
Organization of Endovascular Thrombectomy The Need For A 2-Tier System
Organization of Endovascular Thrombectomy The Need For A 2-Tier System
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- IES Test Prep Answer Explanations For SAT GrammarDocument72 pagesIES Test Prep Answer Explanations For SAT GrammarĐ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘̚ Đ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘75% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
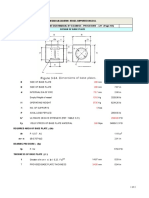
- Leg Support Calculation PDFDocument2 pagesLeg Support Calculation PDFSanjay MoreNo ratings yet
- 120lab Report 3Document4 pages120lab Report 3Valerie Mae Librero Areño100% (2)
- EASA Part-66 Exam Questions of Module 01 - Part IIDocument24 pagesEASA Part-66 Exam Questions of Module 01 - Part IISteven J. Selcuk100% (2)
- Directory of SMEs in India-2012 EditionDocument7,115 pagesDirectory of SMEs in India-2012 EditionNilesh RanaNo ratings yet
- MEP MyanmarDocument27 pagesMEP Myanmarempty87No ratings yet
- Filipino BasicDocument21 pagesFilipino BasicReiko Nakayama100% (1)
- Advanced Landscape DesignDocument10 pagesAdvanced Landscape DesignSomhita DasNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- He Is A Chocolate Lover: Kamaladevi RengasamyDocument4 pagesHe Is A Chocolate Lover: Kamaladevi RengasamyKamala DeviNo ratings yet
- Textbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFDocument39 pagesTextbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFjanet.galloway812100% (8)
- BW Inside CiscoDocument3 pagesBW Inside CiscoMunkhbayar BaadgaiNo ratings yet
- Functional Specification For Deck CraneDocument31 pagesFunctional Specification For Deck Craneaiyubi20% (1)
- Delhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsDocument3 pagesDelhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsAnishikaNo ratings yet
- Yuxi CatalogueDocument16 pagesYuxi CatalogueSoltani AliNo ratings yet
- EQUILIBRIUMDocument1 pageEQUILIBRIUMMohammed IliasNo ratings yet
- WiringDocument147 pagesWiringYovani Cortes50% (2)
- Petroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityDocument13 pagesPetroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityAli AbubakarNo ratings yet
- Schiavi Enc Met Page015Document1 pageSchiavi Enc Met Page015Adel AdelNo ratings yet
- HwyconstDocument23 pagesHwyconstAmulie JarjuseyNo ratings yet
- Ex 4Document4 pagesEx 420-MCE-63 SYED HASSAN KUMAILNo ratings yet
- Valve Body 55Document3 pagesValve Body 55Davidoff RedNo ratings yet
- Bael-Tree Details and Medicinal UsesDocument4 pagesBael-Tree Details and Medicinal UsesSanjay PatilNo ratings yet
- Drawing Details: Cie 332 Quantity Surveying and Estimation Lecture Two Lecturer: Eng. Goodson MashekaDocument23 pagesDrawing Details: Cie 332 Quantity Surveying and Estimation Lecture Two Lecturer: Eng. Goodson MashekaPerpetual hubbyNo ratings yet
- Inverse of A FunctionDocument10 pagesInverse of A Functionnitin30100% (2)
- W8 Module08 Meaning and Relevance of History Presentation 1Document22 pagesW8 Module08 Meaning and Relevance of History Presentation 1Jessa UdtohanNo ratings yet
- NT Seq DatabaseDocument4 pagesNT Seq DatabaseDevinder KaurNo ratings yet
- KONAN Emmanuel Sales Technical Engineer 16 Juin 23Document1 pageKONAN Emmanuel Sales Technical Engineer 16 Juin 23EMMANUEL KONANNo ratings yet
- Absolute Priority Based Cell ReselectionDocument11 pagesAbsolute Priority Based Cell ReselectionNeoRa Ndivo RamsNo ratings yet
- A. Title of Experiment B. Date and Time of Experiment: Wednesday, 10Document15 pagesA. Title of Experiment B. Date and Time of Experiment: Wednesday, 10LichaNo ratings yet





































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- IES Test Prep Answer Explanations For SAT GrammarDocument72 pagesIES Test Prep Answer Explanations For SAT GrammarĐ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘̚ Đ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘75% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Leg Support Calculation PDFDocument2 pagesLeg Support Calculation PDFSanjay MoreNo ratings yet
- 120lab Report 3Document4 pages120lab Report 3Valerie Mae Librero Areño100% (2)
- EASA Part-66 Exam Questions of Module 01 - Part IIDocument24 pagesEASA Part-66 Exam Questions of Module 01 - Part IISteven J. Selcuk100% (2)
- Directory of SMEs in India-2012 EditionDocument7,115 pagesDirectory of SMEs in India-2012 EditionNilesh RanaNo ratings yet
- MEP MyanmarDocument27 pagesMEP Myanmarempty87No ratings yet
- Filipino BasicDocument21 pagesFilipino BasicReiko Nakayama100% (1)
- Advanced Landscape DesignDocument10 pagesAdvanced Landscape DesignSomhita DasNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- He Is A Chocolate Lover: Kamaladevi RengasamyDocument4 pagesHe Is A Chocolate Lover: Kamaladevi RengasamyKamala DeviNo ratings yet
- Textbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFDocument39 pagesTextbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFjanet.galloway812100% (8)
- BW Inside CiscoDocument3 pagesBW Inside CiscoMunkhbayar BaadgaiNo ratings yet
- Functional Specification For Deck CraneDocument31 pagesFunctional Specification For Deck Craneaiyubi20% (1)
- Delhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsDocument3 pagesDelhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsAnishikaNo ratings yet
- Yuxi CatalogueDocument16 pagesYuxi CatalogueSoltani AliNo ratings yet
- EQUILIBRIUMDocument1 pageEQUILIBRIUMMohammed IliasNo ratings yet
- WiringDocument147 pagesWiringYovani Cortes50% (2)
- Petroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityDocument13 pagesPetroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityAli AbubakarNo ratings yet
- Schiavi Enc Met Page015Document1 pageSchiavi Enc Met Page015Adel AdelNo ratings yet
- HwyconstDocument23 pagesHwyconstAmulie JarjuseyNo ratings yet
- Ex 4Document4 pagesEx 420-MCE-63 SYED HASSAN KUMAILNo ratings yet
- Valve Body 55Document3 pagesValve Body 55Davidoff RedNo ratings yet
- Bael-Tree Details and Medicinal UsesDocument4 pagesBael-Tree Details and Medicinal UsesSanjay PatilNo ratings yet
- Drawing Details: Cie 332 Quantity Surveying and Estimation Lecture Two Lecturer: Eng. Goodson MashekaDocument23 pagesDrawing Details: Cie 332 Quantity Surveying and Estimation Lecture Two Lecturer: Eng. Goodson MashekaPerpetual hubbyNo ratings yet
- Inverse of A FunctionDocument10 pagesInverse of A Functionnitin30100% (2)
- W8 Module08 Meaning and Relevance of History Presentation 1Document22 pagesW8 Module08 Meaning and Relevance of History Presentation 1Jessa UdtohanNo ratings yet
- NT Seq DatabaseDocument4 pagesNT Seq DatabaseDevinder KaurNo ratings yet
- KONAN Emmanuel Sales Technical Engineer 16 Juin 23Document1 pageKONAN Emmanuel Sales Technical Engineer 16 Juin 23EMMANUEL KONANNo ratings yet
- Absolute Priority Based Cell ReselectionDocument11 pagesAbsolute Priority Based Cell ReselectionNeoRa Ndivo RamsNo ratings yet
- A. Title of Experiment B. Date and Time of Experiment: Wednesday, 10Document15 pagesA. Title of Experiment B. Date and Time of Experiment: Wednesday, 10LichaNo ratings yet