Download as docx, pdf, or txt
You might also like
- BWS Female Beginner - Phase 2 Workouts - 4 Days PDFDocument50 pagesBWS Female Beginner - Phase 2 Workouts - 4 Days PDFhmimez100% (1)
- Frenkel's ExerciseDocument2 pagesFrenkel's ExerciseAnusha AppajiNo ratings yet
- 108 KaranasDocument37 pages108 Karanasbikergal0% (1)
- ECG Interpretation Made Incredibly Easy! (5th Edition)Document6 pagesECG Interpretation Made Incredibly Easy! (5th Edition)Islam AminNo ratings yet
- Dr. Waqas Ayubian Notes For Step 3Document772 pagesDr. Waqas Ayubian Notes For Step 3Muhammad HammadNo ratings yet
- Gait Phases Kinetics Kinema TicsDocument36 pagesGait Phases Kinetics Kinema Ticsjonrocks100% (1)
- CTEVDocument61 pagesCTEVSylvia LoongNo ratings yet
- Definition: Is A Condition Resulting in Partial or Complete Separation of A Segment of Normal Hyaline Cartilage From It's Supporting BoneDocument8 pagesDefinition: Is A Condition Resulting in Partial or Complete Separation of A Segment of Normal Hyaline Cartilage From It's Supporting BoneKarla Chariz Fernandez BayagNo ratings yet
- Cavus Foot 2015 Foot and Ankle ClinicsDocument13 pagesCavus Foot 2015 Foot and Ankle ClinicsRadu StoenescuNo ratings yet
- Anomalies of Skeletal System-1Document44 pagesAnomalies of Skeletal System-1Meena Koushal100% (1)
- Anomalies of Skeletal System-1Document44 pagesAnomalies of Skeletal System-1Meena Koushal100% (1)
- TC, SB, DDH, CtevDocument23 pagesTC, SB, DDH, CtevMukharradhiNo ratings yet
- Cavus Foot: Monica Paschoal Nogueira,, Fernando Farcetta,, Alexandre ZucconDocument12 pagesCavus Foot: Monica Paschoal Nogueira,, Fernando Farcetta,, Alexandre ZucconCesar AlvaradoNo ratings yet
- Koreksi KontrakturDocument14 pagesKoreksi KontrakturarifNo ratings yet
- MX - Stiff ElbowDocument8 pagesMX - Stiff ElbowPrabath ChinthakaNo ratings yet
- Congenital DeformitiesDocument102 pagesCongenital DeformitiesFahmi MujahidNo ratings yet
- Andi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtDocument30 pagesAndi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtAndi Rahmat HidayatNo ratings yet
- IOM in Scoliosis TMHDocument75 pagesIOM in Scoliosis TMHtuanemgNo ratings yet
- Referat Reconstruction IDocument7 pagesReferat Reconstruction IReza Devianto HambaliNo ratings yet
- Medscape Knee OCDDocument16 pagesMedscape Knee OCDDita Ambarsari SyafruddinNo ratings yet
- Etiology: Congenital Talipes Equinovarus (Clubfoot)Document23 pagesEtiology: Congenital Talipes Equinovarus (Clubfoot)victormoirangthemNo ratings yet
- Acetabular Dysplasia in Adults - JBJSDocument3 pagesAcetabular Dysplasia in Adults - JBJSErnesto Ewertz MiquelNo ratings yet
- 2014 Article 9237Document6 pages2014 Article 9237Mahmoud A KhatabNo ratings yet
- Legg-Calvé-Perthes Disease: Roberto E. Novo, DVM, DACVSDocument2 pagesLegg-Calvé-Perthes Disease: Roberto E. Novo, DVM, DACVSEdi BackyNo ratings yet
- CTEVDocument46 pagesCTEVjhogie afitnandriNo ratings yet
- Adult FlatfootDocument7 pagesAdult FlatfootAbraham SaldañaNo ratings yet
- Pinzamiento de Cadea Pincer CamDocument9 pagesPinzamiento de Cadea Pincer Camvlc driveNo ratings yet
- Paediatric Clubfoot: Differential DiagnosisDocument10 pagesPaediatric Clubfoot: Differential DiagnosisVishwas MohanNo ratings yet
- Joint Instability: Hendradi Khumarga SPOT. FICSDocument48 pagesJoint Instability: Hendradi Khumarga SPOT. FICSJoshua ObrienNo ratings yet
- Vascular Symptoms. Vascular Symptoms Include Syncope, Vertigo, Intermittent PeriodsDocument16 pagesVascular Symptoms. Vascular Symptoms Include Syncope, Vertigo, Intermittent Periodsalbertina tebayNo ratings yet
- JurnalDocument5 pagesJurnalQorin Diin ArifniNo ratings yet
- Congenital AbnormalitiesDocument37 pagesCongenital AbnormalitiesrezkadehaNo ratings yet
- 2.8 Additional Radio Graphic Views of The Thoracic Limb in DogsDocument8 pages2.8 Additional Radio Graphic Views of The Thoracic Limb in DogsMiri MorganNo ratings yet
- Refer atDocument9 pagesRefer atMaharani Dhian KusumawatiNo ratings yet
- Foot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Document15 pagesFoot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Biblioteca Centro Médico De Mar del PlataNo ratings yet
- William C. Cottrell, MD AbstractDocument4 pagesWilliam C. Cottrell, MD AbstractmalaNo ratings yet
- Neurofibromatosis Pada Tulang BelakangDocument8 pagesNeurofibromatosis Pada Tulang Belakangdadakan16No ratings yet
- Spinal StenosisDocument14 pagesSpinal Stenosisshwampa100% (3)
- Treatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisDocument5 pagesTreatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisPeko PekoNo ratings yet
- Pes Cavus ....Document34 pagesPes Cavus ....Rupika Sodhi100% (2)
- Presentor-Dr. Momin Mohammad Farhan Moderator-Dr. M. A. Q. AnsariDocument48 pagesPresentor-Dr. Momin Mohammad Farhan Moderator-Dr. M. A. Q. Ansarimohammad farhanNo ratings yet
- Congenital Talipes EquinovarusDocument24 pagesCongenital Talipes EquinovarusVipul Nagnesia100% (1)
- Posterior Dislocation of The Hip JointDocument25 pagesPosterior Dislocation of The Hip JointadibahNo ratings yet
- Patellar Tendon RuptureDocument13 pagesPatellar Tendon Rupturededyalkarni08No ratings yet
- Lower Extremity DisordersDocument8 pagesLower Extremity DisordersisauraNo ratings yet
- Cervical Spondylotic MyelopathyDocument9 pagesCervical Spondylotic MyelopathyShonima VivishNo ratings yet
- Fracture-Dislocation of The Hip-KaizarDocument69 pagesFracture-Dislocation of The Hip-KaizarKaizar Ennis100% (1)
- Hallux VarusDocument4 pagesHallux VarusmadziiieNo ratings yet
- LUMBAR DISC NotesDocument7 pagesLUMBAR DISC NotesPrasadNo ratings yet
- Aaos2007 Hip Knee PDFDocument61 pagesAaos2007 Hip Knee PDFHéctor Pando Sánchez100% (1)
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- Wagner 2021Document17 pagesWagner 2021Biblioteca Centro Médico De Mar del PlataNo ratings yet
- Cerebral PalsyDocument16 pagesCerebral PalsyReza Devianto HambaliNo ratings yet
- Pain Spine Disorders - MainDocument10 pagesPain Spine Disorders - Mainsimona mariana dutuNo ratings yet
- Develop Med Child Neuro - 2009 - ROOT - Surgical Treatment For Hip Pain in The Adult Cerebral Palsy PatientDocument8 pagesDevelop Med Child Neuro - 2009 - ROOT - Surgical Treatment For Hip Pain in The Adult Cerebral Palsy PatientSitthikorn StrikerrNo ratings yet
- V67N1 4 PDFDocument8 pagesV67N1 4 PDFAndrésOlivaRossiNo ratings yet
- KyphosisDocument32 pagesKyphosisBeniamin CostinașNo ratings yet
- Lumbar Spine Stenosis: A Common Cause of Back and Leg Pain: Normal AnatomyDocument13 pagesLumbar Spine Stenosis: A Common Cause of Back and Leg Pain: Normal Anatomyhunter_axl01No ratings yet
- CP SybpoDocument40 pagesCP SybpoIipo ChennaiNo ratings yet
- Lumbar Spine StenosisDocument12 pagesLumbar Spine StenosisParag DashatwarNo ratings yet
- Osteotomias PediatriaDocument13 pagesOsteotomias PediatriaM Ram CrraNo ratings yet
- Coxa PlanaDocument15 pagesCoxa PlanaAngelyn MoralNo ratings yet
- Gadline PrsentationDocument12 pagesGadline PrsentationsumardiNo ratings yet
- Hip Disorders in Children: Postgraduate Orthopaedics SeriesFrom EverandHip Disorders in Children: Postgraduate Orthopaedics SeriesRating: 3 out of 5 stars3/5 (2)
- Stroke Impact Scale SISDocument6 pagesStroke Impact Scale SISJohann Sebastian CruzNo ratings yet
- Neurologic ExaminationDocument6 pagesNeurologic ExaminationJohann Sebastian CruzNo ratings yet
- Serenity Prayer PrintableDocument1 pageSerenity Prayer PrintableJohann Sebastian CruzNo ratings yet
- KINESIOLOGY - Carmina Cortez, MD - September 27, 2017Document9 pagesKINESIOLOGY - Carmina Cortez, MD - September 27, 2017Johann Sebastian CruzNo ratings yet
- SR OF CVsDocument16 pagesSR OF CVsJohann Sebastian CruzNo ratings yet
- PT 1 Midterm RubricDocument3 pagesPT 1 Midterm RubricJohann Sebastian CruzNo ratings yet
- Physical Therapy Research 1 Manual: Find A Review of Related To YourDocument5 pagesPhysical Therapy Research 1 Manual: Find A Review of Related To YourJohann Sebastian CruzNo ratings yet
- Pathophysiology of Bacterial Infections Cheat Sheet: by ViaDocument5 pagesPathophysiology of Bacterial Infections Cheat Sheet: by ViaJohann Sebastian CruzNo ratings yet
- The Skeletal & Articular SystemsDocument11 pagesThe Skeletal & Articular SystemsJohann Sebastian CruzNo ratings yet
- AFRICAN AMERICAN CULTURE by Group Two 1Document61 pagesAFRICAN AMERICAN CULTURE by Group Two 1Johann Sebastian CruzNo ratings yet
- Hispanic CultureDocument76 pagesHispanic CultureJohann Sebastian CruzNo ratings yet
- The Ability of The Landing Error Scoring System To Detect Changes in Landing Mechanics: A Critically Appraised TopicDocument9 pagesThe Ability of The Landing Error Scoring System To Detect Changes in Landing Mechanics: A Critically Appraised TopicJohann Sebastian CruzNo ratings yet
- Final MD HGD ReportDocument100 pagesFinal MD HGD ReportJohann Sebastian CruzNo ratings yet
- Head and Neck - MusclesDocument3 pagesHead and Neck - MusclesJohann Sebastian CruzNo ratings yet
- CPM18th Parkinson - S DiseaseDocument19 pagesCPM18th Parkinson - S DiseaseJohann Sebastian CruzNo ratings yet
- Blood Physiology: General FunctionsDocument13 pagesBlood Physiology: General FunctionsJohann Sebastian CruzNo ratings yet
- Medicine The American Journal of SportsDocument7 pagesMedicine The American Journal of SportsJohann Sebastian CruzNo ratings yet
- Activity WorksheetDocument1 pageActivity WorksheetJohann Sebastian CruzNo ratings yet
- Basal Ganglia: Corpus StriatumDocument5 pagesBasal Ganglia: Corpus StriatumJohann Sebastian CruzNo ratings yet
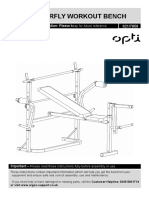
- Opti Butterfly Workout Bench: Assembly & User Instruction 621/7859Document27 pagesOpti Butterfly Workout Bench: Assembly & User Instruction 621/7859TunaNo ratings yet
- Dynamic Stretching For AthletesDocument6 pagesDynamic Stretching For Athletesshivnair100% (2)
- Chevron or Austin Metatarsal OsteotomyDocument5 pagesChevron or Austin Metatarsal OsteotomyAndré LaranjoNo ratings yet
- Warm Up ProgramDocument10 pagesWarm Up ProgrammnbvqwertNo ratings yet
- Khulna University of Engineering & TechnologyDocument49 pagesKhulna University of Engineering & Technology17044 AZMAIN IKTIDER AKASHNo ratings yet
- HealthDocument12 pagesHealthazuldraconNo ratings yet
- L Mollart Pregnancy Oedema, Emotions and ReflexologyDocument7 pagesL Mollart Pregnancy Oedema, Emotions and ReflexologyMoh. Fahmi FathullahNo ratings yet
- Foot Measuring Tips - Drew'sDocument1 pageFoot Measuring Tips - Drew'ssam suckNo ratings yet
- Untuk Dikirim Pesanan-2022-12-22-18 - 40Document7 pagesUntuk Dikirim Pesanan-2022-12-22-18 - 40Dodit SikacangNo ratings yet
- RRASSINGMENTDocument12 pagesRRASSINGMENTAditi RajoraNo ratings yet
- Two-Dimensional Inverse DynamicsDocument22 pagesTwo-Dimensional Inverse DynamicsEric Urbina SantibañezNo ratings yet
- Screenshot 2023-01-10 at 11.40.36 AMDocument67 pagesScreenshot 2023-01-10 at 11.40.36 AMAnchal LohanaNo ratings yet
- Journal 4 PDFDocument5 pagesJournal 4 PDFSylviany El NovitaNo ratings yet
- Bodyguard E-Brochure 2021Document6 pagesBodyguard E-Brochure 2021Nate JamesNo ratings yet
- Warmup VolleyballDocument2 pagesWarmup Volleyballapi-345720435No ratings yet
- Nama Latin TulangDocument4 pagesNama Latin TulangMuhammad Urfan SNo ratings yet
- Legs and Glutes Part 2Document5 pagesLegs and Glutes Part 2swati-tiwari-8626No ratings yet
- Fitness WalkingDocument192 pagesFitness Walkingjha.sofcon5941100% (1)
- JazzDocument2 pagesJazzCindy Graze EscaleraNo ratings yet
- Unit 2Document17 pagesUnit 2Garvit GargNo ratings yet
- Anatomy and Physiology Lab Activity 9Document4 pagesAnatomy and Physiology Lab Activity 9Kylene Gayle MoralesNo ratings yet
- Brunstorm'sDocument19 pagesBrunstorm'sHARSH 23 (Jalu)No ratings yet
- Ankle Sprain Rehab 1Document3 pagesAnkle Sprain Rehab 1John NixonNo ratings yet
- RS Flip-FlopDocument2 pagesRS Flip-FlopDenis KukuljacNo ratings yet
- Surgical Treatment of ClubfootDocument49 pagesSurgical Treatment of Clubfootvishwas dabasNo ratings yet
- Bingo Games Falls AwarenessDocument21 pagesBingo Games Falls AwarenessFallsAssistUKNo ratings yet