Download as docx, pdf, or txt
You might also like
- Alexander's Care of The Patient in Surgery by Rothrock (17th Edition)Document1,217 pagesAlexander's Care of The Patient in Surgery by Rothrock (17th Edition)ezinne obinna-uma100% (2)
- Critical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFDocument335 pagesCritical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFSami Atawi100% (1)
- Porths Pathophysiology Concepts of Altered Health States Grossman 9th Edition Test BankDocument8 pagesPorths Pathophysiology Concepts of Altered Health States Grossman 9th Edition Test BankDorothy Brissett100% (42)
- Health Policy Analysis ExampleDocument39 pagesHealth Policy Analysis Examplewilliamandre08100% (9)
- Evidence Based Practice: 5) Case Reports and Clinical ExamplesDocument11 pagesEvidence Based Practice: 5) Case Reports and Clinical ExamplesSahaj Yadav100% (6)
- Dr. Patrick J. Bryant Pharm.D. FSCIP, Dr. Heather A. Pace Pharm.D. - The Pharmacist's Guide To Evidence-Based Medicine For Clinical Decision Making-ASHP (2008) PDFDocument209 pagesDr. Patrick J. Bryant Pharm.D. FSCIP, Dr. Heather A. Pace Pharm.D. - The Pharmacist's Guide To Evidence-Based Medicine For Clinical Decision Making-ASHP (2008) PDFRaju Niraula100% (1)
- Clinical Decision Support Systems: Theory and PracticeFrom EverandClinical Decision Support Systems: Theory and PracticeRating: 2.5 out of 5 stars2.5/5 (1)
- Unhealthy Politics: The Battle over Evidence-Based MedicineFrom EverandUnhealthy Politics: The Battle over Evidence-Based MedicineRating: 4 out of 5 stars4/5 (1)
- Evidence-Based Psychotherapy: Advantages and Challenges: ReviewDocument9 pagesEvidence-Based Psychotherapy: Advantages and Challenges: ReviewJuan ParedesNo ratings yet
- MBE Controversias PDFDocument9 pagesMBE Controversias PDFAdriana M Rueda CastellanosNo ratings yet
- Rights To Social Determinants of Flourishing? A Paradigm For Disability and Public Health Research and PolicyDocument7 pagesRights To Social Determinants of Flourishing? A Paradigm For Disability and Public Health Research and Policymelicruz14No ratings yet
- Evidence Based Practive 2006Document15 pagesEvidence Based Practive 2006Bolo GanNo ratings yet
- Eip Gpe Eqc 2003 1Document24 pagesEip Gpe Eqc 2003 1rhuNo ratings yet
- Subject: Advanced Nursing Practice Evidence Based PracticeDocument7 pagesSubject: Advanced Nursing Practice Evidence Based PracticerinkuNo ratings yet
- Evidence Based Practice in Nursing BinuDocument51 pagesEvidence Based Practice in Nursing BinuBinu Joshva100% (3)
- 2013-Evidence Based Public HealthDocument15 pages2013-Evidence Based Public HealthEric Yesaya TanNo ratings yet
- MBE 2015 (Chapter)Document12 pagesMBE 2015 (Chapter)Anderson CarvalhoNo ratings yet
- ReprinttosendDocument7 pagesReprinttosendayatnapil193No ratings yet
- Research in Health and Social Care - EditedDocument8 pagesResearch in Health and Social Care - EditedJannat ButtNo ratings yet
- Practice Guidelines: Go ToDocument2 pagesPractice Guidelines: Go TokapilscribNo ratings yet
- Gesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Document15 pagesGesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Stavros TheodoridisNo ratings yet
- What Is Evidence PracticeDocument80 pagesWhat Is Evidence PracticeIndrajith LiyanageNo ratings yet
- Ebp 7Document7 pagesEbp 7way to satlokNo ratings yet
- Evidence Based Medicine Practice With Their Evolution and Application in Current Health SectorDocument5 pagesEvidence Based Medicine Practice With Their Evolution and Application in Current Health SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Primary Health Care Literature ReviewDocument4 pagesPrimary Health Care Literature Reviewafdtbluwq100% (1)
- Name:Matugue, Lorna Date: April 27, 2015 Yr/Sec:BSN-2B Score: Nursing Info-Lab Activity#1 Clinical Decision Support SystemDocument3 pagesName:Matugue, Lorna Date: April 27, 2015 Yr/Sec:BSN-2B Score: Nursing Info-Lab Activity#1 Clinical Decision Support SystemLorna MatugueNo ratings yet
- Articulo Trabajo 1Document13 pagesArticulo Trabajo 1NICOLAS OLAVE VINASCONo ratings yet
- MPH Question 2Document30 pagesMPH Question 2al azar bitNo ratings yet
- Public Health Education For Medical StudentsDocument20 pagesPublic Health Education For Medical StudentsOm AbdalrahmanNo ratings yet
- 2010 Evidence-Based Radiology Why and HowDocument16 pages2010 Evidence-Based Radiology Why and HowPeter Thaddeus RblsNo ratings yet
- s12961-018-0304-2Document15 pagess12961-018-0304-2LUISA FERNANDA OCHOA VILLEGASNo ratings yet
- Effectiveness of Manual Therapies: The UK Evidence ReportDocument40 pagesEffectiveness of Manual Therapies: The UK Evidence Reportapi-286958060No ratings yet
- Effectiveness of Manual Therapies The UKDocument33 pagesEffectiveness of Manual Therapies The UKSimao GigiNo ratings yet
- Best Practices For Mixed Methods ResearchDocument39 pagesBest Practices For Mixed Methods Researchscribd104444No ratings yet
- What Are The Ingredients For A Successful Evidence-Based Patient Choice Consultation?: A Qualitative StudyDocument14 pagesWhat Are The Ingredients For A Successful Evidence-Based Patient Choice Consultation?: A Qualitative StudyLourdes Fernandez CabreraNo ratings yet
- Scoping Review of Patient-Centered Careapproaches in HealthcareDocument9 pagesScoping Review of Patient-Centered Careapproaches in HealthcareLorena MunevarNo ratings yet
- Health Literacy QuestionnairDocument17 pagesHealth Literacy QuestionnairSafwan HadiNo ratings yet
- HS 4810 DF Unit 2Document5 pagesHS 4810 DF Unit 2Mathias NjoyaNo ratings yet
- Bronfort Report 2010 ChiropracticDocument33 pagesBronfort Report 2010 ChiropracticvicarofskepticNo ratings yet
- Physical Therapist As Critical InquirerDocument39 pagesPhysical Therapist As Critical InquirerMichels Garments S.H Nawaz Hosiery100% (1)
- Digital Drugs An Anatomy of New Medicines PDFDocument27 pagesDigital Drugs An Anatomy of New Medicines PDFshraddha5jNo ratings yet
- National Institute For Health and Clinical Excellence (NICE) : How Does It Work and What Are The Implications For The U.S.? (Executive Summary)Document8 pagesNational Institute For Health and Clinical Excellence (NICE) : How Does It Work and What Are The Implications For The U.S.? (Executive Summary)National Pharmaceutical CouncilNo ratings yet
- Sdi 5294 KumarDocument20 pagesSdi 5294 KumarBharatKumarMaheshwariNo ratings yet
- HealthSystemResearch DevelopmentDesignsandMethodsDocument6 pagesHealthSystemResearch DevelopmentDesignsandMethodsGesler Pilvan SainNo ratings yet
- 2019 Article 894Document12 pages2019 Article 894Elfina NataliaNo ratings yet
- 1-S2.0-S2590229620300149-Main PT 4Document11 pages1-S2.0-S2590229620300149-Main PT 4Ridania CahyanegaraNo ratings yet
- Economic Evaluation: A Reader's Guide To Studies of Cost-EffectivenessDocument12 pagesEconomic Evaluation: A Reader's Guide To Studies of Cost-Effectivenesskarthick pNo ratings yet
- Mr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaDocument6 pagesMr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaHariom RajputNo ratings yet
- Patient Safety Full ReportDocument40 pagesPatient Safety Full ReportYudi Ariesta Chandra100% (1)
- A Framework To Measure The Impact of Investments in Health ResearchDocument16 pagesA Framework To Measure The Impact of Investments in Health ResearchGesler Pilvan SainNo ratings yet
- Week1 NotesDocument21 pagesWeek1 NotesAlvia MagnoNo ratings yet
- NUR 816: Week1 NotesDocument21 pagesNUR 816: Week1 NotesAlvia MagnoNo ratings yet
- Evidence Based Medicine New ApprDocument15 pagesEvidence Based Medicine New ApprHalim SyahrilNo ratings yet
- AASLD Clinical Practice Guidelines: A Critical Review of Scientific Evidence and Evolving RecommendationsDocument11 pagesAASLD Clinical Practice Guidelines: A Critical Review of Scientific Evidence and Evolving RecommendationsManaswini SahuNo ratings yet
- Conjoint in HEALTH ResearchDocument17 pagesConjoint in HEALTH ResearchDiana Tan May KimNo ratings yet
- Personalized Medicine Support System: Resolving Conflict in Allocation To Risk Groups and Predicting Patient Molecular Response To Targeted TherapyDocument21 pagesPersonalized Medicine Support System: Resolving Conflict in Allocation To Risk Groups and Predicting Patient Molecular Response To Targeted TherapyhiijjournalNo ratings yet
- EBP in Adults FinalDocument20 pagesEBP in Adults FinalTony JacobNo ratings yet
- HealthSystemResearch DevelopmentDesignsandMethodsDocument6 pagesHealthSystemResearch DevelopmentDesignsandMethodsSani BaniaNo ratings yet
- Learning Objectives: Diane Romano-WoodwardDocument16 pagesLearning Objectives: Diane Romano-WoodwardFauzi FarhanNo ratings yet
- Week 1 1Document8 pagesWeek 1 1R-jeyn TorresNo ratings yet
- America's Healthcare Transformation: Strategies and InnovationsFrom EverandAmerica's Healthcare Transformation: Strategies and InnovationsNo ratings yet
- Ethical Diversity in Healthcare Delivery: Ethics in Healthcare & BeyondFrom EverandEthical Diversity in Healthcare Delivery: Ethics in Healthcare & BeyondNo ratings yet
- Critical Evaluation of Biomedical LiteraturesDocument33 pagesCritical Evaluation of Biomedical Literaturespragna novaNo ratings yet
- Natural Polymers: A Recent Review: World Journal of Pharmacy and Pharmaceutical SciencesDocument23 pagesNatural Polymers: A Recent Review: World Journal of Pharmacy and Pharmaceutical Sciencespragna novaNo ratings yet
- Gonorrhea: SymptomsDocument9 pagesGonorrhea: Symptomspragna novaNo ratings yet
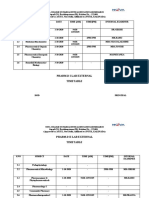
- Pharm.D I Lab External Timetable: Nova College of Pharmaceutical Education and Research)Document4 pagesPharm.D I Lab External Timetable: Nova College of Pharmaceutical Education and Research)pragna novaNo ratings yet
- DR - Pragna Pharm.d External Lab Question PapersDocument7 pagesDR - Pragna Pharm.d External Lab Question Paperspragna novaNo ratings yet
- (Spondilitis) : SpirometryDocument4 pages(Spondilitis) : Spirometrypragna novaNo ratings yet
- Dr. Pragna Pharm.d External Lab Question PapersDocument4 pagesDr. Pragna Pharm.d External Lab Question Paperspragna novaNo ratings yet
- August Month Report 20 To 31STDocument8 pagesAugust Month Report 20 To 31STpragna novaNo ratings yet
- Case StudiesDocument5 pagesCase Studiespragna novaNo ratings yet
- Fungal InfectionsDocument13 pagesFungal Infectionspragna novaNo ratings yet
- Causes: GastroenteritisDocument5 pagesCauses: Gastroenteritispragna novaNo ratings yet
- Risk Factors Include Having: Congenital Heart DefectsDocument3 pagesRisk Factors Include Having: Congenital Heart Defectspragna novaNo ratings yet
- Schematic Diagram Pathophysiology (Book-Based) COPD and TuberculosisDocument1 pageSchematic Diagram Pathophysiology (Book-Based) COPD and Tuberculosispragna novaNo ratings yet
- Gastroesophageal Reflux Disease: SymptomsDocument8 pagesGastroesophageal Reflux Disease: Symptomspragna novaNo ratings yet
- Asthma Diagnosis and TreatmentDocument7 pagesAsthma Diagnosis and Treatmentpragna novaNo ratings yet
- Symptoms: AnaemiaDocument11 pagesSymptoms: Anaemiapragna novaNo ratings yet
- Impetigo: Signs and SymptomsDocument3 pagesImpetigo: Signs and Symptomspragna novaNo ratings yet
- Pulmonary Function TestsDocument7 pagesPulmonary Function Testspragna novaNo ratings yet
- Scabies: Signs and SymptomsDocument8 pagesScabies: Signs and Symptomspragna novaNo ratings yet
- ECZEMADocument5 pagesECZEMApragna novaNo ratings yet
- Venous ThromboembolismDocument8 pagesVenous Thromboembolismpragna novaNo ratings yet
- ECZEMADocument5 pagesECZEMApragna novaNo ratings yet
- Peptic Ulcer DiseaseDocument8 pagesPeptic Ulcer Diseasepragna novaNo ratings yet
- Causes of Jaundice: Signs and SymptomsDocument9 pagesCauses of Jaundice: Signs and Symptomspragna novaNo ratings yet
- 2020 - 2022 Seminar ReflectionDocument17 pages2020 - 2022 Seminar Reflectionapi-529388510No ratings yet
- Delfinm QsenDocument57 pagesDelfinm Qsenapi-346220114No ratings yet
- Concurrence of Big Data Analytics and HealthcareDocument10 pagesConcurrence of Big Data Analytics and HealthcareShubham KimtaniNo ratings yet
- Welcome To The World of OBDocument25 pagesWelcome To The World of OBPratyum PradhanNo ratings yet
- Template Cobe Systematic ReviewDocument7 pagesTemplate Cobe Systematic ReviewLaryssa MylennaNo ratings yet
- In Service 2020 PrimerDocument6 pagesIn Service 2020 PrimerZaqueo Gutierrez FajardoNo ratings yet
- GCBH Cognitively Stimulating Activities ReportDocument27 pagesGCBH Cognitively Stimulating Activities ReportAnand SaaNo ratings yet
- Curriculum For Degree in Clinical PsychiatryDocument72 pagesCurriculum For Degree in Clinical PsychiatryEricBoamahNo ratings yet
- Nrs 305Document15 pagesNrs 305Michael AlutaNo ratings yet
- Clinical Practice Guidelines Einc 2014Document52 pagesClinical Practice Guidelines Einc 2014dennisreveni100% (1)
- Anaesthesiology in China Present and FutureDocument6 pagesAnaesthesiology in China Present and Futuremono011019No ratings yet
- Evidencebased Pharmacotherapy Optimal Patient Care Best Knowledge Competent PractitionerDocument171 pagesEvidencebased Pharmacotherapy Optimal Patient Care Best Knowledge Competent PractitionerTessa Amanda SavetriNo ratings yet
- Template For PHIL IRI Post TestDocument4 pagesTemplate For PHIL IRI Post TestAiza QuelangNo ratings yet
- Helen Aveyard 2010 Literature ReviewDocument5 pagesHelen Aveyard 2010 Literature Reviewc5qrve03100% (1)
- Ebp - 10 MCQS: Rimsha SadiqDocument2 pagesEbp - 10 MCQS: Rimsha SadiqZunaira100% (1)
- Sept 20 - Hbo Final Revision PDFDocument120 pagesSept 20 - Hbo Final Revision PDFjonna timonanNo ratings yet
- Develop and Implement Clinical Pathway PDFDocument10 pagesDevelop and Implement Clinical Pathway PDFAhmad Safi'i Bin SamirinNo ratings yet
- NP CompetenciesDocument84 pagesNP CompetenciesarbyjamesNo ratings yet
- An Introduction To Critical Appraisal: Training NotesDocument12 pagesAn Introduction To Critical Appraisal: Training NotesRima ZahraNo ratings yet
- Patient Acceptance For Computer Use in Outpatient DepartmentDocument9 pagesPatient Acceptance For Computer Use in Outpatient DepartmentEarl RomanosNo ratings yet
- Obesity Treatment Recommendations in The Philippines:Perspective On Their Utility and Implementation in Clinical PracticeDocument8 pagesObesity Treatment Recommendations in The Philippines:Perspective On Their Utility and Implementation in Clinical PracticeKaye Rioflorido ChingNo ratings yet
- Evidence Based PracticeDocument28 pagesEvidence Based PracticeSathish Rajamani100% (7)
- Review Article: Efficacy of Acupuncture in Reducing Preoperative Anxiety: A Meta-AnalysisDocument13 pagesReview Article: Efficacy of Acupuncture in Reducing Preoperative Anxiety: A Meta-AnalysisDyan TonyNo ratings yet
- Birth Preparedness and Complication Readiness - A Matrix of Shared ResponsibilitiesDocument7 pagesBirth Preparedness and Complication Readiness - A Matrix of Shared ResponsibilitiesAnil MishraNo ratings yet
- Malta SPFM Curriculum - MMCFD 2008 PDFDocument487 pagesMalta SPFM Curriculum - MMCFD 2008 PDFNicko RachmanioNo ratings yet