Download as doc, pdf, or txt
You might also like
- RNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2Document4 pagesRNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2katrinasdNo ratings yet
- Physical Exam SheetDocument6 pagesPhysical Exam SheetDidi SaputraNo ratings yet
- PANCE Content BlueprintDocument5 pagesPANCE Content Blueprintalren258No ratings yet
- Gemp3 Paediatric Clinical Examination SkillsDocument13 pagesGemp3 Paediatric Clinical Examination SkillsAnna-Tammy HumanNo ratings yet
- Board II Review PDFDocument131 pagesBoard II Review PDFJohnNo ratings yet
- Family Medicine Haad ExamDocument727 pagesFamily Medicine Haad ExamAbdelnasir Abbas Abdalla ELsheikh89% (9)
- Review of Session 2003-2004Document246 pagesReview of Session 2003-2004The Royal Society of Edinburgh0% (1)
- Arterial DiseaseDocument57 pagesArterial DiseaseYil MosNo ratings yet
- WK 6 Study QsDocument7 pagesWK 6 Study Qsapi-479720222No ratings yet
- A Case of BreathlessnessDocument5 pagesA Case of BreathlessnesschuhuaNo ratings yet
- Preoperative AssessmentDocument2 pagesPreoperative AssessmentTom MallinsonNo ratings yet
- Post-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeDocument5 pagesPost-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeEben Ezar Dela CruzNo ratings yet
- Testicular ExamDocument3 pagesTesticular ExamminikatitingNo ratings yet
- Name: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionDocument46 pagesName: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionAbdirahman Abdillahi FarahNo ratings yet
- U World Endocrine FinalDocument12 pagesU World Endocrine Finalsean blazeNo ratings yet
- Screening and Early Detection: Epidemiological Basis For Disease Control - Fall 2001Document28 pagesScreening and Early Detection: Epidemiological Basis For Disease Control - Fall 2001Kharisma Rizqiah WahyuniNo ratings yet
- Basic Medical Wide QRS ArrhythmiaDocument39 pagesBasic Medical Wide QRS ArrhythmiaJee JunpyoNo ratings yet
- Common Signs and SymptomsDocument36 pagesCommon Signs and SymptomsJamil AimanNo ratings yet
- Medication Error 2017Document51 pagesMedication Error 2017Christina100% (1)
- CS Entire ScriptDocument31 pagesCS Entire ScriptSandeep SasidharanNo ratings yet
- Bundle Branch BlockDocument37 pagesBundle Branch BlocksyukronchalimNo ratings yet
- Warfarin Q and ADocument40 pagesWarfarin Q and AAbdul-Rhman Hamdy KishkNo ratings yet
- Thrombocytopenia Thrombocytopenia Thrombocytopenia ThrombocytopeniaDocument12 pagesThrombocytopenia Thrombocytopenia Thrombocytopenia ThrombocytopeniaRashed ShatnawiNo ratings yet
- Mul - Factorial Falls Risk Assessment: (Acute Hospital)Document2 pagesMul - Factorial Falls Risk Assessment: (Acute Hospital)eimear100% (1)
- SAQ MatrixDocument2 pagesSAQ MatrixThistell ThistleNo ratings yet
- Management of HypertensionDocument93 pagesManagement of Hypertensionhasibsb28No ratings yet
- CS Final PDFDocument46 pagesCS Final PDFOsteoprosis MyopathyNo ratings yet
- Usmle World Step 1 Pharmacology: Question ListDocument73 pagesUsmle World Step 1 Pharmacology: Question ListAnonymous 4txA8N8etNo ratings yet
- Perioperative Management of AnticoagulationDocument33 pagesPerioperative Management of Anticoagulationmonge20No ratings yet
- Endocrinology CasesDocument17 pagesEndocrinology CasesRoop SinghNo ratings yet
- Source NotesDocument30 pagesSource NotesChris Jardine Li100% (1)
- What Are The 4 Hormones With Disulfide Bonds?: Prolactin Insulin GH I Pig On BondsDocument782 pagesWhat Are The 4 Hormones With Disulfide Bonds?: Prolactin Insulin GH I Pig On BondsDrNatacha BarosyNo ratings yet
- Intravenous Fluid Therapy - Knowledge For Medical Students and PhysiciansDocument6 pagesIntravenous Fluid Therapy - Knowledge For Medical Students and PhysiciansNafiul IslamNo ratings yet
- Subject Sub-Subject Topic NameDocument6 pagesSubject Sub-Subject Topic NameHemanth Manikanta Sai PosaNo ratings yet
- Neuro Osce Cheat Sheet LolsDocument1 pageNeuro Osce Cheat Sheet LolsDjan Kurvie ValencerinaNo ratings yet
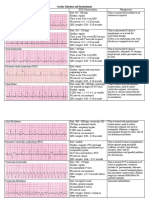
- Summary of ECG AbnormalitiesDocument7 pagesSummary of ECG AbnormalitiesKarin AdraiNo ratings yet
- MZ/MR A. I. First I'll Ask You Ii. Then I'll Do A Quick Iii. Then I'll Give You MyDocument6 pagesMZ/MR A. I. First I'll Ask You Ii. Then I'll Do A Quick Iii. Then I'll Give You Mykabal321No ratings yet
- Bio Chem 1Document5 pagesBio Chem 1Reynaldo RiveraNo ratings yet
- Pediatric Alterations in Cardiac Function: Congenital Heart Defects Laura M. Hernandez, DNP, Arnp NwcnhsDocument40 pagesPediatric Alterations in Cardiac Function: Congenital Heart Defects Laura M. Hernandez, DNP, Arnp Nwcnhsloita100% (1)
- PBL PgamboaDocument6 pagesPBL PgamboaLeanne Princess GamboaNo ratings yet
- USE THIS Exam Study Guide!!!!Document5 pagesUSE THIS Exam Study Guide!!!!daniel amosad lNo ratings yet
- 22 Disritmia 2018Document60 pages22 Disritmia 2018Nur akilaNo ratings yet
- Arteriolar Dilator Decreases After Load Ejection FractionDocument1 pageArteriolar Dilator Decreases After Load Ejection FractionJack GuccioneNo ratings yet
- Rectal Bleeding OverviewDocument7 pagesRectal Bleeding OverviewYanceHanzieNo ratings yet
- Sepsis 23-24Document45 pagesSepsis 23-24mcmillanb2No ratings yet
- Hepatitis A Virus: Incubation 1 - 6 MosDocument6 pagesHepatitis A Virus: Incubation 1 - 6 MosLiz Tollefson100% (1)
- Cardiac DysrhythmiasDocument3 pagesCardiac DysrhythmiasWilbert GuerreroNo ratings yet
- Pharmacology For Nurses: The Islamic UniversityDocument118 pagesPharmacology For Nurses: The Islamic UniversityRojina AdhikariNo ratings yet
- Wallenberg Syndrome: Publication DetailsDocument9 pagesWallenberg Syndrome: Publication DetailsHuang Jen Liang100% (1)
- Child Development and Milestones - Knowledge at AMBOSSDocument22 pagesChild Development and Milestones - Knowledge at AMBOSSJoseNo ratings yet
- Nbme 7 Block 2 Answerr+ExplanationsDocument24 pagesNbme 7 Block 2 Answerr+ExplanationsShauki AliNo ratings yet
- Kathynotes PDFDocument103 pagesKathynotes PDFvarrakeshNo ratings yet
- My Step 2 CK ExperienceDocument4 pagesMy Step 2 CK ExperienceshikaibNo ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- Step 2 Clinical Knowledge (CK) : Sample Test QuestionsDocument59 pagesStep 2 Clinical Knowledge (CK) : Sample Test QuestionsmarceloabadNo ratings yet
- ABCDE Management of A Critically Ill Patient: 1. Quickly Review CaseDocument2 pagesABCDE Management of A Critically Ill Patient: 1. Quickly Review CaseShannon RamsumairNo ratings yet
- The Disease Called DiabetesDocument71 pagesThe Disease Called Diabetesone_nd_onlyuNo ratings yet
- What Is Diabetes Mellitus?Document5 pagesWhat Is Diabetes Mellitus?Moħắmẻd ŘắắfatNo ratings yet
- The Perfect Guide To Understanding Diabetes: Monica Danforth BSC 1008 24 July 2011 Professor RiveroDocument17 pagesThe Perfect Guide To Understanding Diabetes: Monica Danforth BSC 1008 24 July 2011 Professor RiveroDan ZkyNo ratings yet
- Do I Have DiabetesDocument6 pagesDo I Have DiabetesSelim HanNo ratings yet
- Diabetes WfaDocument14 pagesDiabetes Wfaapi-611702624No ratings yet
- Information Sheet For CandidatesDocument4 pagesInformation Sheet For CandidatesjljoioiuNo ratings yet
- Information Sheet For CandidateDocument3 pagesInformation Sheet For CandidatejljoioiuNo ratings yet
- Information Sheet For CandidateDocument3 pagesInformation Sheet For CandidatejljoioiuNo ratings yet
- A45 GP T: H PE I: Yperthryroidism NervousnessDocument1 pageA45 GP T: H PE I: Yperthryroidism NervousnessjljoioiuNo ratings yet
- Myocardial InfarctionDocument1 pageMyocardial InfarctionjljoioiuNo ratings yet
- A Middle Aged Widow Apathetic AND Lethargic: YpothyroidismDocument1 pageA Middle Aged Widow Apathetic AND Lethargic: YpothyroidismjljoioiuNo ratings yet
- HypothyroidismDocument1 pageHypothyroidismjljoioiuNo ratings yet
- CholesteatomaDocument2 pagesCholesteatomajljoioiuNo ratings yet
- Drug Seeking BehaviourDocument1 pageDrug Seeking BehaviourjljoioiuNo ratings yet
- Contact Dermatitis: Ontact Ermatitis Ement PhotoDocument2 pagesContact Dermatitis: Ontact Ermatitis Ement PhotojljoioiuNo ratings yet
- Community Acquired PNEUMONIADocument4 pagesCommunity Acquired PNEUMONIAjljoioiuNo ratings yet
- DM Counseling New DXDocument3 pagesDM Counseling New DXjljoioiuNo ratings yet
- 70, - H 35 - H 2 - O N, L T: T: E G D - Develop A Self Management PlanDocument11 pages70, - H 35 - H 2 - O N, L T: T: E G D - Develop A Self Management PlanjljoioiuNo ratings yet
- Paeds Complete PDFDocument176 pagesPaeds Complete PDFjljoioiuNo ratings yet
- COMADocument1 pageCOMAjljoioiuNo ratings yet
- Some People Think That in Order To Prevent Illness and DiseaseDocument2 pagesSome People Think That in Order To Prevent Illness and DiseasejljoioiuNo ratings yet
- Congestive Cardiac FailuredDocument1 pageCongestive Cardiac FailuredjljoioiuNo ratings yet
- Band 8.0 Sample EssayDocument2 pagesBand 8.0 Sample EssayjljoioiuNo ratings yet
- Band 9.0 Model Essay 1Document2 pagesBand 9.0 Model Essay 1jljoioiuNo ratings yet
- MU MCQs Internal Medicine (2022)Document427 pagesMU MCQs Internal Medicine (2022)salar Vahid BagherniaNo ratings yet
- Hemat FPPP Questions and AnswersDocument18 pagesHemat FPPP Questions and AnswersDammy DebbyNo ratings yet
- Targocid Article 30 Referral Annex III - enDocument32 pagesTargocid Article 30 Referral Annex III - enDR JAMAL WARISNo ratings yet
- Polyarteritis NodosaDocument10 pagesPolyarteritis Nodosaaaron mbindyoNo ratings yet
- 5 Benefits and Uses of FrankincenseDocument2 pages5 Benefits and Uses of FrankincenseABDULKARIM HAJI YOUSUFNo ratings yet
- Homeo TipsDocument124 pagesHomeo TipsAditya uniyal100% (2)
- Diastolic Heart Failure Diagnosis and Therapy.12Document7 pagesDiastolic Heart Failure Diagnosis and Therapy.12enriquegarciagalianaNo ratings yet
- Chapter 2. Digestive System & Respiratory SystemDocument72 pagesChapter 2. Digestive System & Respiratory SystemFatiha AmiraNo ratings yet
- BIOC3364 - 2021 Lecture Notes AsthmaDocument26 pagesBIOC3364 - 2021 Lecture Notes AsthmachrystalNo ratings yet
- Module 5 - Intracerebral HemorrhageDocument29 pagesModule 5 - Intracerebral HemorrhageRick RanitNo ratings yet
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedNo ratings yet
- BP I Case StudyDocument29 pagesBP I Case StudyJoy-Rena Sabinay OchondraNo ratings yet
- Notes: Generally, What Are They?Document10 pagesNotes: Generally, What Are They?Yusril MarhaenNo ratings yet
- Endocrinology Lectures 1 3 DR - LigonDocument14 pagesEndocrinology Lectures 1 3 DR - LigonJealine Marie BernabeNo ratings yet
- All Questions With AnswersDocument940 pagesAll Questions With AnswersMaria Hernandez Martinez75% (4)
- Radiology Mission NEETDocument130 pagesRadiology Mission NEETShibdatta DasNo ratings yet
- Nd-Lesson-3 21 SynapsesDocument22 pagesNd-Lesson-3 21 Synapsesapi-176402481No ratings yet
- Complications of 3 Stage of LabourDocument17 pagesComplications of 3 Stage of LabourshravaniNo ratings yet
- Dr. Deri Rivano Pembimbing: Dr. Elsa Susanti. SP.SDocument25 pagesDr. Deri Rivano Pembimbing: Dr. Elsa Susanti. SP.Sderi rivanoNo ratings yet
- Unit SHC21 From The Level 2 Diploma in Health and Social Care Candidate HandbookDocument33 pagesUnit SHC21 From The Level 2 Diploma in Health and Social Care Candidate HandbookVaso Te AmargoNo ratings yet
- Monday MoussaDocument19 pagesMonday MoussaNational Press FoundationNo ratings yet
- Special SensesDocument5 pagesSpecial SensesggukNo ratings yet
- Chapter 8 Special SensesDocument5 pagesChapter 8 Special SensesEdralyn EgaelNo ratings yet
- NM Brosura ENG RED OldDocument29 pagesNM Brosura ENG RED OldDacan MiticNo ratings yet
- Red EyeDocument6 pagesRed EyeafatNo ratings yet
- 2007, Vol.25, Issues 3, DementiaDocument279 pages2007, Vol.25, Issues 3, Dementiajeaje100% (1)
- Dor LombarDocument27 pagesDor LombarLeonardoCampanelliNo ratings yet
- Appendex: VestigialityDocument14 pagesAppendex: VestigialitySher KhanNo ratings yet
- Biochemistry of Hormones: Dr. Rabia HussainDocument24 pagesBiochemistry of Hormones: Dr. Rabia HussainRabia HussainNo ratings yet