Download as pdf or txt
You might also like
- Clinical Crown Lengthening in The Esthetic Zone2028Document12 pagesClinical Crown Lengthening in The Esthetic Zone2028AchyutSinhaNo ratings yet
- Blood Gas Analysis Ppt-3Document32 pagesBlood Gas Analysis Ppt-3Kresna Dharma SuryanaNo ratings yet
- Thoracoabdominal Aortic Aneurysms Open RepairDocument13 pagesThoracoabdominal Aortic Aneurysms Open RepairJonathan Frimpong AnsahNo ratings yet
- Imaging Thoracic Aortic AneurysmDocument11 pagesImaging Thoracic Aortic AneurysmHector Hernandez-SoriaNo ratings yet
- AngioNet A Convolutional Neural Network For VesselDocument14 pagesAngioNet A Convolutional Neural Network For VesselFederico WeckesserNo ratings yet
- IRB Proposal - PSU Aorta NLP ProjectDocument39 pagesIRB Proposal - PSU Aorta NLP Projectjhk0428No ratings yet
- Pitcher 2017Document6 pagesPitcher 2017anhca4519No ratings yet
- Art:10.1007/s11517 014 1165 7Document8 pagesArt:10.1007/s11517 014 1165 7Mustafa A. ElattarNo ratings yet
- A Deep Learning Based Automatic System For Intracranial Aneurysms Diagnosis OnDocument17 pagesA Deep Learning Based Automatic System For Intracranial Aneurysms Diagnosis Ontomou00999No ratings yet
- Deepaaa: Clinically Applicable and Generalizable Detection of Abdominal Aortic Aneurysm Using Deep LearningDocument10 pagesDeepaaa: Clinically Applicable and Generalizable Detection of Abdominal Aortic Aneurysm Using Deep LearningIzzHyukNo ratings yet
- Practical Aspects of IVUS-Guided Percutaneous Coronary InterventionDocument7 pagesPractical Aspects of IVUS-Guided Percutaneous Coronary InterventionRajesh JayakumarNo ratings yet
- 1 s2.0 S1875213618300913 MainDocument10 pages1 s2.0 S1875213618300913 MainSara TeixeiraNo ratings yet
- Gray-Matter Volume Estimate Score - A Novel Semi-Automatic Method Measuring Early Ischemic Change On CTDocument7 pagesGray-Matter Volume Estimate Score - A Novel Semi-Automatic Method Measuring Early Ischemic Change On CTkartini ciatawiNo ratings yet
- Errors and Margins in RadiotherapyDocument13 pagesErrors and Margins in RadiotherapychatsashNo ratings yet
- Cost-Effectiveness Analysis of The SAPIEN 3 Transcatheter Aortic Valve Implant in Patients With Symptomatic Severe Aortic StenosisDocument9 pagesCost-Effectiveness Analysis of The SAPIEN 3 Transcatheter Aortic Valve Implant in Patients With Symptomatic Severe Aortic StenosisGaal PinNo ratings yet
- Endoscopic Submucosal Dissection For Early Gastric Cancer: Are Expanded Resection Criteria Safe For Western Patients?Document11 pagesEndoscopic Submucosal Dissection For Early Gastric Cancer: Are Expanded Resection Criteria Safe For Western Patients?Mayra Camila PerezNo ratings yet
- 3-Dimensional Ultrasound in Carotid Stenosis Quantitation and Beyond - JACC, 2018Document3 pages3-Dimensional Ultrasound in Carotid Stenosis Quantitation and Beyond - JACC, 2018flavio_duarte3880No ratings yet
- 2017 Article 233Document8 pages2017 Article 233Alfeus GradyNo ratings yet
- 1 s2.0 S0735109723064550 MainDocument20 pages1 s2.0 S0735109723064550 MainWaleed Ismail KamelNo ratings yet
- Cardiologia: Patient-Specific 3D Printing Simulation To Guide Complex Coronary InterventionDocument4 pagesCardiologia: Patient-Specific 3D Printing Simulation To Guide Complex Coronary InterventionJoãoNo ratings yet
- CT Support of Cardiac Structural Interventions: Review ArticleDocument12 pagesCT Support of Cardiac Structural Interventions: Review ArticlefibiaNo ratings yet
- Osareh 2010Document7 pagesOsareh 2010VivekNo ratings yet
- Defreitas 2018Document6 pagesDefreitas 2018drrajeshb77No ratings yet
- Optimal Bowel Resection Margin in Colon Cancer Surgery 2023Document13 pagesOptimal Bowel Resection Margin in Colon Cancer Surgery 2023CIRUGÍA ONCOLÓGICA ABDOMENNo ratings yet
- Angiographic Characterization of Lesion Morphology: Cover StoryDocument6 pagesAngiographic Characterization of Lesion Morphology: Cover StorysuckeydluffyNo ratings yet
- Vera 2019 J. Phys. Conf. Ser. 1160 012001Document8 pagesVera 2019 J. Phys. Conf. Ser. 1160 012001veramig1396No ratings yet
- The Role of AI in The Echocardiogrphy Worklow 1699588143Document8 pagesThe Role of AI in The Echocardiogrphy Worklow 1699588143giovannimacNo ratings yet
- 1526602817740133Document9 pages1526602817740133Enrique San NorbertoNo ratings yet
- 10 3400@avd Ra 18-00139Document5 pages10 3400@avd Ra 18-00139Younis SayefNo ratings yet
- Stroke Mimics VagalDocument12 pagesStroke Mimics VagalBrunaProençaNo ratings yet
- Glomus CcarotidasDocument8 pagesGlomus CcarotidasJuan TijerinaNo ratings yet
- Abdominal Aortic Calcification On A Plain X-Ray and The Relation With Significant Coronary Artery Disease in Asymptomatic Chronic Dialysis PatientsDocument7 pagesAbdominal Aortic Calcification On A Plain X-Ray and The Relation With Significant Coronary Artery Disease in Asymptomatic Chronic Dialysis PatientsArdiansyah Yolanda PutraNo ratings yet
- Magnetic Resonance Imaging of Breast Cancer: Factors Affecting The Accuracy of Preoperative Lesion SizingDocument9 pagesMagnetic Resonance Imaging of Breast Cancer: Factors Affecting The Accuracy of Preoperative Lesion SizingkhadijawhasNo ratings yet
- IkjjjkjDocument7 pagesIkjjjkjMohammad AjiNo ratings yet
- Intravascular Ultrasound Criteria For Determination of Optimal Longitudinal Positioning of Sirolimus-Eluting StentsDocument8 pagesIntravascular Ultrasound Criteria For Determination of Optimal Longitudinal Positioning of Sirolimus-Eluting StentsRicardo Novoa AlvarezNo ratings yet
- The Role of MRI Quantitative Assessment in PreoperativeDocument8 pagesThe Role of MRI Quantitative Assessment in PreoperativeRonWuNo ratings yet
- Al-Mansour2021 Validation of A Simple Technique of Volumetric Analysis of Complex Hernias Without 3D ReconstructionDocument7 pagesAl-Mansour2021 Validation of A Simple Technique of Volumetric Analysis of Complex Hernias Without 3D ReconstructionEham AroraNo ratings yet
- Lopez Campos2021 Article SEORSBRT SGStereotacticBodyRadDocument12 pagesLopez Campos2021 Article SEORSBRT SGStereotacticBodyRadMaria MuñozNo ratings yet
- Effects of Statins On Coronary Atherosclerotic Plaques The PARADIGM Study.Document10 pagesEffects of Statins On Coronary Atherosclerotic Plaques The PARADIGM Study.Oscar OrtegaNo ratings yet
- CT Angiography Versus Digital Subtraction Angiography For Intracranial Vascular Pathology in A Clinical SettingDocument9 pagesCT Angiography Versus Digital Subtraction Angiography For Intracranial Vascular Pathology in A Clinical SettingPari Pengda BaliNo ratings yet
- Doble ArcoDocument19 pagesDoble ArcoCorazon MabelNo ratings yet
- CABG ConduitDocument15 pagesCABG ConduitSundaresan SankarNo ratings yet
- Deep Learning For Automated Cerebral Aneurysm Detection On Computed Tomography ImagesDocument9 pagesDeep Learning For Automated Cerebral Aneurysm Detection On Computed Tomography Imagestomou00999No ratings yet
- CMRMitralRegurgitation - reviEW.jacc .2018Document17 pagesCMRMitralRegurgitation - reviEW.jacc .2018PanfilAlinaNo ratings yet
- Metaanalisis FD en Agudo Ajnr 223 Pacientes CagnazoDocument7 pagesMetaanalisis FD en Agudo Ajnr 223 Pacientes CagnazoangelNo ratings yet
- AutomaticLiverTumor PDFDocument18 pagesAutomaticLiverTumor PDFMuhammad Zaka Ud DinNo ratings yet
- Recent Update On Carotid Endarterectomy Versus Carotid Artery StentingDocument8 pagesRecent Update On Carotid Endarterectomy Versus Carotid Artery StentingYahya AlmalkiNo ratings yet
- Zhao 2018Document7 pagesZhao 2018Alexandru PusneiNo ratings yet
- Changes of Size and Shape of Small, Unruptured Intracranial Aneurysms in Repeated Computed Tomography Angiography StudiesDocument11 pagesChanges of Size and Shape of Small, Unruptured Intracranial Aneurysms in Repeated Computed Tomography Angiography StudiesAnand KumarNo ratings yet
- 10 1016@j Ajodo 2016 06 034Document10 pages10 1016@j Ajodo 2016 06 034Soe San KyawNo ratings yet
- 4644 16382 1 PBDocument8 pages4644 16382 1 PBWahyu RianiNo ratings yet
- Abou Elkassem Et Al 2021 Role of Imaging in Renal Cell Carcinoma A Multidisciplinary PerspectiveDocument21 pagesAbou Elkassem Et Al 2021 Role of Imaging in Renal Cell Carcinoma A Multidisciplinary Perspectiveandrescabrera24No ratings yet
- CT For Treatment Selection in Acute Ischemic Stroke: A Code Stroke PrimerDocument22 pagesCT For Treatment Selection in Acute Ischemic Stroke: A Code Stroke PrimerSantiago TapiaNo ratings yet
- Incidence of Lower Eyelid Asymmetry: An Anthropometric Analysis of 204 PatientsDocument6 pagesIncidence of Lower Eyelid Asymmetry: An Anthropometric Analysis of 204 PatientsAndrewNo ratings yet
- 1 s2.0 S1726490114002822 MainDocument6 pages1 s2.0 S1726490114002822 MainS Ram KishoreNo ratings yet
- 1093-39 Mri-1622746065Document4 pages1093-39 Mri-1622746065Khurram ChauhanNo ratings yet
- Patient Prosthesis MismatchDocument19 pagesPatient Prosthesis Mismatchtalal.fazmin1No ratings yet
- Barber 2018Document4 pagesBarber 2018Boris CanahuireNo ratings yet
- Breast Mri ThesisDocument9 pagesBreast Mri ThesisKaela Johnson100% (2)
- 3D Partial NephrctDocument10 pages3D Partial NephrctnadalNo ratings yet
- Venous Thromboembolism in AestheticDocument11 pagesVenous Thromboembolism in Aestheticdoc100fuegosNo ratings yet
- SPN BrochureDocument2 pagesSPN BrochureIzzHyukNo ratings yet
- Deepaaa: Clinically Applicable and Generalizable Detection of Abdominal Aortic Aneurysm Using Deep LearningDocument10 pagesDeepaaa: Clinically Applicable and Generalizable Detection of Abdominal Aortic Aneurysm Using Deep LearningIzzHyukNo ratings yet
- Smart Cities Shifting Asia - Ubs 2019 enDocument58 pagesSmart Cities Shifting Asia - Ubs 2019 enIzzHyukNo ratings yet
- Yes This Is A TitleDocument8 pagesYes This Is A TitleIzzHyukNo ratings yet
- Health & Safety at Work Act 2015 PDFDocument14 pagesHealth & Safety at Work Act 2015 PDFIzzHyukNo ratings yet
- 373 FullDocument7 pages373 FullIzzHyukNo ratings yet
- User's Guide of Uprgading The M.NT68676.2A FirmwareDocument10 pagesUser's Guide of Uprgading The M.NT68676.2A FirmwareIzzHyukNo ratings yet
- Enhanced Manufacturing Possibilities Using Multi-Materials in Laser Metal DepositionDocument11 pagesEnhanced Manufacturing Possibilities Using Multi-Materials in Laser Metal DepositionIzzHyukNo ratings yet
- Hemelb Acceleration and Visualization For Cerebral AneurysmsDocument5 pagesHemelb Acceleration and Visualization For Cerebral AneurysmsIzzHyukNo ratings yet
- Shey PDFDocument1 pageShey PDFIzzHyukNo ratings yet
- Ryan Holiday: Trust Me, I'm Lying: Confessions of A Media ManipulatorDocument4 pagesRyan Holiday: Trust Me, I'm Lying: Confessions of A Media ManipulatorIzzHyukNo ratings yet
- Banner PVA225P6E Datasheet PDFDocument8 pagesBanner PVA225P6E Datasheet PDFIzzHyukNo ratings yet
- PaperCALCOPRINT ENDocument1 pagePaperCALCOPRINT ENIzzHyukNo ratings yet
- Pid TuningDocument11 pagesPid TuningIzzHyukNo ratings yet
- Handbook of Timing Belts and Pulleys: Section 1 IntroductionDocument3 pagesHandbook of Timing Belts and Pulleys: Section 1 IntroductionIzzHyukNo ratings yet
- Step3S: 3-4 Axes Stepper Motor Driver BoardDocument2 pagesStep3S: 3-4 Axes Stepper Motor Driver BoardIzzHyukNo ratings yet
- Digistart STV 2313: Electronic Soft StarterDocument40 pagesDigistart STV 2313: Electronic Soft StarterIzzHyukNo ratings yet
- ADF Main Spindle Motors: RexrothDocument55 pagesADF Main Spindle Motors: RexrothIzzHyukNo ratings yet
- Stepper - Why Steppers Loose Steps - WPDocument4 pagesStepper - Why Steppers Loose Steps - WPIzzHyukNo ratings yet
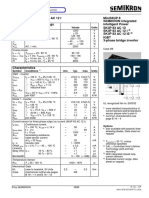
- SKIIP83AC12 Semikron PDFDocument5 pagesSKIIP83AC12 Semikron PDFIzzHyukNo ratings yet
- Ryan Holiday: Trust Me, I'm Lying: Confessions of A Media ManipulatorDocument4 pagesRyan Holiday: Trust Me, I'm Lying: Confessions of A Media ManipulatorIzzHyukNo ratings yet
- Laser Error List PDFDocument32 pagesLaser Error List PDFIzzHyuk100% (1)
- COVID-19 EHS PlanDocument18 pagesCOVID-19 EHS Planyusuf BakhtiarNo ratings yet
- Mapeh 8Document2 pagesMapeh 8Jeje MonsantoNo ratings yet
- OMS Central Nervous SystemDocument312 pagesOMS Central Nervous SystemDenisa Gherman100% (1)
- Medical Transcription: Candice B. Relieve, M.DDocument31 pagesMedical Transcription: Candice B. Relieve, M.DMaricar U. Payongayong100% (2)
- 10 1016@j Ejogrb 2015 09 020Document5 pages10 1016@j Ejogrb 2015 09 020samuel tapia pardoNo ratings yet
- Joining IntimationDocument2 pagesJoining IntimationDurga Prasad SeerapuNo ratings yet
- Biology GCE 2010 June Paper 1 Mark SchemeDocument10 pagesBiology GCE 2010 June Paper 1 Mark SchemeRicky MartinNo ratings yet
- Đề 22.Mh2022.Key Chi TiếtDocument32 pagesĐề 22.Mh2022.Key Chi TiếtThao Thanh PhamNo ratings yet
- Head InjuryDocument61 pagesHead InjuryRicky Cornelius TariganNo ratings yet
- No. 279 December 2014: Please NoteDocument6 pagesNo. 279 December 2014: Please NoteCornwall and Isles of Scilly LMCNo ratings yet
- Executive Order No. - : Series of 2021Document2 pagesExecutive Order No. - : Series of 2021BARANGAY ANIBAN 2No ratings yet
- Chapter-2 Hunger and Malnutrition in India - Policies and ProgrammesDocument35 pagesChapter-2 Hunger and Malnutrition in India - Policies and ProgrammesJames KnotNo ratings yet
- 2016 Laboratory GuidelinesDocument61 pages2016 Laboratory GuidelinesDenySidiqMulyonoCht100% (1)
- BW Filmfill EngDocument4 pagesBW Filmfill EngkylegazeNo ratings yet
- Hubungan Pengetahuan Ibu Terhadap Pemberian Makanan Pendamping Asi (MP-ASI) Dengan Kejadian Stunting Pada Baduta Di Kabupaten Pandeglang Provinsi BantenDocument7 pagesHubungan Pengetahuan Ibu Terhadap Pemberian Makanan Pendamping Asi (MP-ASI) Dengan Kejadian Stunting Pada Baduta Di Kabupaten Pandeglang Provinsi BantenUmroatul AlfiyahNo ratings yet
- Ethics in Mental Health NursingDocument27 pagesEthics in Mental Health Nursingvallal100% (2)
- How To Start Virgin CocoDocument6 pagesHow To Start Virgin CocoB GirishNo ratings yet
- Guidance On The in Vitro Diagnostic Medical Devices Directive 98/79/ECDocument15 pagesGuidance On The in Vitro Diagnostic Medical Devices Directive 98/79/ECRick GreenNo ratings yet
- Human Nocardia Infections: A Review of Pulmonary NocardiosisDocument7 pagesHuman Nocardia Infections: A Review of Pulmonary NocardiosisAyu Nurislami WulandariNo ratings yet
- Serbia Cleanrooms Seminar 2Document31 pagesSerbia Cleanrooms Seminar 2Luis Gerardo Almanza LlanosNo ratings yet
- Assessment of Fetal WellbeingDocument177 pagesAssessment of Fetal Wellbeingvrutipatel100% (1)
- Tandem Loading Guidelines v1 21Document129 pagesTandem Loading Guidelines v1 21Cindy100% (2)
- 3rd and 4th Stage of LaborDocument8 pages3rd and 4th Stage of LaborMarco Paulo Reyes NaoeNo ratings yet
- Rosen - Medicina de Urgencias Tomo 1.abbyyDocument994 pagesRosen - Medicina de Urgencias Tomo 1.abbyyJessica Wiley100% (9)
- CSFI Letter of ProposalDocument2 pagesCSFI Letter of Proposalhannah jade judillaNo ratings yet
- Rural-Urban-migration - Study IGCSEDocument25 pagesRural-Urban-migration - Study IGCSEmahika gaurNo ratings yet
- Acknowledgement: M Mohibuz Zaman, Chief Operating Officer For Giving Us The Opportunity ToDocument81 pagesAcknowledgement: M Mohibuz Zaman, Chief Operating Officer For Giving Us The Opportunity ToShahed AhmedNo ratings yet