Download as pdf or txt
You might also like
- ASTM E1527 Downloaded 2014-04-14Document47 pagesASTM E1527 Downloaded 2014-04-14thescubatater100% (3)
- Assignment 2 MaterialsDocument2 pagesAssignment 2 Materialspoornima patil100% (1)
- Use of ForceDocument7 pagesUse of ForceNewsChannel 9100% (1)
- BS 05883 1996 (En)Document10 pagesBS 05883 1996 (En)Emanuele Mastrangelo100% (1)
- Kidney StonesDocument65 pagesKidney Stonesadhikarisamir100% (1)
- Urinary Tract StoneDocument17 pagesUrinary Tract StoneWilko WilliamNo ratings yet
- Stone Disease: (Brief Overview)Document54 pagesStone Disease: (Brief Overview)cafemedNo ratings yet
- Source: 20 Harrison's Principles of Internal Medicine: Nephrolithiasis/Kidney Stone DiseaseDocument8 pagesSource: 20 Harrison's Principles of Internal Medicine: Nephrolithiasis/Kidney Stone DiseaseMartin ClydeNo ratings yet
- Kidney Stones: BMJ (Online) July 2004Document6 pagesKidney Stones: BMJ (Online) July 2004Lina LopezNo ratings yet
- 1 Urinary StonesDocument11 pages1 Urinary StonesMohamed Al-zichrawyNo ratings yet
- Nephrolithiasis: Etiology, Stone Composition, Medical Management, and PreventionDocument28 pagesNephrolithiasis: Etiology, Stone Composition, Medical Management, and PreventionRuthra Devi NarayanasamyNo ratings yet
- Urinary LithiasisDocument35 pagesUrinary Lithiasishussain AltaherNo ratings yet
- Nephrolithiasis (K16) FinalDocument28 pagesNephrolithiasis (K16) FinalAndro Winardo SinagaNo ratings yet
- Stone Diseases (Brief Overview)Document54 pagesStone Diseases (Brief Overview)Rendra DananjayaNo ratings yet
- Batu Saluran Kemih Etio-Patogenesis PencegahanDocument43 pagesBatu Saluran Kemih Etio-Patogenesis Pencegahanikhlasia AmaliNo ratings yet
- Lifestyle Recommendations To Reduce The Risk of Kidney StonesDocument8 pagesLifestyle Recommendations To Reduce The Risk of Kidney Stonesjsali9210No ratings yet
- Surgery Urinary Lithiasis DR - HazimDocument8 pagesSurgery Urinary Lithiasis DR - Hazimhussain AltaherNo ratings yet
- Stone - Uro ClubDocument33 pagesStone - Uro Clubapoorva jainNo ratings yet
- Nephrolithiasis: Cynthia Denu-Ciocca, M.DDocument74 pagesNephrolithiasis: Cynthia Denu-Ciocca, M.DMA FTNo ratings yet
- Urinary Stones (Calculi)Document16 pagesUrinary Stones (Calculi)meedoasadelNo ratings yet
- Clinical UrologyDocument98 pagesClinical Urologythapan87100% (2)
- Nephrolithiasis: Incidence PathogenesisDocument7 pagesNephrolithiasis: Incidence PathogenesisNona Casey BaringNo ratings yet
- Chapter 38 UrolithiasisDocument20 pagesChapter 38 UrolithiasisKym DominguezNo ratings yet
- UROLITHIASISDocument9 pagesUROLITHIASISRimbun SidaurukNo ratings yet
- Batu GinjalDocument29 pagesBatu Ginjalarim100% (1)
- Medical Management of Renal Stone: Review ArticleDocument4 pagesMedical Management of Renal Stone: Review ArticlenaveenNo ratings yet
- Renal CalculiDocument49 pagesRenal CalculiDr. M. Prasad NaiduNo ratings yet
- Struvite (Consists of Uric Acid Cystine Xanthine Frequenc y Clinical RFDocument3 pagesStruvite (Consists of Uric Acid Cystine Xanthine Frequenc y Clinical RFAdnin ShereenNo ratings yet
- Urinary Stone DiseaseDocument11 pagesUrinary Stone DiseaseAdelia Maharani DNo ratings yet
- Preventive Kidney Stones: Continue Medical Education: Review ArticleDocument6 pagesPreventive Kidney Stones: Continue Medical Education: Review ArticleLusianaTasyaNo ratings yet
- L4 - Urolithiasis 1Document25 pagesL4 - Urolithiasis 1mhammednan2000No ratings yet
- The Management of UrolithiasisDocument9 pagesThe Management of UrolithiasiselhaanNo ratings yet
- Clinical Review: Kidney StonesDocument5 pagesClinical Review: Kidney StonesmrezasyahliNo ratings yet
- A Review On Kidney Stone and Its Herbal TreatmentDocument15 pagesA Review On Kidney Stone and Its Herbal TreatmentSabrina JonesNo ratings yet
- Stones in KidneyDocument7 pagesStones in Kidneygujji111No ratings yet
- Renal StonesDocument48 pagesRenal StonesLamiaa AliNo ratings yet
- Harrison StonesDocument9 pagesHarrison Stonesnova starNo ratings yet
- International Journal of Ayurveda and Pharma Research: Review ArticleDocument10 pagesInternational Journal of Ayurveda and Pharma Research: Review ArticleDrAnkur BorahNo ratings yet
- NephrolithiasisDocument56 pagesNephrolithiasisverdita100% (1)
- Dr. Bernard - Batu Ginjal (Urolithiasis)Document58 pagesDr. Bernard - Batu Ginjal (Urolithiasis)Ignatio Armando KenziNo ratings yet
- in Continuous Contact With Urine, The Calcium Phosphate Nidus Will Develop Into Calcium OxalateDocument4 pagesin Continuous Contact With Urine, The Calcium Phosphate Nidus Will Develop Into Calcium OxalatevaniaNo ratings yet
- Kidney StonesDocument65 pagesKidney StonesnazmiNo ratings yet
- Help Pedsurgeryafrica. 4Document4 pagesHelp Pedsurgeryafrica. 4Legina AromatikaNo ratings yet
- Kidney Stone PresenationDocument17 pagesKidney Stone PresenationNicole MandichNo ratings yet
- Roni Khoeroni Regi Septian Maruli Oloan TuaDocument72 pagesRoni Khoeroni Regi Septian Maruli Oloan TuaGiovan GaulNo ratings yet
- Developmental Disturbances in Mineral MetabolismDocument52 pagesDevelopmental Disturbances in Mineral MetabolismpriyaNo ratings yet
- Assessment of Kidney Stone and Prevalence of Its Chemical CompositionsDocument3 pagesAssessment of Kidney Stone and Prevalence of Its Chemical CompositionsAnjan khadkaNo ratings yet
- 3.1.3.2 Batu Saluran KemihDocument64 pages3.1.3.2 Batu Saluran Kemihwinda musliraNo ratings yet
- Hypercalcemia and Calcium Oxalate Urolithiasis in Cats: A Report of Five CasesDocument5 pagesHypercalcemia and Calcium Oxalate Urolithiasis in Cats: A Report of Five CasesJean AmorinNo ratings yet
- 5 Minute Biochemistry PresentationDocument23 pages5 Minute Biochemistry PresentationPITAGAN, Galda Boy 1-FNo ratings yet
- UROLITHIASISDocument25 pagesUROLITHIASISPaulo ManlangitNo ratings yet
- 02 Urothialisis - Prof. Doddy M SoebadiDocument27 pages02 Urothialisis - Prof. Doddy M Soebadirifqi13No ratings yet
- Urolithiasis: Philip M. Mshelbwala Hyacinth N. MbibuDocument4 pagesUrolithiasis: Philip M. Mshelbwala Hyacinth N. MbibuRatna Puspa RahayuNo ratings yet
- Urolithiasis: KSM Bedah Rsud Ciawi Kabupaten BogorDocument15 pagesUrolithiasis: KSM Bedah Rsud Ciawi Kabupaten BogorFilemon NyorapeNo ratings yet
- Renal Stones A Clinical Review PDFDocument6 pagesRenal Stones A Clinical Review PDFNurholis MajidNo ratings yet
- Urolithiasis and Its Causes-Short Review: T. Vijaya, M. Sathish Kumar, N. V. Ramarao, A. Naredra Babu, N. RamaraoDocument6 pagesUrolithiasis and Its Causes-Short Review: T. Vijaya, M. Sathish Kumar, N. V. Ramarao, A. Naredra Babu, N. RamaraoLea Bali Ulina SinurayaNo ratings yet
- Kidney Stones - A ReviewDocument18 pagesKidney Stones - A ReviewViall Ivenka100% (1)
- Urinary Tract CalculiDocument34 pagesUrinary Tract CalculiOnkar SinghNo ratings yet
- Renal and Genitourinary ConcernsDocument25 pagesRenal and Genitourinary ConcernsHerdy AdrianoNo ratings yet
- IntroductionDocument6 pagesIntroductionses_perez0412No ratings yet
- Notes on Diseases of Cattle: Cause, Symptoms and TreatmentFrom EverandNotes on Diseases of Cattle: Cause, Symptoms and TreatmentNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoNo ratings yet
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocument7 pagesDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoNo ratings yet
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoNo ratings yet
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (2)
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoNo ratings yet
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoNo ratings yet
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoNo ratings yet
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- Child PsychiatryDocument6 pagesChild PsychiatryVon HippoNo ratings yet
- Compilation of Platings in MicrobiologyDocument6 pagesCompilation of Platings in MicrobiologyVon HippoNo ratings yet
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoNo ratings yet
- Abdominal: Al HerniaDocument3 pagesAbdominal: Al HerniaVon Hippo100% (1)
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoNo ratings yet
- 1) Any Medical Student or GraduateDocument27 pages1) Any Medical Student or GraduateVon HippoNo ratings yet
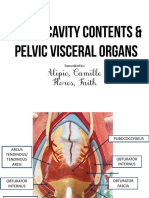
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoNo ratings yet
- Biochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Document14 pagesBiochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Von HippoNo ratings yet
- Book: - RecordingDocument8 pagesBook: - RecordingVon HippoNo ratings yet
- Fluid and Electrolytes YMDocument8 pagesFluid and Electrolytes YMVon HippoNo ratings yet
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoNo ratings yet
- 2013 Compiled para Exams and Shiftings PDFDocument27 pages2013 Compiled para Exams and Shiftings PDFVon HippoNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- Internal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoDocument3 pagesInternal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoVon HippoNo ratings yet
- MCQ Practice Test - Anatomy - 18 - 10 - 2020Document36 pagesMCQ Practice Test - Anatomy - 18 - 10 - 2020KhanNo ratings yet
- Hydrostatic Test ProcedureDocument3 pagesHydrostatic Test Proceduredep_vin100% (4)
- Behavioral Pathology in Alzheimers Disease Rating Scale Behavead 1997Document3 pagesBehavioral Pathology in Alzheimers Disease Rating Scale Behavead 1997Filly ZhangNo ratings yet
- Algae Final InteractiveDocument8 pagesAlgae Final InteractivesuziethefatcatNo ratings yet
- Fundamentals of Freestyle Wrestling v1Document3 pagesFundamentals of Freestyle Wrestling v1keynote76No ratings yet
- Penguin - Magnetic Drive Pump M SeiresDocument4 pagesPenguin - Magnetic Drive Pump M SeiresMiguel Angel LòpezNo ratings yet
- Air Pollution 4. Noise & Light PollutionDocument3 pagesAir Pollution 4. Noise & Light Pollutionclara olsenNo ratings yet
- General Description: Plug Fan ER..C With Standard MotorDocument7 pagesGeneral Description: Plug Fan ER..C With Standard MotorwildanNo ratings yet
- Off Load Tap Changer - Part 1Document20 pagesOff Load Tap Changer - Part 1Moncoz Aye100% (3)
- Quality Management Principles For Excellence: by - Sacchidanand Gogawale, Zen International SystemsDocument5 pagesQuality Management Principles For Excellence: by - Sacchidanand Gogawale, Zen International SystemsSanjeevani GogawaleNo ratings yet
- The Role of Public Health Leadership (2) FinalDocument20 pagesThe Role of Public Health Leadership (2) FinalKing Mugitah18No ratings yet
- Minutes of Meeting Sept 2, 2022Document11 pagesMinutes of Meeting Sept 2, 2022roseannurakNo ratings yet
- Caso #3Document2 pagesCaso #3Viviana Liz AlverioNo ratings yet
- C32400 PDFDocument76 pagesC32400 PDFjeffer rojasNo ratings yet
- 26 Jan 21Document156 pages26 Jan 21Aj YangNo ratings yet
- HIRA - COVID 19 Prevention and ControlsDocument17 pagesHIRA - COVID 19 Prevention and ControlsGyanendra Narayan NayakNo ratings yet
- Aecc 2 EnvsDocument12 pagesAecc 2 Envssaha7003810868No ratings yet
- 20T Wheat Flour Milling PlantDocument12 pages20T Wheat Flour Milling Plantshio29100% (2)
- Atlan A300 A300xl Pi 9107089 en MasterDocument12 pagesAtlan A300 A300xl Pi 9107089 en MasterHanh NguyenNo ratings yet
- Henry D. Solatorio JR.: A Reflection PaperDocument2 pagesHenry D. Solatorio JR.: A Reflection PaperCristoper BodionganNo ratings yet
- Document No. 13 - Oxygen ScavengersDocument3 pagesDocument No. 13 - Oxygen Scavengerssergio_perNo ratings yet
- Development of Affective Assess Ment ToolsDocument15 pagesDevelopment of Affective Assess Ment ToolsSpence EliverNo ratings yet
- Titration of Vinegar Lab ReportDocument8 pagesTitration of Vinegar Lab ReportIbrahim Abdulkadir JumaNo ratings yet
- Geography Chapter 7 Land SupplyDocument9 pagesGeography Chapter 7 Land SupplydenrabyNo ratings yet
- 19 20Document42 pages19 20Bharath ChandranNo ratings yet
- Ayelech EsheteDocument112 pagesAyelech EshetetemNo ratings yet