Download as docx, pdf, or txt
You might also like
- Bronchopneumonia Lesson PlanDocument16 pagesBronchopneumonia Lesson PlanUday Kumar88% (17)
- NCP SinusitisDocument7 pagesNCP SinusitisBeverly May Ambut71% (7)
- Long Term:: Iloilo Doctors' College College of NursingDocument7 pagesLong Term:: Iloilo Doctors' College College of NursingAbie Jean BalbontinNo ratings yet
- Critical Thinking ExerciseDocument1 pageCritical Thinking ExerciseMaye ArugayNo ratings yet
- 6 Pleural Effusion Nursing Care PlansDocument7 pages6 Pleural Effusion Nursing Care PlansShaina Fe RabaneraNo ratings yet
- Risk For Acute ConfusionDocument2 pagesRisk For Acute ConfusionChar PereaNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluationria_soriano_2No ratings yet
- NURSING-CARE-PLAN-Lung-Cancerxxx 1Document3 pagesNURSING-CARE-PLAN-Lung-Cancerxxx 1Caroline Cha100% (1)
- Health Education HTPDocument4 pagesHealth Education HTPizelelelsNo ratings yet
- Worksheet#2-Maintaining Asepsis: Medical Asepsis Includes All Practices Intended To Confine A SpecificDocument4 pagesWorksheet#2-Maintaining Asepsis: Medical Asepsis Includes All Practices Intended To Confine A SpecificCj MayoyoNo ratings yet
- 10 Rights of Drug Administration With Nursing ImplicationsDocument3 pages10 Rights of Drug Administration With Nursing ImplicationsJet Bautista100% (6)
- THINK AGAIN: Revisiting IM Injections: Bautista, Jesther Rowen B. BSN Iii-1 BLDH, 7-3, WARDDocument4 pagesTHINK AGAIN: Revisiting IM Injections: Bautista, Jesther Rowen B. BSN Iii-1 BLDH, 7-3, WARDJet BautistaNo ratings yet
- Herbal Tea Blending NOTESDocument9 pagesHerbal Tea Blending NOTESAna Lopes100% (2)
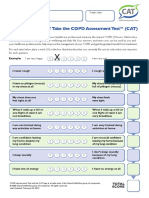
- How Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateDocument1 pageHow Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateAndreea BurceaNo ratings yet
- Philippine NLE Board ExamDocument46 pagesPhilippine NLE Board ExamDavid Lopez91% (22)
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearancejomerdalonaNo ratings yet
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternPaolo Anthony GonzalesNo ratings yet
- NCP For CTTDocument2 pagesNCP For CTTKay D. BeredoNo ratings yet
- Uti NCPDocument1 pageUti NCPAngelique Vinoya100% (2)
- Ineffective Breathing Pattern Pneumonia Nursing Care PlanDocument1 pageIneffective Breathing Pattern Pneumonia Nursing Care PlanJasonlee BaluyotNo ratings yet
- NCP LocDocument2 pagesNCP LocMel RodolfoNo ratings yet
- Activity Intolerance NCPDocument3 pagesActivity Intolerance NCPGen RodriguezNo ratings yet
- NCP Near DrowningDocument1 pageNCP Near Drowningchristine louise bernardoNo ratings yet
- Nursing DX: Acute Pain Related To Surgical Manipulation (Laminectomy) As Manifested by Reports of Pain On The Lumbar Area Rated As 7/10Document1 pageNursing DX: Acute Pain Related To Surgical Manipulation (Laminectomy) As Manifested by Reports of Pain On The Lumbar Area Rated As 7/10YESSAMIN GUADIZ100% (2)
- Nursing Care Plan: Cues Problem Scientific Reason Nursing Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Cues Problem Scientific Reason Nursing Intervention Rationale Evaluationeihjay-bravo-8041No ratings yet
- Assessment Diagnisis Planning Intervention Rationale Evaluation SubjectiveDocument2 pagesAssessment Diagnisis Planning Intervention Rationale Evaluation SubjectiveDanica Kate GalleonNo ratings yet
- NCP For CTTDocument1 pageNCP For CTTJen Rhae LimNo ratings yet
- Nursing Care Plan - Ineffective Airway ClearanceDocument1 pageNursing Care Plan - Ineffective Airway ClearanceLei OrtegaNo ratings yet
- Ineffective Breathing Pattern Pneumonia Nursing Care PlanDocument1 pageIneffective Breathing Pattern Pneumonia Nursing Care Planjustin_saneNo ratings yet
- NCP-Septic Shock (Acute Pain)Document3 pagesNCP-Septic Shock (Acute Pain)Ted anadiloNo ratings yet
- NCP DobDocument1 pageNCP DobsarahAcristobalNo ratings yet
- Introduction of FNCP 1Document2 pagesIntroduction of FNCP 1Helen QuibuyenNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJ.r. MercadoNo ratings yet
- NCPDocument5 pagesNCPRose AnnNo ratings yet
- Assessment Diagnosis Planning Nursing Interventions Rationale EvaluationDocument6 pagesAssessment Diagnosis Planning Nursing Interventions Rationale EvaluationChristine Denise Venus ValentinoNo ratings yet
- Ineffective Breathing Pattern As Evidenced by Use of Accessory Muscles and Episodes of DyspneaDocument3 pagesIneffective Breathing Pattern As Evidenced by Use of Accessory Muscles and Episodes of DyspneaNiel MinatozakiNo ratings yet
- NCP - TBDocument2 pagesNCP - TBPahw BaluisNo ratings yet
- Hyperthermia NCPDocument3 pagesHyperthermia NCPJayr DiazNo ratings yet
- NCPDocument9 pagesNCPYesha Mae MartinNo ratings yet
- NCP Ineffective Breathing PatternDocument3 pagesNCP Ineffective Breathing PatternNecheal BaayNo ratings yet
- Acute Pain NCPDocument2 pagesAcute Pain NCPBobby Valencerina100% (1)
- DeficientDocument2 pagesDeficientVANNEZA TRIXZY TAMPARONGNo ratings yet
- Drug StudyDocument4 pagesDrug Studyreanne_davidNo ratings yet
- NURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired PhysicalDocument1 pageNURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired Physicalmitchie riveraNo ratings yet
- Assessment Diagnosis Background Knowledge Planning Intervention Rationale Evaluation SubjectiveDocument3 pagesAssessment Diagnosis Background Knowledge Planning Intervention Rationale Evaluation SubjectiveAngelaNo ratings yet
- Nursing Care Plan Risk For Imbalance Body TemperatureDocument4 pagesNursing Care Plan Risk For Imbalance Body TemperatureCarl J.No ratings yet
- FATIGUE NCP Que Fransis A.Document4 pagesFATIGUE NCP Que Fransis A.Irene Grace BalcuevaNo ratings yet
- Capitol University: College of Nursing Cagayan de Oro CityDocument2 pagesCapitol University: College of Nursing Cagayan de Oro CityChaine Agolito100% (1)
- NCP PryllDocument6 pagesNCP PryllpjcolitaNo ratings yet
- Risk For Decreased Cardiac OutputDocument3 pagesRisk For Decreased Cardiac OutputSid Artemis FriasNo ratings yet
- NCP PediaDocument2 pagesNCP PediaJacinth Rizalino40% (5)
- Nursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NDocument2 pagesNursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NnananaNo ratings yet
- HTP PneumoniaDocument2 pagesHTP PneumoniaNikki ArmentaNo ratings yet
- Health Teaching PlanDocument4 pagesHealth Teaching PlanAirene Gonzales SantiagoNo ratings yet
- FNCP TB As A Health DeficitDocument5 pagesFNCP TB As A Health Deficitkuu faalNo ratings yet
- NCP PneumoniaDocument2 pagesNCP PneumoniaChristian Apelo Serquillos100% (2)
- Drug Study MaaloxDocument4 pagesDrug Study MaaloxJessie Batilo100% (2)
- NCP CroupDocument3 pagesNCP Croupaurezea100% (3)
- SNU49Document2 pagesSNU49Nora BacolNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective: Objective: STG: at The End of 1 DependentDocument1 pageNursing Care Plan Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective: Objective: STG: at The End of 1 DependentThomas FarrishNo ratings yet
- NCP Severe HypocalcemiaDocument4 pagesNCP Severe HypocalcemiaMark Zedrix MediarioNo ratings yet
- Assessment Diagnosis Planning Implementation Evaluation No Subjective Cues ObjectiveDocument3 pagesAssessment Diagnosis Planning Implementation Evaluation No Subjective Cues ObjectiveMaverick Lim100% (1)
- Ineffective Airway Clearance-NCPDocument5 pagesIneffective Airway Clearance-NCPJAMES ROD MARINDUQUENo ratings yet
- Nursing Care Plan: Group 1 Pangilinan Tadeo Sta. Maria Tecson Rivera SilvestreDocument8 pagesNursing Care Plan: Group 1 Pangilinan Tadeo Sta. Maria Tecson Rivera SilvestreTADEO, Joyce B.No ratings yet
- MCN NCPDocument4 pagesMCN NCPPEARL CHRISTINE CUDALNo ratings yet
- Nursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationDocument5 pagesNursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationMarivic Yuson MalagarNo ratings yet
- Dysfunctional Uterine BleedingDocument8 pagesDysfunctional Uterine BleedingJet BautistaNo ratings yet
- NCP - Risk For InfectionDocument2 pagesNCP - Risk For InfectionJet Bautista100% (1)
- NCP - Acute Abdominal PainDocument3 pagesNCP - Acute Abdominal PainJet Bautista100% (2)
- NCP HypertensionDocument2 pagesNCP HypertensionJet BautistaNo ratings yet
- Abnormal Uterine Bleeding - FinalDocument2 pagesAbnormal Uterine Bleeding - FinalJet BautistaNo ratings yet
- Myocardial Infarction/ Heart AttackDocument2 pagesMyocardial Infarction/ Heart AttackJet BautistaNo ratings yet
- Drug Study - Captopril CefuroximeDocument3 pagesDrug Study - Captopril CefuroximeJet BautistaNo ratings yet
- NCP Imbalanced NutritionDocument2 pagesNCP Imbalanced NutritionLouie James Velasco OstreaNo ratings yet
- Drug Study - CelebrexDocument1 pageDrug Study - CelebrexJet BautistaNo ratings yet
- Drug Study - AmpicillinDocument1 pageDrug Study - AmpicillinJet BautistaNo ratings yet
- Summary - Hyaline Membrane DiseaseDocument1 pageSummary - Hyaline Membrane DiseaseJet BautistaNo ratings yet
- Cord Care Case Slip - Lorma CollegesDocument1 pageCord Care Case Slip - Lorma CollegesJet BautistaNo ratings yet
- Drug Study - Nifedipine PODocument1 pageDrug Study - Nifedipine POJet BautistaNo ratings yet
- Drug Study - Hyoscine Butylbromide IVDocument1 pageDrug Study - Hyoscine Butylbromide IVJet Bautista80% (5)
- Chronic Obstructive Pulmonary DiseaseDocument7 pagesChronic Obstructive Pulmonary DiseaseCadiz Etrama Di RaizelNo ratings yet
- Bronkitis 2Document12 pagesBronkitis 2Lucky PuspitasariNo ratings yet
- CH 035 STG Bronchial AsthmaDocument11 pagesCH 035 STG Bronchial AsthmaNosirova ManijaNo ratings yet
- Accupressure For Cold and FluDocument5 pagesAccupressure For Cold and FluAmri Wicaksono Pribadi100% (1)
- Treatment of Influenza PDFDocument68 pagesTreatment of Influenza PDFavidmasterNo ratings yet
- Medical History Report Medical Prescreen QuestionnaireDocument4 pagesMedical History Report Medical Prescreen Questionnairejames antonioNo ratings yet
- Nash Repertory PDFDocument53 pagesNash Repertory PDFSatyendra RawatNo ratings yet
- Ineffective Airway Clearance-Nursing Care Plan For COPDDocument2 pagesIneffective Airway Clearance-Nursing Care Plan For COPDRnspeakcom100% (1)
- Nombre: Melany Yubitza Betzabe Fuentes Hernandez: Grado: Cuarto Medicina Sección: D Miss: Velia Minera Materia: InglésDocument9 pagesNombre: Melany Yubitza Betzabe Fuentes Hernandez: Grado: Cuarto Medicina Sección: D Miss: Velia Minera Materia: InglésArleth PerezNo ratings yet
- MATERIA MEDICA1 - UpdatedDocument26 pagesMATERIA MEDICA1 - UpdatedJerald BaliteNo ratings yet
- The Ear and Ear Points and Areas: Chapter TwoDocument16 pagesThe Ear and Ear Points and Areas: Chapter TwomihaelahristeaNo ratings yet
- Neumonia Aspirativa en PediatriaDocument28 pagesNeumonia Aspirativa en PediatriaFranklin Aranda100% (4)
- Asthma AlgorithmDocument13 pagesAsthma Algorithmgamecockusc1992No ratings yet
- Nursing InterventionsDocument68 pagesNursing Interventionsash aliNo ratings yet
- PneumoniaSystem DisorderDocument1 pagePneumoniaSystem DisorderAA DDNo ratings yet
- The Materia Medica of Acutes Activity DecreasedDocument24 pagesThe Materia Medica of Acutes Activity DecreasedMukeshPatelNo ratings yet
- Pre Employment Health AssessmentDocument7 pagesPre Employment Health AssessmentMP13No ratings yet
- 00 TB MCQ Quiz - Eng PDFDocument32 pages00 TB MCQ Quiz - Eng PDFSp PpvNo ratings yet
- Reminder Card Booklet v13 Print FinalDocument8 pagesReminder Card Booklet v13 Print FinalMayur MulyeNo ratings yet
- Makalah B.inggris EsiDocument11 pagesMakalah B.inggris EsiUMINo ratings yet
- Priority Disease ReportDocument24 pagesPriority Disease ReportalirrehmanNo ratings yet
- TriosDocument4 pagesTriosTej PrajapatiNo ratings yet
- Homeo MedicinesDocument31 pagesHomeo MedicinesSaleem RazaNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument62 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- 1 s2.0 S2287884X22001340 Main PDFDocument22 pages1 s2.0 S2287884X22001340 Main PDFashley lallaineNo ratings yet