNWIMC Annual Conference AnnouncementnwberryfoundationNo ratings yet
- CordaDocument7 pagesCordaAlone InNo ratings yet
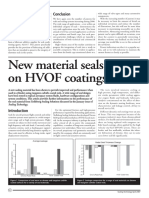
- New Material Seals Better On HVOF CoatingsDocument2 pagesNew Material Seals Better On HVOF Coatingssandbad2100% (2)
- D 661Document20 pagesD 661CristianNo ratings yet
- Prof. D. Pulla RaoDocument20 pagesProf. D. Pulla RaoAppan Kandala VasudevacharyNo ratings yet
- PPC Researched PointersDocument4 pagesPPC Researched PointershitmonNo ratings yet
- DC Ammeter and VoltmeterDocument21 pagesDC Ammeter and VoltmeterSyed Shehryar AliNo ratings yet
- Waqia Karbala Tareekh Ke Aine Me - Urdu BookDocument86 pagesWaqia Karbala Tareekh Ke Aine Me - Urdu BookABBAS ZAIDINo ratings yet
- Atomic Structure, Bohr Model and IsotopesDocument17 pagesAtomic Structure, Bohr Model and IsotopeskushanNo ratings yet