
SST I Guidelines
SST I Guidelines
You might also like
- Drug Formulary For Primates and Primate SanctuariesDocument20 pagesDrug Formulary For Primates and Primate SanctuariesMel Cid IIINo ratings yet
- Infections in Primary CareDocument5 pagesInfections in Primary CareAtta Muhammad Memon100% (1)
- SHC ABSSSI ED CDU GuidelineDocument4 pagesSHC ABSSSI ED CDU GuidelineHector Sanchez LacayoNo ratings yet
- Hpei PneumgdlnsDocument7 pagesHpei PneumgdlnsNurbayanti HermanNo ratings yet
- CNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Document1 pageCNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Fitri RachmadaniNo ratings yet
- IV To PO Poster VersionDocument1 pageIV To PO Poster VersionJohn Benedict Sta AnaNo ratings yet
- NAG Upper Respiratory Tract InfectionsDocument20 pagesNAG Upper Respiratory Tract InfectionsJun JimenezNo ratings yet
- Ckhs Empiric Antibiotic Guidance For Adult Pneumonia.2016Document3 pagesCkhs Empiric Antibiotic Guidance For Adult Pneumonia.2016surenvishvaNo ratings yet
- WFBMC Community Acquired Pneumonia (CAP) Treatment Guide For AdultsDocument2 pagesWFBMC Community Acquired Pneumonia (CAP) Treatment Guide For AdultsAlmas Safina KauserNo ratings yet
- Share Drugs of Choice To DiseasesDocument4 pagesShare Drugs of Choice To DiseasesDrkhanmianiNo ratings yet
- PCP Treatment GeneralDocument1 pagePCP Treatment GeneralLegolas gantengNo ratings yet
- Antibiotic Guidelines For AdultsDocument9 pagesAntibiotic Guidelines For AdultsVarshini Tamil SelvanNo ratings yet
- Infection of Ear, Nose, Throat, Skin and Skin Structure of GU TractDocument4 pagesInfection of Ear, Nose, Throat, Skin and Skin Structure of GU TractLide Arna CamposNo ratings yet
- Clinicalpath-Dfi Institutional Guideline FinalDocument6 pagesClinicalpath-Dfi Institutional Guideline Finalsu6233843No ratings yet
- Antibiotic Hospital ManDocument1 pageAntibiotic Hospital Manarshiya.manasekiNo ratings yet
- Treatment of Community Acquired PneumoniaDocument5 pagesTreatment of Community Acquired PneumoniaVarun R'MenonNo ratings yet
- Community Acquired Pneumonia in AdultsDocument5 pagesCommunity Acquired Pneumonia in AdultsEspie FerrerNo ratings yet
- Fournier's Gangrene GuidelinesDocument2 pagesFournier's Gangrene GuidelinesDavid Morales ZepedaNo ratings yet
- Ob Gyn AdultDocument3 pagesOb Gyn AdultHarshit RastogiNo ratings yet
- Infectious Disease, Pulmonology, and GI Study NotesDocument22 pagesInfectious Disease, Pulmonology, and GI Study NotesAlexis TranNo ratings yet
- Surgery Case Study Powerpoint - TalaDocument15 pagesSurgery Case Study Powerpoint - Talatqvhztcqb5No ratings yet
- Empiric Treatment Guidelines Common InfectionsDocument9 pagesEmpiric Treatment Guidelines Common InfectionsShiza Batool100% (1)
- Escalation Guide For Gram-Negative Bacteremia StanfordDocument3 pagesEscalation Guide For Gram-Negative Bacteremia StanfordLuis MedinaNo ratings yet
- Antibiotic Guidelines For PediatricsDocument33 pagesAntibiotic Guidelines For PediatricsVarshini Tamil SelvanNo ratings yet
- Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines For Sepsis Syndromes in AdultsDocument10 pagesHealth PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines For Sepsis Syndromes in AdultsFarmasi RSUD Kramat JatiNo ratings yet
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- Bone and Joint Infections BNHFT 2010 PDFDocument3 pagesBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriNo ratings yet
- Common Antibiotics Used in ObgDocument7 pagesCommon Antibiotics Used in ObgNur Aliah Amirah AmranNo ratings yet
- Final Antibiotics by ZaighamDocument35 pagesFinal Antibiotics by ZaighamMoazzam AliNo ratings yet
- L 44 Bendamustine 70 R CLLDocument7 pagesL 44 Bendamustine 70 R CLLsatishNo ratings yet
- 4.PE pdf correctedDocument17 pages4.PE pdf correctedjjclara003No ratings yet
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Document2 pagesPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikNo ratings yet
- Sepsis Antibiotics 2019 PDFDocument3 pagesSepsis Antibiotics 2019 PDFKobra CaktusNo ratings yet
- NAG Skin and Soft Tissue Infections AdultsDocument21 pagesNAG Skin and Soft Tissue Infections AdultsJun JimenezNo ratings yet
- MedicinesDocument6 pagesMedicinesMARJINA A. UDDAHNo ratings yet
- Antibiotic Pocket GuideDocument19 pagesAntibiotic Pocket GuideNaomi Liang100% (1)
- Skin and Soft Tissue Infections: CellulitisDocument9 pagesSkin and Soft Tissue Infections: Cellulitisgod4alllNo ratings yet
- Pharmacology Antibiotics Table FINALDocument3 pagesPharmacology Antibiotics Table FINALAndre AndreeaNo ratings yet
- Protocolos ATB MichiganDocument7 pagesProtocolos ATB MichiganDaniel Alejandro CastrilloNo ratings yet
- CPG Typhoid Fever 2017Document11 pagesCPG Typhoid Fever 2017Tam Adrian Aya-ayNo ratings yet
- Pneumonia ADULTDocument6 pagesPneumonia ADULTSebastian TjuwatjaNo ratings yet
- Med AtbDocument3 pagesMed AtbพัชรพลนะเออNo ratings yet
- Antibiotics PDFDocument4 pagesAntibiotics PDFNilamdeen Mohamed ZamilNo ratings yet
- CotriDocument2 pagesCotridenalynNo ratings yet
- Carboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Document8 pagesCarboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Olaru DianaNo ratings yet
- Camp General Servillano A Aquino, 2301 San Miguel, Tarlac CityDocument9 pagesCamp General Servillano A Aquino, 2301 San Miguel, Tarlac CityRuffa FriasNo ratings yet
- AntibioticsDocument13 pagesAntibioticsJOrgeNo ratings yet
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For Adultssee yinNo ratings yet
- PSMMC IV GUIDE LINES - Copy6Document18 pagesPSMMC IV GUIDE LINES - Copy6NhcpsNo ratings yet
- Obat UKMPPDDocument54 pagesObat UKMPPDMuh.ikhsan zainalNo ratings yet
- Lampiran OM & FaringitisDocument6 pagesLampiran OM & FaringitisAdhinyDistiHelmiNo ratings yet
- Ministry Health Medicines Formulary 1 2015Document371 pagesMinistry Health Medicines Formulary 1 2015David Lim Su ShenNo ratings yet
- MAPPING PINERE 6, Jumat 3 Sep 2021Document5 pagesMAPPING PINERE 6, Jumat 3 Sep 2021Rina SyafritaNo ratings yet
- Antibiotik: Generik Nama Paten Indikasi Dosis Bumil As. Clavulanat + AmoxycillinDocument8 pagesAntibiotik: Generik Nama Paten Indikasi Dosis Bumil As. Clavulanat + AmoxycillinVeve PujiNo ratings yet
- Ciprobay PIDocument26 pagesCiprobay PIfsdfNo ratings yet
- Navora OB WARD DRUG STUDYDocument7 pagesNavora OB WARD DRUG STUDYNavora, Bryle TrixthaneNo ratings yet
- Antibiotic Choices For Treatment of MRSADocument16 pagesAntibiotic Choices For Treatment of MRSAfarmasi_hm100% (2)
- Indications For CT Brain or Neck in Head InjuriesDocument4 pagesIndications For CT Brain or Neck in Head InjuriesMehrine MehrNo ratings yet
- Ortho 2Document13 pagesOrtho 2Mehrine MehrNo ratings yet
- Open Nephrolithotomy and Open Pyelolithotomy: A GuideDocument6 pagesOpen Nephrolithotomy and Open Pyelolithotomy: A GuideMehrine MehrNo ratings yet
- Hematoma Small Artery RuptureDocument7 pagesHematoma Small Artery RuptureMehrine MehrNo ratings yet
- Topical Preparation Counselling Guide Pharmacist Ed1.2018 01.08.2019Document49 pagesTopical Preparation Counselling Guide Pharmacist Ed1.2018 01.08.2019Mehrine MehrNo ratings yet
- Set3 PDFDocument36 pagesSet3 PDFvishwas100% (1)
- Astrological Study of Infertility - ConclusionDocument9 pagesAstrological Study of Infertility - ConclusionAnamika SNo ratings yet
- Edl What Is A TestDocument18 pagesEdl What Is A TestEric Tipton100% (1)
- Loctite 270 Eng MsdsDocument16 pagesLoctite 270 Eng Msdstimeforever aymenNo ratings yet
- Focus Level 3 Table of Contents PDFDocument2 pagesFocus Level 3 Table of Contents PDFDaria KudosLamNo ratings yet
- The Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocDocument43 pagesThe Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocKenberly DingleNo ratings yet
- Three Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphDocument10 pagesThree Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphLuluk NafisahNo ratings yet
- How To Find Inner PeaceDocument5 pagesHow To Find Inner Peacedivya shindeNo ratings yet
- Mass. Proposed AddendumsDocument25 pagesMass. Proposed AddendumsKirk HartleyNo ratings yet
- Master Circular 16 Compassionate GroundDocument13 pagesMaster Circular 16 Compassionate GroundSHANMUGA VADIVEL SUNDARARAJANNo ratings yet
- Coitus ReservatusDocument4 pagesCoitus ReservatusTrà Thanh NguyễnNo ratings yet
- Mnemonics For Block 3Document3 pagesMnemonics For Block 3sahana2791No ratings yet
- Joy Trust Fear Surprise Sadness Disgust Anger AnticipationDocument4 pagesJoy Trust Fear Surprise Sadness Disgust Anger AnticipationsatyakaamsNo ratings yet
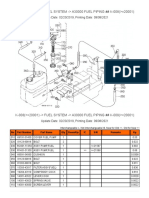
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Technical Data Sheet TGZ190 Rev-1.pdf (Read Only)Document2 pagesTechnical Data Sheet TGZ190 Rev-1.pdf (Read Only)Fatiga jrNo ratings yet
- Module 2 Project Gap Analysis Strategy For Team #3Document20 pagesModule 2 Project Gap Analysis Strategy For Team #3Mary A. Dillard100% (2)
- Hunna I. Lipke v. City of New York, Et Al.Document21 pagesHunna I. Lipke v. City of New York, Et Al.Eric SandersNo ratings yet
- Pathfit 2Document18 pagesPathfit 2Pam LlanetaNo ratings yet
- 10 Transport in Plants Neet Biology Model Question PaperDocument5 pages10 Transport in Plants Neet Biology Model Question PaperJosephNo ratings yet
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (4)
- 2022 Children's ReportDocument3 pages2022 Children's ReportMSWD Camiling100% (2)
- Creep and Shrinkage in ConcreteDocument18 pagesCreep and Shrinkage in Concretesarthakpuri21No ratings yet
- Chapter 1Document26 pagesChapter 1Reigner Jay B. Escartin100% (1)
- Bacteria ProfileDocument18 pagesBacteria ProfileNOR-FATIMAH BARATNo ratings yet
- Methods of Measuring Plaque PH: Assignment in CariologyDocument6 pagesMethods of Measuring Plaque PH: Assignment in Cariologydr_shakir-sudanNo ratings yet
- Peugeot 607 Owners Manual 2005Document206 pagesPeugeot 607 Owners Manual 2005AndreiNo ratings yet
- Focaccia Bread: IngredientsDocument3 pagesFocaccia Bread: IngredientsJack WillisNo ratings yet
- What Are The Expected Tasks You Have Successfully AccomplishedDocument1 pageWhat Are The Expected Tasks You Have Successfully AccomplishedImmortality Realm67% (18)
- Embedded Controlled Drip Irrigation SystemDocument5 pagesEmbedded Controlled Drip Irrigation SystemInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet




















































































Download as pdf or txt
You might also like
- Drug Formulary For Primates and Primate SanctuariesDocument20 pagesDrug Formulary For Primates and Primate SanctuariesMel Cid IIINo ratings yet
- Infections in Primary CareDocument5 pagesInfections in Primary CareAtta Muhammad Memon100% (1)
- SHC ABSSSI ED CDU GuidelineDocument4 pagesSHC ABSSSI ED CDU GuidelineHector Sanchez LacayoNo ratings yet
- Hpei PneumgdlnsDocument7 pagesHpei PneumgdlnsNurbayanti HermanNo ratings yet
- CNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Document1 pageCNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Fitri RachmadaniNo ratings yet
- IV To PO Poster VersionDocument1 pageIV To PO Poster VersionJohn Benedict Sta AnaNo ratings yet
- NAG Upper Respiratory Tract InfectionsDocument20 pagesNAG Upper Respiratory Tract InfectionsJun JimenezNo ratings yet
- Ckhs Empiric Antibiotic Guidance For Adult Pneumonia.2016Document3 pagesCkhs Empiric Antibiotic Guidance For Adult Pneumonia.2016surenvishvaNo ratings yet
- WFBMC Community Acquired Pneumonia (CAP) Treatment Guide For AdultsDocument2 pagesWFBMC Community Acquired Pneumonia (CAP) Treatment Guide For AdultsAlmas Safina KauserNo ratings yet
- Share Drugs of Choice To DiseasesDocument4 pagesShare Drugs of Choice To DiseasesDrkhanmianiNo ratings yet
- PCP Treatment GeneralDocument1 pagePCP Treatment GeneralLegolas gantengNo ratings yet
- Antibiotic Guidelines For AdultsDocument9 pagesAntibiotic Guidelines For AdultsVarshini Tamil SelvanNo ratings yet
- Infection of Ear, Nose, Throat, Skin and Skin Structure of GU TractDocument4 pagesInfection of Ear, Nose, Throat, Skin and Skin Structure of GU TractLide Arna CamposNo ratings yet
- Clinicalpath-Dfi Institutional Guideline FinalDocument6 pagesClinicalpath-Dfi Institutional Guideline Finalsu6233843No ratings yet
- Antibiotic Hospital ManDocument1 pageAntibiotic Hospital Manarshiya.manasekiNo ratings yet
- Treatment of Community Acquired PneumoniaDocument5 pagesTreatment of Community Acquired PneumoniaVarun R'MenonNo ratings yet
- Community Acquired Pneumonia in AdultsDocument5 pagesCommunity Acquired Pneumonia in AdultsEspie FerrerNo ratings yet
- Fournier's Gangrene GuidelinesDocument2 pagesFournier's Gangrene GuidelinesDavid Morales ZepedaNo ratings yet
- Ob Gyn AdultDocument3 pagesOb Gyn AdultHarshit RastogiNo ratings yet
- Infectious Disease, Pulmonology, and GI Study NotesDocument22 pagesInfectious Disease, Pulmonology, and GI Study NotesAlexis TranNo ratings yet
- Surgery Case Study Powerpoint - TalaDocument15 pagesSurgery Case Study Powerpoint - Talatqvhztcqb5No ratings yet
- Empiric Treatment Guidelines Common InfectionsDocument9 pagesEmpiric Treatment Guidelines Common InfectionsShiza Batool100% (1)
- Escalation Guide For Gram-Negative Bacteremia StanfordDocument3 pagesEscalation Guide For Gram-Negative Bacteremia StanfordLuis MedinaNo ratings yet
- Antibiotic Guidelines For PediatricsDocument33 pagesAntibiotic Guidelines For PediatricsVarshini Tamil SelvanNo ratings yet
- Health PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines For Sepsis Syndromes in AdultsDocument10 pagesHealth PEI: Provincial Antibiotic Advisory Team Empiric Antibiotic Treatment Guidelines For Sepsis Syndromes in AdultsFarmasi RSUD Kramat JatiNo ratings yet
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- Bone and Joint Infections BNHFT 2010 PDFDocument3 pagesBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriNo ratings yet
- Common Antibiotics Used in ObgDocument7 pagesCommon Antibiotics Used in ObgNur Aliah Amirah AmranNo ratings yet
- Final Antibiotics by ZaighamDocument35 pagesFinal Antibiotics by ZaighamMoazzam AliNo ratings yet
- L 44 Bendamustine 70 R CLLDocument7 pagesL 44 Bendamustine 70 R CLLsatishNo ratings yet
- 4.PE pdf correctedDocument17 pages4.PE pdf correctedjjclara003No ratings yet
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Document2 pagesPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikNo ratings yet
- Sepsis Antibiotics 2019 PDFDocument3 pagesSepsis Antibiotics 2019 PDFKobra CaktusNo ratings yet
- NAG Skin and Soft Tissue Infections AdultsDocument21 pagesNAG Skin and Soft Tissue Infections AdultsJun JimenezNo ratings yet
- MedicinesDocument6 pagesMedicinesMARJINA A. UDDAHNo ratings yet
- Antibiotic Pocket GuideDocument19 pagesAntibiotic Pocket GuideNaomi Liang100% (1)
- Skin and Soft Tissue Infections: CellulitisDocument9 pagesSkin and Soft Tissue Infections: Cellulitisgod4alllNo ratings yet
- Pharmacology Antibiotics Table FINALDocument3 pagesPharmacology Antibiotics Table FINALAndre AndreeaNo ratings yet
- Protocolos ATB MichiganDocument7 pagesProtocolos ATB MichiganDaniel Alejandro CastrilloNo ratings yet
- CPG Typhoid Fever 2017Document11 pagesCPG Typhoid Fever 2017Tam Adrian Aya-ayNo ratings yet
- Pneumonia ADULTDocument6 pagesPneumonia ADULTSebastian TjuwatjaNo ratings yet
- Med AtbDocument3 pagesMed AtbพัชรพลนะเออNo ratings yet
- Antibiotics PDFDocument4 pagesAntibiotics PDFNilamdeen Mohamed ZamilNo ratings yet
- CotriDocument2 pagesCotridenalynNo ratings yet
- Carboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Document8 pagesCarboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Olaru DianaNo ratings yet
- Camp General Servillano A Aquino, 2301 San Miguel, Tarlac CityDocument9 pagesCamp General Servillano A Aquino, 2301 San Miguel, Tarlac CityRuffa FriasNo ratings yet
- AntibioticsDocument13 pagesAntibioticsJOrgeNo ratings yet
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For Adultssee yinNo ratings yet
- PSMMC IV GUIDE LINES - Copy6Document18 pagesPSMMC IV GUIDE LINES - Copy6NhcpsNo ratings yet
- Obat UKMPPDDocument54 pagesObat UKMPPDMuh.ikhsan zainalNo ratings yet
- Lampiran OM & FaringitisDocument6 pagesLampiran OM & FaringitisAdhinyDistiHelmiNo ratings yet
- Ministry Health Medicines Formulary 1 2015Document371 pagesMinistry Health Medicines Formulary 1 2015David Lim Su ShenNo ratings yet
- MAPPING PINERE 6, Jumat 3 Sep 2021Document5 pagesMAPPING PINERE 6, Jumat 3 Sep 2021Rina SyafritaNo ratings yet
- Antibiotik: Generik Nama Paten Indikasi Dosis Bumil As. Clavulanat + AmoxycillinDocument8 pagesAntibiotik: Generik Nama Paten Indikasi Dosis Bumil As. Clavulanat + AmoxycillinVeve PujiNo ratings yet
- Ciprobay PIDocument26 pagesCiprobay PIfsdfNo ratings yet
- Navora OB WARD DRUG STUDYDocument7 pagesNavora OB WARD DRUG STUDYNavora, Bryle TrixthaneNo ratings yet
- Antibiotic Choices For Treatment of MRSADocument16 pagesAntibiotic Choices For Treatment of MRSAfarmasi_hm100% (2)
- Indications For CT Brain or Neck in Head InjuriesDocument4 pagesIndications For CT Brain or Neck in Head InjuriesMehrine MehrNo ratings yet
- Ortho 2Document13 pagesOrtho 2Mehrine MehrNo ratings yet
- Open Nephrolithotomy and Open Pyelolithotomy: A GuideDocument6 pagesOpen Nephrolithotomy and Open Pyelolithotomy: A GuideMehrine MehrNo ratings yet
- Hematoma Small Artery RuptureDocument7 pagesHematoma Small Artery RuptureMehrine MehrNo ratings yet
- Topical Preparation Counselling Guide Pharmacist Ed1.2018 01.08.2019Document49 pagesTopical Preparation Counselling Guide Pharmacist Ed1.2018 01.08.2019Mehrine MehrNo ratings yet
- Set3 PDFDocument36 pagesSet3 PDFvishwas100% (1)
- Astrological Study of Infertility - ConclusionDocument9 pagesAstrological Study of Infertility - ConclusionAnamika SNo ratings yet
- Edl What Is A TestDocument18 pagesEdl What Is A TestEric Tipton100% (1)
- Loctite 270 Eng MsdsDocument16 pagesLoctite 270 Eng Msdstimeforever aymenNo ratings yet
- Focus Level 3 Table of Contents PDFDocument2 pagesFocus Level 3 Table of Contents PDFDaria KudosLamNo ratings yet
- The Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocDocument43 pagesThe Internet Addiction and The Academic Productivity of Grade 12 Students in Aclc OrmocKenberly DingleNo ratings yet
- Three Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphDocument10 pagesThree Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphLuluk NafisahNo ratings yet
- How To Find Inner PeaceDocument5 pagesHow To Find Inner Peacedivya shindeNo ratings yet
- Mass. Proposed AddendumsDocument25 pagesMass. Proposed AddendumsKirk HartleyNo ratings yet
- Master Circular 16 Compassionate GroundDocument13 pagesMaster Circular 16 Compassionate GroundSHANMUGA VADIVEL SUNDARARAJANNo ratings yet
- Coitus ReservatusDocument4 pagesCoitus ReservatusTrà Thanh NguyễnNo ratings yet
- Mnemonics For Block 3Document3 pagesMnemonics For Block 3sahana2791No ratings yet
- Joy Trust Fear Surprise Sadness Disgust Anger AnticipationDocument4 pagesJoy Trust Fear Surprise Sadness Disgust Anger AnticipationsatyakaamsNo ratings yet
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Technical Data Sheet TGZ190 Rev-1.pdf (Read Only)Document2 pagesTechnical Data Sheet TGZ190 Rev-1.pdf (Read Only)Fatiga jrNo ratings yet
- Module 2 Project Gap Analysis Strategy For Team #3Document20 pagesModule 2 Project Gap Analysis Strategy For Team #3Mary A. Dillard100% (2)
- Hunna I. Lipke v. City of New York, Et Al.Document21 pagesHunna I. Lipke v. City of New York, Et Al.Eric SandersNo ratings yet
- Pathfit 2Document18 pagesPathfit 2Pam LlanetaNo ratings yet
- 10 Transport in Plants Neet Biology Model Question PaperDocument5 pages10 Transport in Plants Neet Biology Model Question PaperJosephNo ratings yet
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (4)
- 2022 Children's ReportDocument3 pages2022 Children's ReportMSWD Camiling100% (2)
- Creep and Shrinkage in ConcreteDocument18 pagesCreep and Shrinkage in Concretesarthakpuri21No ratings yet
- Chapter 1Document26 pagesChapter 1Reigner Jay B. Escartin100% (1)
- Bacteria ProfileDocument18 pagesBacteria ProfileNOR-FATIMAH BARATNo ratings yet
- Methods of Measuring Plaque PH: Assignment in CariologyDocument6 pagesMethods of Measuring Plaque PH: Assignment in Cariologydr_shakir-sudanNo ratings yet
- Peugeot 607 Owners Manual 2005Document206 pagesPeugeot 607 Owners Manual 2005AndreiNo ratings yet
- Focaccia Bread: IngredientsDocument3 pagesFocaccia Bread: IngredientsJack WillisNo ratings yet
- What Are The Expected Tasks You Have Successfully AccomplishedDocument1 pageWhat Are The Expected Tasks You Have Successfully AccomplishedImmortality Realm67% (18)
- Embedded Controlled Drip Irrigation SystemDocument5 pagesEmbedded Controlled Drip Irrigation SystemInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet