Download as pdf or txt
You might also like
- Fractures Related To Occlusal Overload With Single Posterior Implants A Clinical ReportDocument6 pagesFractures Related To Occlusal Overload With Single Posterior Implants A Clinical ReportSurya TejaNo ratings yet
- ANSYS Fluent in ANSYS Workbench User's Guide PDFDocument106 pagesANSYS Fluent in ANSYS Workbench User's Guide PDFMarcos Vinicius100% (1)
- Pi Is 0889540615013311Document5 pagesPi Is 0889540615013311msoaresmirandaNo ratings yet
- Fracture Resistance and Microleakage of Endocrowns Utilizing Three CAD-CAM BlocksDocument10 pagesFracture Resistance and Microleakage of Endocrowns Utilizing Three CAD-CAM BlocksZen AhmadNo ratings yet
- Vertical 3D Bone Reconstruction With Simultaneous Implantation A Case Series ReportDocument9 pagesVertical 3D Bone Reconstruction With Simultaneous Implantation A Case Series ReportYuki MuraNo ratings yet
- Vigolo, Zaccaria - 2010 - Clinical Evaluation of Marginal Bone Level Change of Multiple Adjacent Implants Restored With Splinted and NonDocument7 pagesVigolo, Zaccaria - 2010 - Clinical Evaluation of Marginal Bone Level Change of Multiple Adjacent Implants Restored With Splinted and NonRenato PetilleNo ratings yet
- 2005 Rojas VizcayaDocument14 pages2005 Rojas Vizcayacasto.carpetasmiaNo ratings yet
- Improvement of An Additively Manufactured Subperiosteal Implant Structure Design by Finite Elements Based Topological OptimizationDocument9 pagesImprovement of An Additively Manufactured Subperiosteal Implant Structure Design by Finite Elements Based Topological OptimizationTîrban Pantelimon FlorinNo ratings yet
- Mandibular Molar Protraction With Orthodontic Temporary Anchorage Devices: A Case ReportDocument4 pagesMandibular Molar Protraction With Orthodontic Temporary Anchorage Devices: A Case ReportKanish AggarwalNo ratings yet
- Implant-Retained Cantilever Fixed Prosthesis: Where and WhenDocument4 pagesImplant-Retained Cantilever Fixed Prosthesis: Where and WhenSitiKhadijahNo ratings yet
- 10 1111@cid 12748Document8 pages10 1111@cid 12748Behnam TaghaviNo ratings yet
- 10 11607@jomi 8122Document8 pages10 11607@jomi 8122Marlene Kasumi Gantier TakanoNo ratings yet
- Prosthetic Rehabilitation of Mandibular Defects With Fixed-Removable Partial Denture Prosthesis Using Precision Attachment - A Twin Case ReportDocument17 pagesProsthetic Rehabilitation of Mandibular Defects With Fixed-Removable Partial Denture Prosthesis Using Precision Attachment - A Twin Case ReportIvy MedNo ratings yet
- Immediate Versus Conventional Loading of Implant-Supported Maxillary Overdentures: A Finite Element Stress AnalysisDocument7 pagesImmediate Versus Conventional Loading of Implant-Supported Maxillary Overdentures: A Finite Element Stress AnalysisMr OdontologiaNo ratings yet
- Hingsammer 2017 CIDRR - The Influence of C-I Ratio On MBL Short Splinted ImplantsDocument9 pagesHingsammer 2017 CIDRR - The Influence of C-I Ratio On MBL Short Splinted ImplantsZhiyi LinNo ratings yet
- TAD Supported Mandibular Space ClosureDocument6 pagesTAD Supported Mandibular Space ClosureAly OsmanNo ratings yet
- Ammar 2011Document13 pagesAmmar 2011manju deviNo ratings yet
- Bodily Distalization of Molars With Absolute AnchorageDocument12 pagesBodily Distalization of Molars With Absolute AnchorageAnamika AttrishiNo ratings yet
- Alternativas en Fenestración de Iplantes.2006.050135 3Document6 pagesAlternativas en Fenestración de Iplantes.2006.050135 3Daniela Alejandra CardonaNo ratings yet
- Bio Orto Movement GigiDocument7 pagesBio Orto Movement GigiRisyaRahmadaniNo ratings yet
- 6.preprosthetic Surgery A Review of LiteratureDocument7 pages6.preprosthetic Surgery A Review of Literaturemirah indrianiNo ratings yet
- Prosthetic Considerations: R Mericske-SternDocument11 pagesProsthetic Considerations: R Mericske-SternSilpayNo ratings yet
- Esthetic Rehabilitation of A Worn Dentition With A Minimally Invasive Prost... : EBSCOhostDocument21 pagesEsthetic Rehabilitation of A Worn Dentition With A Minimally Invasive Prost... : EBSCOhostNaoki Mezarina100% (1)
- Prosthetic Considerations: R Mericske-SternDocument11 pagesProsthetic Considerations: R Mericske-SternpmodontologiaNo ratings yet
- Bone GraftDocument4 pagesBone Graftsmansa123No ratings yet
- Mandible FracturesDocument17 pagesMandible FracturesYaser JasNo ratings yet
- Point of CareDocument6 pagesPoint of Carepbo4No ratings yet
- Screw Tent Pole Graft TechniqueDocument8 pagesScrew Tent Pole Graft TechniqueSweet ToothNo ratings yet
- Oh 2010Document5 pagesOh 2010gbaez.88No ratings yet
- 1 s2.0 S0278239107016424 MainDocument11 pages1 s2.0 S0278239107016424 MainDANTE DELEGUERYNo ratings yet
- Bmri2021 5699962Document16 pagesBmri2021 5699962Pablo Gutiérrez Da VeneziaNo ratings yet
- Rehabilitation of Sieberts Class III Defect Using Fixed Removable Prosthesis (Andrew's Bridge)Document5 pagesRehabilitation of Sieberts Class III Defect Using Fixed Removable Prosthesis (Andrew's Bridge)drgunNo ratings yet
- MSE 10.1016@j.ajodo.2016.10.025Document11 pagesMSE 10.1016@j.ajodo.2016.10.025Neycer Catpo NuncevayNo ratings yet
- Socket Shield Technique Vs Conventional Immediate Implant Placement With Immediate Temporization. Randomized Clinical TrialDocument10 pagesSocket Shield Technique Vs Conventional Immediate Implant Placement With Immediate Temporization. Randomized Clinical TrialeveraldocruzNo ratings yet
- Fixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Document11 pagesFixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Nathawat PleumsamranNo ratings yet
- Cicatrizador PersonalizadoDocument9 pagesCicatrizador PersonalizadoJosué SamaniegoNo ratings yet
- PAPER 5 - Anclaje EsqueletalDocument8 pagesPAPER 5 - Anclaje EsqueletalNicolás ValenzuelaNo ratings yet
- 1 s2.0 S2468785523000915 MainDocument6 pages1 s2.0 S2468785523000915 MainHakim TaghzoutiNo ratings yet
- Surgical Extrusion With An Atraumatic Extraction System: A Clinical StudyDocument7 pagesSurgical Extrusion With An Atraumatic Extraction System: A Clinical StudyFebri YolandaNo ratings yet
- Zufia e Sans 2022Document14 pagesZufia e Sans 2022henriquetaranNo ratings yet
- 2023 StressDocument9 pages2023 StressEslam ShawkyNo ratings yet
- 2000 J C. H S W A: Udson Ickey Cientific Riting WardDocument6 pages2000 J C. H S W A: Udson Ickey Cientific Riting WardPremshith CpNo ratings yet
- 2020 Article 265Document7 pages2020 Article 265Fabian BarretoNo ratings yet
- Jap 11 48Document7 pagesJap 11 48Zerelie MaudNo ratings yet
- Aula EduinaDocument7 pagesAula EduinaJoão S NetoNo ratings yet
- Clinical Longevity of Removable Partial Dentures Retained by Telescopic Crowns: Outcome of The Double Crown With Clearance FitDocument8 pagesClinical Longevity of Removable Partial Dentures Retained by Telescopic Crowns: Outcome of The Double Crown With Clearance FitStephanie NúñezNo ratings yet
- Passant Connection Screw of Dental Implants An inDocument8 pagesPassant Connection Screw of Dental Implants An inJose Manuel Quintero RomeroNo ratings yet
- Estabilidad Microimplantes - 1Document7 pagesEstabilidad Microimplantes - 1Marcelo ChinizacaNo ratings yet
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocument7 pagesThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin Sapri100% (1)
- Cirugía OralDocument7 pagesCirugía OralLenny GrauNo ratings yet
- Screw-Versus Cement-Retained Implant RestorationsDocument8 pagesScrew-Versus Cement-Retained Implant RestorationsMia V. UckrmnnNo ratings yet
- Ridge Preservation Techniques For Implant Therapy: JO M I 2009 24 :260-271Document12 pagesRidge Preservation Techniques For Implant Therapy: JO M I 2009 24 :260-271Viorel FaneaNo ratings yet
- Anatomic Considerations in Dental Implant Surgery: Mitra SadrameliDocument22 pagesAnatomic Considerations in Dental Implant Surgery: Mitra SadrameliSebastián BernalNo ratings yet
- Comparison Between Intermaxillary Fixation With Screws and An Arch Bar For Mandibular FractureDocument3 pagesComparison Between Intermaxillary Fixation With Screws and An Arch Bar For Mandibular Fracture6hd6mnrzw2No ratings yet
- Abutment Options For The Restoration of The Malalinged Implant 2016 PDFDocument5 pagesAbutment Options For The Restoration of The Malalinged Implant 2016 PDFmarwa100% (1)
- Mantenimiento de Prótesis Maxilares ImplantosoportadasDocument10 pagesMantenimiento de Prótesis Maxilares ImplantosoportadasKAREN DANA KARELYA SIQUERO VERANo ratings yet
- 15 Years Rand Cobtrolled Trial 2011Document7 pages15 Years Rand Cobtrolled Trial 2011Hicham AL KHAYARNo ratings yet
- A Predictable All-Digital Work Ow To Retrofit A Crown To An Existing Removable ProsthesisDocument3 pagesA Predictable All-Digital Work Ow To Retrofit A Crown To An Existing Removable ProsthesismaiNo ratings yet
- Conservative Mangement of Tilted AbutmentsDocument3 pagesConservative Mangement of Tilted Abutmentsrayavarapu sunilNo ratings yet
- Pi Is 1043181008000225Document5 pagesPi Is 1043181008000225drbhaskar128No ratings yet
- Adv IC Engines Assignment No 2.Document3 pagesAdv IC Engines Assignment No 2.Madhupriya KalahastiNo ratings yet
- GermanDocument25 pagesGermanMadhupriya KalahastiNo ratings yet
- Biomaterial Fabrication Techniques: Arjun G Namboodiri Polymer Processing Laboratory 4/6/10Document48 pagesBiomaterial Fabrication Techniques: Arjun G Namboodiri Polymer Processing Laboratory 4/6/10Madhupriya KalahastiNo ratings yet
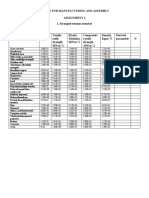
- Design For Manufacturing and Assembly Assignment 2 1. Strongest Tension MemberDocument1 pageDesign For Manufacturing and Assembly Assignment 2 1. Strongest Tension MemberMadhupriya KalahastiNo ratings yet
- 10 1016@j Compbiomed 2019 03 004 PDFDocument41 pages10 1016@j Compbiomed 2019 03 004 PDFMadhupriya KalahastiNo ratings yet
- Desktop Engineering - 2014-02Document52 pagesDesktop Engineering - 2014-02Бушинкин ВладиславNo ratings yet
- Fluent-Intro 14.5 L02 IntroCFDDocument13 pagesFluent-Intro 14.5 L02 IntroCFDKarl-Andrew Kluge RudisileNo ratings yet
- ANSYS Release Notes 190 PDFDocument146 pagesANSYS Release Notes 190 PDFAle100% (1)
- Design Modification & Analysis For Venturi Section of Invelox System To Maximize Power Using Multiple Wind TurbineDocument26 pagesDesign Modification & Analysis For Venturi Section of Invelox System To Maximize Power Using Multiple Wind TurbineRJ ManiNo ratings yet
- Crash AnalysisDocument5 pagesCrash AnalysisMomo PierreNo ratings yet
- Getting Started With ANSYS WorkbenchDocument0 pagesGetting Started With ANSYS WorkbenchasgharmahfoozNo ratings yet
- ANSYS Workbench Concrete Pavement ModelDocument8 pagesANSYS Workbench Concrete Pavement ModelMohamed Nageeb SalemNo ratings yet
- FEM TrendsinBiosciences8Document6 pagesFEM TrendsinBiosciences8Ahmad SawanNo ratings yet
- HyperMesh 12.0 Tutorials-ANSYSDocument60 pagesHyperMesh 12.0 Tutorials-ANSYSĐỗ Minh ĐứcNo ratings yet
- Modelling and Simulation Offlow Induced Vibrations in Vertical Axis Wind Turbine BladeDocument11 pagesModelling and Simulation Offlow Induced Vibrations in Vertical Axis Wind Turbine BladeElena VlangarNo ratings yet
- Engineering Data Users GuideDocument86 pagesEngineering Data Users GuideAjay KumarNo ratings yet
- Comparison of Two-Phase Pipe Flow in Openfoam With A Mechanistic ModelDocument14 pagesComparison of Two-Phase Pipe Flow in Openfoam With A Mechanistic ModelMusa MohammadNo ratings yet
- Ansys All You Need To Know About Hardware For SimulationDocument36 pagesAnsys All You Need To Know About Hardware For Simulationnovkovic1984No ratings yet
- Uday Ramu Pujari-ResumeDocument2 pagesUday Ramu Pujari-ResumePujari RamuNo ratings yet
- Contact Element TutorialsDocument15 pagesContact Element TutorialsSushil DhunganaNo ratings yet
- An Introduction To HFSSDocument114 pagesAn Introduction To HFSSMs. Deepthy G.S.100% (1)
- Gaurav Bhonsule: SR.D EDocument5 pagesGaurav Bhonsule: SR.D EgauvNo ratings yet
- Assignment No 1-2020-FEA Intro PDFDocument2 pagesAssignment No 1-2020-FEA Intro PDFTinashe ErwinNo ratings yet
- AA V6 I1 High Fidelity FSIDocument3 pagesAA V6 I1 High Fidelity FSIpriyankar007No ratings yet
- CFD TrainingDocument25 pagesCFD TrainingRui AuditoreNo ratings yet
- ANSYS Fluent Text Command ListDocument134 pagesANSYS Fluent Text Command ListhafidzfbNo ratings yet
- Program Book Rev 8Document115 pagesProgram Book Rev 8TuswanNo ratings yet
- .Design and Analysis of A Shock Absorber by Varying Spring Materials - Analysis Using Fea TechniqueDocument9 pages.Design and Analysis of A Shock Absorber by Varying Spring Materials - Analysis Using Fea TechniqueManjunath ReddyNo ratings yet
- ANSYS ACT Developers Guide PDFDocument506 pagesANSYS ACT Developers Guide PDFojbulmerNo ratings yet
- CFX TBR Aeromechanics CFD 18.0 Module01 Intro To ANSYSDocument6 pagesCFX TBR Aeromechanics CFD 18.0 Module01 Intro To ANSYSAnubhav SharmaNo ratings yet
- Pressure Based Coupled Solver, Hybrid InitializationDocument2 pagesPressure Based Coupled Solver, Hybrid InitializationAleksandar PasicNo ratings yet
- Analyzer ProfileDocument13 pagesAnalyzer Profilesuryawanshi_nitinNo ratings yet
- ANSYS FLUENT Magnetohydrodynamics (MHD) Module ManualDocument48 pagesANSYS FLUENT Magnetohydrodynamics (MHD) Module ManualAyoub MaDridiNo ratings yet
- Chemcad PresentationDocument39 pagesChemcad PresentationRana MubasherNo ratings yet