Download as pdf or txt
You might also like
- SHSB Health Contact DetailsDocument35 pagesSHSB Health Contact DetailsDharmendra Saw100% (2)
- CD Manual 09Document99 pagesCD Manual 09Matthew Ho100% (2)
- Effect of Oil Pulling On Plaque and Gingivitis PDFDocument8 pagesEffect of Oil Pulling On Plaque and Gingivitis PDFHerman WongNo ratings yet
- Oil Pulling As An Adjunct To Scaling and Root Planing: A Clinico-Microbial StudyDocument7 pagesOil Pulling As An Adjunct To Scaling and Root Planing: A Clinico-Microbial StudyinventionjournalsNo ratings yet
- Three MouthwashDocument12 pagesThree MouthwashrashmitanayakNo ratings yet
- Heliyon: Julian Woolley, Tatjana Gibbons, Kajal Patel, Roberto SaccoDocument7 pagesHeliyon: Julian Woolley, Tatjana Gibbons, Kajal Patel, Roberto SaccoArianneNo ratings yet
- Articulo CortelliDocument9 pagesArticulo CortelliDAVID ESTEBAN PAEZ URUEÑANo ratings yet
- Bestari 2017 J. Phys.: Conf. Ser. 884 012136Document9 pagesBestari 2017 J. Phys.: Conf. Ser. 884 012136ariipratiwiiNo ratings yet
- Aloe Vera MouthwashDocument6 pagesAloe Vera MouthwashGondoriyo PkmNo ratings yet
- The Effect of Coconut Oil Pulling On Streptococcus Mutans Count in Saliva in Comparison With Chlorhexidine MouthwashDocument4 pagesThe Effect of Coconut Oil Pulling On Streptococcus Mutans Count in Saliva in Comparison With Chlorhexidine MouthwashMelk SalesNo ratings yet
- Literature Review On MouthwashDocument4 pagesLiterature Review On Mouthwashfvfpvgph100% (1)
- MenakaDocument6 pagesMenakaTasha FarahNo ratings yet
- Totalcarequintessenceinternationalqi 43 7 E82 Cortelli 11-1Document14 pagesTotalcarequintessenceinternationalqi 43 7 E82 Cortelli 11-1DANIELA RINCÓN BELLONo ratings yet
- Review On Herbal Mouthwash For Management and Prevention of Oral DiseasesDocument9 pagesReview On Herbal Mouthwash For Management and Prevention of Oral DiseasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Kapoor2011Document5 pagesKapoor2011Tiara IkaNo ratings yet
- Oil Pulling and Its Oral Benefits-A Review: 2. Dr. N.Aravindha BabuDocument6 pagesOil Pulling and Its Oral Benefits-A Review: 2. Dr. N.Aravindha BabuTasha FarahNo ratings yet
- Effect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonDocument7 pagesEffect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonIndah LestariNo ratings yet
- Pre-Operative Antibiotics: Current and Future PracticesDocument5 pagesPre-Operative Antibiotics: Current and Future PracticesMariana PalaciosNo ratings yet
- The Effect of Listerine Mouthwash On Dental Plaque Gingival Inflammation and C Reactive Protein CRP 2161 1122.1000191Document5 pagesThe Effect of Listerine Mouthwash On Dental Plaque Gingival Inflammation and C Reactive Protein CRP 2161 1122.1000191Bagus RahmawanNo ratings yet
- Efficacy Test of A Toothpaste in Reducing Extrinsic Dental StainDocument7 pagesEfficacy Test of A Toothpaste in Reducing Extrinsic Dental StainJuwita Ratna IntanNo ratings yet
- Kandaswamy - Comparison of The Effectiveness of ProbioticDocument5 pagesKandaswamy - Comparison of The Effectiveness of ProbioticEls JastNo ratings yet
- The OIL PULLING GUIDE For ORAL HEALTH A How To Guide On Oil Pulling For Gum Health and Tooth Health (Susan Foster) (Z-Library)Document21 pagesThe OIL PULLING GUIDE For ORAL HEALTH A How To Guide On Oil Pulling For Gum Health and Tooth Health (Susan Foster) (Z-Library)Harshita ShivanagowdaNo ratings yet
- Kumar2017Document6 pagesKumar2017Andre KusoemoNo ratings yet
- TurmericDocument4 pagesTurmericEllizabeth LilantiNo ratings yet
- Comparative Evaluation of Chlorhexidine and Hydrogen Peroxide Mouth Wash Among Patients With GingivitisDocument5 pagesComparative Evaluation of Chlorhexidine and Hydrogen Peroxide Mouth Wash Among Patients With GingivitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mazhari2018 PDFDocument9 pagesMazhari2018 PDFKhaerani SaharNo ratings yet
- Article 4 AJOD SeptDocument5 pagesArticle 4 AJOD Septaakanksha bhardwajNo ratings yet
- Aloe Vera VS CHXDocument6 pagesAloe Vera VS CHXMai ThúyNo ratings yet
- 11th JC - SINDHUDocument22 pages11th JC - SINDHUDadi SindhuNo ratings yet
- Oil Pulling and Importance of Traditional Medicine in Oral Health MaintenanceDocument6 pagesOil Pulling and Importance of Traditional Medicine in Oral Health MaintenanceTasha FarahNo ratings yet
- Clinically Proven Herbal Toothpaste in Sri LankaDocument7 pagesClinically Proven Herbal Toothpaste in Sri LankaYoga ChanNo ratings yet
- s00784 019 03194 3Document9 pagess00784 019 03194 3shaikhwasif9597No ratings yet
- Effectiveness of A Desensitizing Agent Before In-Office Tooth Bleaching in Restored TeethDocument7 pagesEffectiveness of A Desensitizing Agent Before In-Office Tooth Bleaching in Restored TeethFer TorresNo ratings yet
- Oral HygieneDocument20 pagesOral HygieneMark NO A LA MinaNo ratings yet
- Comparative Effect of Neemstick and Toothbrush On Plaque Removal and Gingival Health - A Clinical TrialDocument6 pagesComparative Effect of Neemstick and Toothbrush On Plaque Removal and Gingival Health - A Clinical TrialnavinlewisNo ratings yet
- In Vivo Antiplaque Effect of Three Edible ToothpastesDocument5 pagesIn Vivo Antiplaque Effect of Three Edible ToothpasteslilingNo ratings yet
- Association Between Traditional Oral Hygiene Methods With Tooth Wear, Gingival Bleeding, and Recession: Descriptive Cross-Sectional StudyDocument4 pagesAssociation Between Traditional Oral Hygiene Methods With Tooth Wear, Gingival Bleeding, and Recession: Descriptive Cross-Sectional StudynavinlewisNo ratings yet
- Oil Pulling and Oral Health: A ReviewDocument5 pagesOil Pulling and Oral Health: A ReviewBabavNo ratings yet
- Herbal 2Document5 pagesHerbal 2Tasneem MostafaNo ratings yet
- 17-229-c FaltaDocument10 pages17-229-c FaltaElizabeth Vicencio AstudilloNo ratings yet
- Denture Cleansers: A ReviewDocument3 pagesDenture Cleansers: A ReviewInternational Organization of Scientific Research (IOSR)No ratings yet
- 0.2% ChlorhexidineDocument6 pages0.2% ChlorhexidineKrishan GuliaNo ratings yet
- Zheng-Yang Et Al 2016Document14 pagesZheng-Yang Et Al 2016karlajanileeNo ratings yet
- Effectiveness of An Essential Oil Mouthrinse in Improving Oral Health in Orthodontic PatientsDocument5 pagesEffectiveness of An Essential Oil Mouthrinse in Improving Oral Health in Orthodontic PatientsHamza GaaloulNo ratings yet
- Journal of Dentistry: A.M.L. Pedersen, M. Darwish, J. Nicholson, M.I. Edwards, A.K. Gupta, D. Belstrøm TDocument6 pagesJournal of Dentistry: A.M.L. Pedersen, M. Darwish, J. Nicholson, M.I. Edwards, A.K. Gupta, D. Belstrøm TVina NuranisyahNo ratings yet
- Bahan JurnalDocument6 pagesBahan JurnalDwi ApriyantiNo ratings yet
- Mouthwash The Use of Virgin Coconut Oil IIIDocument15 pagesMouthwash The Use of Virgin Coconut Oil IIIdominick binoyaNo ratings yet
- 2 AdultExpertsurveyJdentDocument13 pages2 AdultExpertsurveyJdentpepeNo ratings yet
- Dan Tik Anti StudyDocument4 pagesDan Tik Anti StudyJuwita Ratna IntanNo ratings yet
- 1852-4834-Aol-33-3-174 FINAL DR HARRYDocument7 pages1852-4834-Aol-33-3-174 FINAL DR HARRYMarco Antonio García LunaNo ratings yet
- Clinical Assessment of A Combination Lip TreatmentDocument6 pagesClinical Assessment of A Combination Lip TreatmentDummy CipawNo ratings yet
- An Oral Health Care Guideline For Institutionalised Older PeopleDocument5 pagesAn Oral Health Care Guideline For Institutionalised Older PeopleAvina Anin NasiaNo ratings yet
- Tikrit Journal For Dental Sciences 6 (2) (2018) 64-71Document8 pagesTikrit Journal For Dental Sciences 6 (2) (2018) 64-71Mudur AdamNo ratings yet
- Oral Hygiene in The Prevention of Periodontal DiseasesDocument20 pagesOral Hygiene in The Prevention of Periodontal DiseasesAlexandra BotezatNo ratings yet
- Erosion SalivaDocument8 pagesErosion SalivaEliza DNNo ratings yet
- Effect of Holy Basil in Mouthrinses On de Novo Plaque Formation in A Four Day Plaque Regrowth Model With Experimental GingivitisDocument3 pagesEffect of Holy Basil in Mouthrinses On de Novo Plaque Formation in A Four Day Plaque Regrowth Model With Experimental GingivitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- association_between_mouth_breathing_habit_and_dental_cariesa_retrospectiveDocument5 pagesassociation_between_mouth_breathing_habit_and_dental_cariesa_retrospectiveHaider AltahanNo ratings yet
- Effectiveness of A Miswak Extract Containing Toothpaste On Gingival Inflammation A Randomized Clinical TrialDocument8 pagesEffectiveness of A Miswak Extract Containing Toothpaste On Gingival Inflammation A Randomized Clinical TrialTahir AliNo ratings yet
- 7 DB 6Document6 pages7 DB 6AamirNo ratings yet
- 4 CHX Comparison BestDocument6 pages4 CHX Comparison BestWilliam LovellNo ratings yet
- How To Prevent BullyingDocument4 pagesHow To Prevent BullyingLiezel-jheng Apostol LozadaNo ratings yet
- CSQ Nap4 FullDocument219 pagesCSQ Nap4 FullJeisson FarroNo ratings yet
- Rabbit KeepingDocument12 pagesRabbit KeepingMoses NdwaruNo ratings yet
- ACE Personal Trainer Manual, 4 Edition - Ning PDFDocument112 pagesACE Personal Trainer Manual, 4 Edition - Ning PDFbasuthker raviNo ratings yet
- Fluid Therapy in Cardiac Surgery PatientsDocument37 pagesFluid Therapy in Cardiac Surgery PatientsaymxNo ratings yet
- Illuminating The Aura of Nostalgia: Perceptions of Time, Place, and Identity (ANASTASIA PLATOFF)Document33 pagesIlluminating The Aura of Nostalgia: Perceptions of Time, Place, and Identity (ANASTASIA PLATOFF)Anastasia PlatoffNo ratings yet
- FREE 8 Week Program For AthletesDocument13 pagesFREE 8 Week Program For AthletesHydra StortoNo ratings yet
- Thorax and Lungs Physical Assessment Includes InspectionDocument9 pagesThorax and Lungs Physical Assessment Includes InspectionwiwinNo ratings yet
- Hospital PharmacyDocument14 pagesHospital PharmacyAbigael PescasioNo ratings yet
- GIT InfectionDocument43 pagesGIT InfectionRaja RuzannaNo ratings yet
- Oxygen Therapy AdviceDocument38 pagesOxygen Therapy Advicenick_clayton_9No ratings yet
- Microbial PathogenesisDocument8 pagesMicrobial PathogenesisRachelleNo ratings yet
- Rehabilitation MedicaleDocument458 pagesRehabilitation MedicaleactoneNo ratings yet
- PacemakersDocument69 pagesPacemakersdocjeevan89100% (1)
- Anthropometry For ElderlyDocument20 pagesAnthropometry For ElderlyjarvantaraNo ratings yet
- Mindfulness: The Big IdeasDocument6 pagesMindfulness: The Big IdeasLuis AndradeNo ratings yet
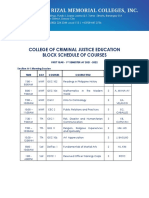
- College of Criminal Justice Education Block Schedule of CoursesDocument12 pagesCollege of Criminal Justice Education Block Schedule of CoursesKristel Ann ManlangitNo ratings yet
- A Review On Various Uses of N-Acetyl CysteineDocument7 pagesA Review On Various Uses of N-Acetyl CysteineMudrikaNo ratings yet
- Admission: Athia Fidian, M.PDDocument6 pagesAdmission: Athia Fidian, M.PDAthiaNo ratings yet
- Clamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)Document5 pagesClamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)rizwan900No ratings yet
- MSDS - X7 BlackDocument11 pagesMSDS - X7 BlackGrimmo1979No ratings yet
- Prosthodontic Perspective To All On - 4 ConceptDocument33 pagesProsthodontic Perspective To All On - 4 ConceptKrupali JainNo ratings yet
- Knauf - Insulation Godisnji Izvestaj PDFDocument29 pagesKnauf - Insulation Godisnji Izvestaj PDFDifermoNo ratings yet
- NewDocument17 pagesNewMadhu BalaNo ratings yet
- GDI 12 States FederalismDocument172 pagesGDI 12 States FederalismSupre ScrblNo ratings yet
- EthicsDocument10 pagesEthicsMadhubala JNo ratings yet
- Construction Site Management ChecklistDocument6 pagesConstruction Site Management ChecklistAbdulaziz IbrahimNo ratings yet
- The Effects of Trauma and How To Deal With It Jim BanksDocument5 pagesThe Effects of Trauma and How To Deal With It Jim Banks2bug2me2not2No ratings yet