
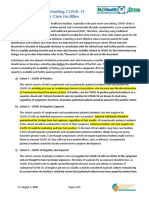
Planning For A Psychiatric COVID-19-Positive Unit
Planning For A Psychiatric COVID-19-Positive Unit
You might also like
- Quantitative Methods For Business 13th Edition Anderson Solutions ManualDocument14 pagesQuantitative Methods For Business 13th Edition Anderson Solutions ManualMicheleWallsertso100% (16)
- A Guide For Departments of Anaesthesia, Critical Care and Pain ManagementDocument57 pagesA Guide For Departments of Anaesthesia, Critical Care and Pain ManagementIrene Cristina100% (2)
- Tongue Tie: From Confusion To Clarity-A ReviewDocument4 pagesTongue Tie: From Confusion To Clarity-A Reviewrahmaputra100% (1)
- Local Resumption of Elective Surgery GuidanceDocument10 pagesLocal Resumption of Elective Surgery Guidancevjgg810199No ratings yet
- Manejo Ambulatorio AdultosDocument18 pagesManejo Ambulatorio AdultosCarlos Huaman ZevallosNo ratings yet
- AssignmentDocument5 pagesAssignmentClaire ChiuNo ratings yet
- Pulmonary Rehabilitation For COVID-19 PatientsDocument16 pagesPulmonary Rehabilitation For COVID-19 Patientspufu crisanNo ratings yet
- COVID 19 Physicians GuideDocument4 pagesCOVID 19 Physicians GuidenilrmNo ratings yet
- Covid 19 ProgramDocument12 pagesCovid 19 ProgramBAGUIO CATSNo ratings yet
- Resp Follow Up Guidance Post Covid PneumoniaDocument15 pagesResp Follow Up Guidance Post Covid PneumoniaAnindam SahaNo ratings yet
- Community Quarantine RecommendationsDocument5 pagesCommunity Quarantine RecommendationsRapplerNo ratings yet
- Joint Statement Resuming Elective Surgery After COVID19Document4 pagesJoint Statement Resuming Elective Surgery After COVID19vjgg810199No ratings yet
- Covid-19: Guide On Home-Based Care, Screening & Isolation Ward Set UpDocument9 pagesCovid-19: Guide On Home-Based Care, Screening & Isolation Ward Set Upvimalraj vtNo ratings yet
- Infection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsDocument20 pagesInfection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsMatthew DavisNo ratings yet
- Covid Flexibility Reopen Essential Non Covid ServicesDocument3 pagesCovid Flexibility Reopen Essential Non Covid ServicesDaniel RusseNo ratings yet
- Office of The Secretary: Temporary TreatmentDocument14 pagesOffice of The Secretary: Temporary TreatmentBenjamin Karlo Delos SantosNo ratings yet
- Clinical Guidance For Managing Suspected COVID 19 Patients in ICRC Supported Hospitals 05.04.2020 - FianlDocument7 pagesClinical Guidance For Managing Suspected COVID 19 Patients in ICRC Supported Hospitals 05.04.2020 - FianlCrys TahNo ratings yet
- Guideline For Conservation of Respiratory Protection ResourcesDocument14 pagesGuideline For Conservation of Respiratory Protection ResourcesAMEU URGENCIASNo ratings yet
- COVID19 IPCProtocolSurgicalProceduresAdultDocument16 pagesCOVID19 IPCProtocolSurgicalProceduresAdultwatimelawatiNo ratings yet
- Preparing Your Intensive Care Unit For The COVID - ASLIDocument24 pagesPreparing Your Intensive Care Unit For The COVID - ASLIEven EdomekoNo ratings yet
- Covid Cohorting PacDocument5 pagesCovid Cohorting PacsimplyrosalynNo ratings yet
- COVID 19 Outpatient DialysisDocument5 pagesCOVID 19 Outpatient DialysisTheala RadistaNo ratings yet
- AdultCriticalCare COVID 19 October2020Document21 pagesAdultCriticalCare COVID 19 October2020Maria Josefina RaffinNo ratings yet
- Guidance For Routine Immunization Services During COVID-19: - PageDocument14 pagesGuidance For Routine Immunization Services During COVID-19: - PagePrisma CahyaNo ratings yet
- Privateroom JournalDocument5 pagesPrivateroom JournalNathaniel PulidoNo ratings yet
- Importance of Healthcare in Covid TimeDocument4 pagesImportance of Healthcare in Covid TimeEditor IJTSRDNo ratings yet
- COVID 19 Antigen Testing GuidelinesDocument12 pagesCOVID 19 Antigen Testing GuidelinesStephanie SánchezNo ratings yet
- prehospital-EMS-COVID-19-recommendations - 4.4Document19 pagesprehospital-EMS-COVID-19-recommendations - 4.4MEONENo ratings yet
- Neurologic Emergencies During The Coronavirus DiseDocument17 pagesNeurologic Emergencies During The Coronavirus DiseCristina CalzadaNo ratings yet
- C0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchDocument4 pagesC0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchKevo VillagranNo ratings yet
- Teknik Resus BosaertDocument13 pagesTeknik Resus BosaertDADASDSANo ratings yet
- Diagnosis and Management of Community-Acquired Pneumonia: Evidence-Based PracticeDocument11 pagesDiagnosis and Management of Community-Acquired Pneumonia: Evidence-Based PracticeMega Julia ThioNo ratings yet
- Hemodialysis Unit Preparedness COVID-19 Pandemic: During and AfterDocument8 pagesHemodialysis Unit Preparedness COVID-19 Pandemic: During and Afteryanuar esthoNo ratings yet
- Kathleen E. Toomey, M.D., M.P.HDocument3 pagesKathleen E. Toomey, M.D., M.P.HdiskreaderrorNo ratings yet
- Handling Trauma and Burn PatientsDocument19 pagesHandling Trauma and Burn PatientsWhisky MiloNo ratings yet
- Covid-19: Guide On Home-Based Care, Screening & Isolation Ward Set UpDocument9 pagesCovid-19: Guide On Home-Based Care, Screening & Isolation Ward Set UpTech Person 03No ratings yet
- 77 - HCW Risk Assessment - Clean - 6.9.2020 Ns CleanDocument32 pages77 - HCW Risk Assessment - Clean - 6.9.2020 Ns CleanbobbyfildianNo ratings yet
- PATIENT SAFETY RECOMMENDATIONS Final Version PDFDocument59 pagesPATIENT SAFETY RECOMMENDATIONS Final Version PDFshinta hombingNo ratings yet
- Covid 2Document34 pagesCovid 2Inthe MOON youNo ratings yet
- Tanzania - SOPs For Case Management and Infection Prevention and ControlDocument115 pagesTanzania - SOPs For Case Management and Infection Prevention and ControlXuan Nguyen100% (1)
- Recommendations For Surgery During The Novel CoronavirusDocument5 pagesRecommendations For Surgery During The Novel CoronavirusHéctor Juárez GrandaNo ratings yet
- Covid19 - Eu Recommendations On Testing Strategies v2 PDFDocument2 pagesCovid19 - Eu Recommendations On Testing Strategies v2 PDFRomeo GhitaNo ratings yet
- Reabilitação Após Doença Crítica de CovidDocument5 pagesReabilitação Após Doença Crítica de CovidCristina BoaventuraNo ratings yet
- Covid 19 Prioritization of DX TestingDocument2 pagesCovid 19 Prioritization of DX TestingMatthew DavisNo ratings yet
- World Health Organization (WHO) Information Note Tuberculosis and COVID-19Document10 pagesWorld Health Organization (WHO) Information Note Tuberculosis and COVID-19WasimNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateDocument40 pagesCoronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateFlorin StanciuNo ratings yet
- DPH Covid-19 Healthcare Personnel Return To Work GuidanceDocument4 pagesDPH Covid-19 Healthcare Personnel Return To Work GuidancediskreaderrorNo ratings yet
- Basic Concepts in Infection Prevention and Control 2023Document44 pagesBasic Concepts in Infection Prevention and Control 2023Tannov SiregarNo ratings yet
- Scope and LimitationsDocument4 pagesScope and LimitationsRey Dela PeñaNo ratings yet
- COVIDDocument9 pagesCOVIDryan smithNo ratings yet
- Triage, Source Control and Additional Control Measures: IPC IPCDocument5 pagesTriage, Source Control and Additional Control Measures: IPC IPCRainbowDashNo ratings yet
- IPC GUIDELINE Version 2Document20 pagesIPC GUIDELINE Version 2Nrs KhalidNo ratings yet
- Checklist For Preparing Your IR Service For COVID-19Document8 pagesChecklist For Preparing Your IR Service For COVID-19uroshkgNo ratings yet
- Ways Operate EffectivelyDocument2 pagesWays Operate EffectivelyALEXANDRU CRISTIAN BUGLENo ratings yet
- Covid 1 PDFDocument17 pagesCovid 1 PDFPrajawira Smanti CilacapNo ratings yet
- Policy Recommendation On Covid-19Document4 pagesPolicy Recommendation On Covid-19RapplerNo ratings yet
- WORKPLACE READINESS FOR COVID Part 3Document37 pagesWORKPLACE READINESS FOR COVID Part 3LNo ratings yet
- Phase 1 Tasks and QuestionsDocument8 pagesPhase 1 Tasks and QuestionsEmmanuel RumbaoaNo ratings yet
- WHO 2019 nCoV IPC 2020.4 Eng - 29june20Document13 pagesWHO 2019 nCoV IPC 2020.4 Eng - 29june20Pusat Penjaminan Mutu Poltekkes PalembangNo ratings yet
- Infection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or ConfirmedDocument13 pagesInfection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or ConfirmedDina PrilyaNo ratings yet
- Updated Nursing Home Visitation GuidanceDocument8 pagesUpdated Nursing Home Visitation GuidanceWGRZ-TVNo ratings yet
- Health Clearance For Tuberculosis, Hepatitis B, Hepatitis C and HIVDocument49 pagesHealth Clearance For Tuberculosis, Hepatitis B, Hepatitis C and HIVNadya ErlianieNo ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19From EverandLiving on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19No ratings yet
- The Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNDocument52 pagesThe Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNrahmaya100% (1)
- Sage Microdeletion Example Screening ReportDocument4 pagesSage Microdeletion Example Screening ReportpathbiomedxNo ratings yet
- Comprensión Escrita 1: LauraDocument3 pagesComprensión Escrita 1: LauraSonia Garcia DiazNo ratings yet
- Soal Latihan Bhs. InggrisDocument12 pagesSoal Latihan Bhs. InggrisFitra FitraNo ratings yet
- Oops-Program 10-MduDocument6 pagesOops-Program 10-MduAtul MalhotraNo ratings yet
- National Rural Health MissionDocument37 pagesNational Rural Health MissionSanjeev SinghNo ratings yet
- Ashley Babb: ObjectiveDocument2 pagesAshley Babb: Objectiveapi-480600361No ratings yet
- Daftar Pustaka LeukokoriaDocument3 pagesDaftar Pustaka LeukokoriaElissa Dewi Lisencia FitriNo ratings yet
- Surgical ObturatorDocument4 pagesSurgical ObturatordentalteethNo ratings yet
- Wound Care NotesDocument5 pagesWound Care NotesdoctorniravNo ratings yet
- Conversation Between ProfessionsDocument3 pagesConversation Between ProfessionsHeryani AnikNo ratings yet
- Personal PronounsDocument2 pagesPersonal PronounsBárbara Souza SouzaNo ratings yet
- QDocument17 pagesQFarhana KanakanNo ratings yet
- Valores de Referecnia RocheDocument122 pagesValores de Referecnia RocheBI Corona0% (1)
- معايير تصميم و تخطيط المستشفياتDocument64 pagesمعايير تصميم و تخطيط المستشفياتJeEmONo ratings yet
- Murphy's SignDocument3 pagesMurphy's SignAdityaOviaPutriNo ratings yet
- Application No: B.SC (Nursing) Programme - Application Form - 2020Document4 pagesApplication No: B.SC (Nursing) Programme - Application Form - 2020ashamartinaNo ratings yet
- Jennifer Frank CV f18Document7 pagesJennifer Frank CV f18api-432068722No ratings yet
- Lenicek Krleza J Et Al Capillary Blood Sampling PDFDocument24 pagesLenicek Krleza J Et Al Capillary Blood Sampling PDFsinta purnama sariNo ratings yet
- Hospital Fires First Shot in Legal War Over EMS Services in Cherokee CountyDocument15 pagesHospital Fires First Shot in Legal War Over EMS Services in Cherokee CountyTim GullaNo ratings yet
- Case Slip Minor CaseDocument1 pageCase Slip Minor CaseRhea May CaporNo ratings yet
- Making Beds: PerformanceDocument2 pagesMaking Beds: PerformanceNicole NipasNo ratings yet
- MS Childrens Behavioral Health 3-6-15 FinalDocument152 pagesMS Childrens Behavioral Health 3-6-15 Finalthe kingfishNo ratings yet
- Payment Agreement PDFDocument1 pagePayment Agreement PDFLisa HalajkoNo ratings yet
- Do Mental Health and Self-Concept Associate With Rhinoplasty Requests?Document4 pagesDo Mental Health and Self-Concept Associate With Rhinoplasty Requests?Estevam HolpertNo ratings yet
- Special Probability Distribution Ii: Juhaidah Binti Jamal Faculty Education of Technical and VocationalDocument32 pagesSpecial Probability Distribution Ii: Juhaidah Binti Jamal Faculty Education of Technical and VocationalJuhaidah Jamal100% (2)
- 2019 Standard Booklet PDFDocument28 pages2019 Standard Booklet PDFclainNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- Quantitative Methods For Business 13th Edition Anderson Solutions ManualDocument14 pagesQuantitative Methods For Business 13th Edition Anderson Solutions ManualMicheleWallsertso100% (16)
- A Guide For Departments of Anaesthesia, Critical Care and Pain ManagementDocument57 pagesA Guide For Departments of Anaesthesia, Critical Care and Pain ManagementIrene Cristina100% (2)
- Tongue Tie: From Confusion To Clarity-A ReviewDocument4 pagesTongue Tie: From Confusion To Clarity-A Reviewrahmaputra100% (1)
- Local Resumption of Elective Surgery GuidanceDocument10 pagesLocal Resumption of Elective Surgery Guidancevjgg810199No ratings yet
- Manejo Ambulatorio AdultosDocument18 pagesManejo Ambulatorio AdultosCarlos Huaman ZevallosNo ratings yet
- AssignmentDocument5 pagesAssignmentClaire ChiuNo ratings yet
- Pulmonary Rehabilitation For COVID-19 PatientsDocument16 pagesPulmonary Rehabilitation For COVID-19 Patientspufu crisanNo ratings yet
- COVID 19 Physicians GuideDocument4 pagesCOVID 19 Physicians GuidenilrmNo ratings yet
- Covid 19 ProgramDocument12 pagesCovid 19 ProgramBAGUIO CATSNo ratings yet
- Resp Follow Up Guidance Post Covid PneumoniaDocument15 pagesResp Follow Up Guidance Post Covid PneumoniaAnindam SahaNo ratings yet
- Community Quarantine RecommendationsDocument5 pagesCommunity Quarantine RecommendationsRapplerNo ratings yet
- Joint Statement Resuming Elective Surgery After COVID19Document4 pagesJoint Statement Resuming Elective Surgery After COVID19vjgg810199No ratings yet
- Covid-19: Guide On Home-Based Care, Screening & Isolation Ward Set UpDocument9 pagesCovid-19: Guide On Home-Based Care, Screening & Isolation Ward Set Upvimalraj vtNo ratings yet
- Infection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsDocument20 pagesInfection Prevention and Control and Preparedness For COVID-19 in Healthcare SettingsMatthew DavisNo ratings yet
- Covid Flexibility Reopen Essential Non Covid ServicesDocument3 pagesCovid Flexibility Reopen Essential Non Covid ServicesDaniel RusseNo ratings yet
- Office of The Secretary: Temporary TreatmentDocument14 pagesOffice of The Secretary: Temporary TreatmentBenjamin Karlo Delos SantosNo ratings yet
- Clinical Guidance For Managing Suspected COVID 19 Patients in ICRC Supported Hospitals 05.04.2020 - FianlDocument7 pagesClinical Guidance For Managing Suspected COVID 19 Patients in ICRC Supported Hospitals 05.04.2020 - FianlCrys TahNo ratings yet
- Guideline For Conservation of Respiratory Protection ResourcesDocument14 pagesGuideline For Conservation of Respiratory Protection ResourcesAMEU URGENCIASNo ratings yet
- COVID19 IPCProtocolSurgicalProceduresAdultDocument16 pagesCOVID19 IPCProtocolSurgicalProceduresAdultwatimelawatiNo ratings yet
- Preparing Your Intensive Care Unit For The COVID - ASLIDocument24 pagesPreparing Your Intensive Care Unit For The COVID - ASLIEven EdomekoNo ratings yet
- Covid Cohorting PacDocument5 pagesCovid Cohorting PacsimplyrosalynNo ratings yet
- COVID 19 Outpatient DialysisDocument5 pagesCOVID 19 Outpatient DialysisTheala RadistaNo ratings yet
- AdultCriticalCare COVID 19 October2020Document21 pagesAdultCriticalCare COVID 19 October2020Maria Josefina RaffinNo ratings yet
- Guidance For Routine Immunization Services During COVID-19: - PageDocument14 pagesGuidance For Routine Immunization Services During COVID-19: - PagePrisma CahyaNo ratings yet
- Privateroom JournalDocument5 pagesPrivateroom JournalNathaniel PulidoNo ratings yet
- Importance of Healthcare in Covid TimeDocument4 pagesImportance of Healthcare in Covid TimeEditor IJTSRDNo ratings yet
- COVID 19 Antigen Testing GuidelinesDocument12 pagesCOVID 19 Antigen Testing GuidelinesStephanie SánchezNo ratings yet
- prehospital-EMS-COVID-19-recommendations - 4.4Document19 pagesprehospital-EMS-COVID-19-recommendations - 4.4MEONENo ratings yet
- Neurologic Emergencies During The Coronavirus DiseDocument17 pagesNeurologic Emergencies During The Coronavirus DiseCristina CalzadaNo ratings yet
- C0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchDocument4 pagesC0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchKevo VillagranNo ratings yet
- Teknik Resus BosaertDocument13 pagesTeknik Resus BosaertDADASDSANo ratings yet
- Diagnosis and Management of Community-Acquired Pneumonia: Evidence-Based PracticeDocument11 pagesDiagnosis and Management of Community-Acquired Pneumonia: Evidence-Based PracticeMega Julia ThioNo ratings yet
- Hemodialysis Unit Preparedness COVID-19 Pandemic: During and AfterDocument8 pagesHemodialysis Unit Preparedness COVID-19 Pandemic: During and Afteryanuar esthoNo ratings yet
- Kathleen E. Toomey, M.D., M.P.HDocument3 pagesKathleen E. Toomey, M.D., M.P.HdiskreaderrorNo ratings yet
- Handling Trauma and Burn PatientsDocument19 pagesHandling Trauma and Burn PatientsWhisky MiloNo ratings yet
- Covid-19: Guide On Home-Based Care, Screening & Isolation Ward Set UpDocument9 pagesCovid-19: Guide On Home-Based Care, Screening & Isolation Ward Set UpTech Person 03No ratings yet
- 77 - HCW Risk Assessment - Clean - 6.9.2020 Ns CleanDocument32 pages77 - HCW Risk Assessment - Clean - 6.9.2020 Ns CleanbobbyfildianNo ratings yet
- PATIENT SAFETY RECOMMENDATIONS Final Version PDFDocument59 pagesPATIENT SAFETY RECOMMENDATIONS Final Version PDFshinta hombingNo ratings yet
- Covid 2Document34 pagesCovid 2Inthe MOON youNo ratings yet
- Tanzania - SOPs For Case Management and Infection Prevention and ControlDocument115 pagesTanzania - SOPs For Case Management and Infection Prevention and ControlXuan Nguyen100% (1)
- Recommendations For Surgery During The Novel CoronavirusDocument5 pagesRecommendations For Surgery During The Novel CoronavirusHéctor Juárez GrandaNo ratings yet
- Covid19 - Eu Recommendations On Testing Strategies v2 PDFDocument2 pagesCovid19 - Eu Recommendations On Testing Strategies v2 PDFRomeo GhitaNo ratings yet
- Reabilitação Após Doença Crítica de CovidDocument5 pagesReabilitação Após Doença Crítica de CovidCristina BoaventuraNo ratings yet
- Covid 19 Prioritization of DX TestingDocument2 pagesCovid 19 Prioritization of DX TestingMatthew DavisNo ratings yet
- World Health Organization (WHO) Information Note Tuberculosis and COVID-19Document10 pagesWorld Health Organization (WHO) Information Note Tuberculosis and COVID-19WasimNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateDocument40 pagesCoronavirus Disease 2019 (COVID-19) - Infection Control in Health Care and Home Settings - UpToDateFlorin StanciuNo ratings yet
- DPH Covid-19 Healthcare Personnel Return To Work GuidanceDocument4 pagesDPH Covid-19 Healthcare Personnel Return To Work GuidancediskreaderrorNo ratings yet
- Basic Concepts in Infection Prevention and Control 2023Document44 pagesBasic Concepts in Infection Prevention and Control 2023Tannov SiregarNo ratings yet
- Scope and LimitationsDocument4 pagesScope and LimitationsRey Dela PeñaNo ratings yet
- COVIDDocument9 pagesCOVIDryan smithNo ratings yet
- Triage, Source Control and Additional Control Measures: IPC IPCDocument5 pagesTriage, Source Control and Additional Control Measures: IPC IPCRainbowDashNo ratings yet
- IPC GUIDELINE Version 2Document20 pagesIPC GUIDELINE Version 2Nrs KhalidNo ratings yet
- Checklist For Preparing Your IR Service For COVID-19Document8 pagesChecklist For Preparing Your IR Service For COVID-19uroshkgNo ratings yet
- Ways Operate EffectivelyDocument2 pagesWays Operate EffectivelyALEXANDRU CRISTIAN BUGLENo ratings yet
- Covid 1 PDFDocument17 pagesCovid 1 PDFPrajawira Smanti CilacapNo ratings yet
- Policy Recommendation On Covid-19Document4 pagesPolicy Recommendation On Covid-19RapplerNo ratings yet
- WORKPLACE READINESS FOR COVID Part 3Document37 pagesWORKPLACE READINESS FOR COVID Part 3LNo ratings yet
- Phase 1 Tasks and QuestionsDocument8 pagesPhase 1 Tasks and QuestionsEmmanuel RumbaoaNo ratings yet
- WHO 2019 nCoV IPC 2020.4 Eng - 29june20Document13 pagesWHO 2019 nCoV IPC 2020.4 Eng - 29june20Pusat Penjaminan Mutu Poltekkes PalembangNo ratings yet
- Infection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or ConfirmedDocument13 pagesInfection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or ConfirmedDina PrilyaNo ratings yet
- Updated Nursing Home Visitation GuidanceDocument8 pagesUpdated Nursing Home Visitation GuidanceWGRZ-TVNo ratings yet
- Health Clearance For Tuberculosis, Hepatitis B, Hepatitis C and HIVDocument49 pagesHealth Clearance For Tuberculosis, Hepatitis B, Hepatitis C and HIVNadya ErlianieNo ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19From EverandLiving on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19No ratings yet
- The Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNDocument52 pagesThe Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNrahmaya100% (1)
- Sage Microdeletion Example Screening ReportDocument4 pagesSage Microdeletion Example Screening ReportpathbiomedxNo ratings yet
- Comprensión Escrita 1: LauraDocument3 pagesComprensión Escrita 1: LauraSonia Garcia DiazNo ratings yet
- Soal Latihan Bhs. InggrisDocument12 pagesSoal Latihan Bhs. InggrisFitra FitraNo ratings yet
- Oops-Program 10-MduDocument6 pagesOops-Program 10-MduAtul MalhotraNo ratings yet
- National Rural Health MissionDocument37 pagesNational Rural Health MissionSanjeev SinghNo ratings yet
- Ashley Babb: ObjectiveDocument2 pagesAshley Babb: Objectiveapi-480600361No ratings yet
- Daftar Pustaka LeukokoriaDocument3 pagesDaftar Pustaka LeukokoriaElissa Dewi Lisencia FitriNo ratings yet
- Surgical ObturatorDocument4 pagesSurgical ObturatordentalteethNo ratings yet
- Wound Care NotesDocument5 pagesWound Care NotesdoctorniravNo ratings yet
- Conversation Between ProfessionsDocument3 pagesConversation Between ProfessionsHeryani AnikNo ratings yet
- Personal PronounsDocument2 pagesPersonal PronounsBárbara Souza SouzaNo ratings yet
- QDocument17 pagesQFarhana KanakanNo ratings yet
- Valores de Referecnia RocheDocument122 pagesValores de Referecnia RocheBI Corona0% (1)
- معايير تصميم و تخطيط المستشفياتDocument64 pagesمعايير تصميم و تخطيط المستشفياتJeEmONo ratings yet
- Murphy's SignDocument3 pagesMurphy's SignAdityaOviaPutriNo ratings yet
- Application No: B.SC (Nursing) Programme - Application Form - 2020Document4 pagesApplication No: B.SC (Nursing) Programme - Application Form - 2020ashamartinaNo ratings yet
- Jennifer Frank CV f18Document7 pagesJennifer Frank CV f18api-432068722No ratings yet
- Lenicek Krleza J Et Al Capillary Blood Sampling PDFDocument24 pagesLenicek Krleza J Et Al Capillary Blood Sampling PDFsinta purnama sariNo ratings yet
- Hospital Fires First Shot in Legal War Over EMS Services in Cherokee CountyDocument15 pagesHospital Fires First Shot in Legal War Over EMS Services in Cherokee CountyTim GullaNo ratings yet
- Case Slip Minor CaseDocument1 pageCase Slip Minor CaseRhea May CaporNo ratings yet
- Making Beds: PerformanceDocument2 pagesMaking Beds: PerformanceNicole NipasNo ratings yet
- MS Childrens Behavioral Health 3-6-15 FinalDocument152 pagesMS Childrens Behavioral Health 3-6-15 Finalthe kingfishNo ratings yet
- Payment Agreement PDFDocument1 pagePayment Agreement PDFLisa HalajkoNo ratings yet
- Do Mental Health and Self-Concept Associate With Rhinoplasty Requests?Document4 pagesDo Mental Health and Self-Concept Associate With Rhinoplasty Requests?Estevam HolpertNo ratings yet
- Special Probability Distribution Ii: Juhaidah Binti Jamal Faculty Education of Technical and VocationalDocument32 pagesSpecial Probability Distribution Ii: Juhaidah Binti Jamal Faculty Education of Technical and VocationalJuhaidah Jamal100% (2)
- 2019 Standard Booklet PDFDocument28 pages2019 Standard Booklet PDFclainNo ratings yet