Download as pdf or txt
You might also like
- Perspectives in Nutrition 7th EditionDocument1,037 pagesPerspectives in Nutrition 7th EditionAlizoo MalikNo ratings yet
- Nutrition Month Quiz Bee ReviewerDocument6 pagesNutrition Month Quiz Bee ReviewerNicholai Escalona100% (1)
- Biochemistry MnemonicsDocument20 pagesBiochemistry MnemonicsAnnapurna Dangeti100% (1)
- DyslipidemiaDocument44 pagesDyslipidemiaenri100% (1)
- Lipids Case StudiesDocument6 pagesLipids Case Studiesgogo29% (7)
- HyperlipidemiaDocument11 pagesHyperlipidemiaDevaky_Dealish_182No ratings yet
- Hyperlipidemia: Michele Ritter, M.D. Argy Resident - February, 2007Document22 pagesHyperlipidemia: Michele Ritter, M.D. Argy Resident - February, 2007Ritha WidyaNo ratings yet
- In Partial Fulfillment of The Requirements in Medical Ward RotationDocument5 pagesIn Partial Fulfillment of The Requirements in Medical Ward RotationEiz CabreraNo ratings yet
- Jurnal HyperlipidemiaDocument12 pagesJurnal HyperlipidemiaJo LenongNo ratings yet
- Thalasemia and HemoglobinopathiDocument57 pagesThalasemia and HemoglobinopathiChristan Chaputtra MaharibeNo ratings yet
- Nursing Care Plan Funds 2Document7 pagesNursing Care Plan Funds 2Yash RamawatNo ratings yet
- Cultural Interview: Filipino AmericanDocument11 pagesCultural Interview: Filipino AmericanLauren Kalanta100% (1)
- Use of Vasopressors and InotropesDocument14 pagesUse of Vasopressors and InotropesEdwin VargasNo ratings yet
- ThalasemiaDocument13 pagesThalasemiaapi-3802092100% (1)
- Multiple Sclerosis AANN-ARN-IOMSN-MS-Guideline - FINAL PDFDocument49 pagesMultiple Sclerosis AANN-ARN-IOMSN-MS-Guideline - FINAL PDFCyntia Theresia LumintangNo ratings yet
- HyperlipidemiaDocument29 pagesHyperlipidemiagowthamNo ratings yet
- rối loạn lipid máu PDFDocument107 pagesrối loạn lipid máu PDFNguyễn MaiNo ratings yet
- Genetic Disorders Causing Hypertriglyceridemia in Children and AdolescentsDocument32 pagesGenetic Disorders Causing Hypertriglyceridemia in Children and AdolescentsThanasis PapatheodorouNo ratings yet
- Notes Chapter 35Document16 pagesNotes Chapter 35Christene GVNo ratings yet
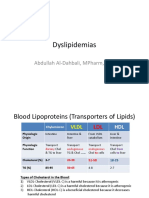
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Final Case StudyDocument5 pagesFinal Case StudyChelo Jan GeronimoNo ratings yet
- Lecture 24 - Plasma Ins 2 - 2006Document30 pagesLecture 24 - Plasma Ins 2 - 2006api-3703352No ratings yet
- TX LipidosDocument14 pagesTX Lipidosxander trujilloNo ratings yet
- Trusted Medical Answers-In Seconds.: Lipid DisordersDocument13 pagesTrusted Medical Answers-In Seconds.: Lipid DisordersMohammed shamiul Shahid100% (1)
- GGN Metabolisme LemakDocument24 pagesGGN Metabolisme LemakAzzahra Nur FadhilahNo ratings yet
- Dislipidemia Lancet Durrington PDFDocument15 pagesDislipidemia Lancet Durrington PDFAlphaJulissa JuarezNo ratings yet
- Mbs127 Slide DislipidemiaDocument45 pagesMbs127 Slide DislipidemiaDaru KristiyonoNo ratings yet
- Lipid Biokimia Semester 2Document93 pagesLipid Biokimia Semester 2Anonymous oyAUZoCeyNo ratings yet
- Kuliah DislipidemiaDocument45 pagesKuliah DislipidemiaPaul Behring ManurungNo ratings yet
- LIPIDS11Document6 pagesLIPIDS11gdudex118811No ratings yet
- Kuliah Dislipidemia UpdateDocument44 pagesKuliah Dislipidemia UpdateYudy Hardiyansah100% (1)
- K 30 - Kuliah Dislipidemia Update (Desktop-Doosshg's Conflicted Copy 2018-06-12)Document45 pagesK 30 - Kuliah Dislipidemia Update (Desktop-Doosshg's Conflicted Copy 2018-06-12)Reina TarihoranNo ratings yet
- Lipoprotein Disorders 2Document33 pagesLipoprotein Disorders 2Bolabo BenivoNo ratings yet
- Desirable - Less Than 200 MG/DL Borderline High Risk - 200-239 MG/DL High Risk - 240 MG/DL and OverDocument62 pagesDesirable - Less Than 200 MG/DL Borderline High Risk - 200-239 MG/DL High Risk - 240 MG/DL and OverAdib RahmanNo ratings yet
- M8 CC1 LecDocument12 pagesM8 CC1 LecNicole GarciaNo ratings yet
- New Developments in The Management of Dyslipidemia: Widjanarko. W MDDocument62 pagesNew Developments in The Management of Dyslipidemia: Widjanarko. W MDyulanda fitrianaNo ratings yet
- Drugs Affecting Lipid MetabolismDocument50 pagesDrugs Affecting Lipid MetabolismchiragcvpNo ratings yet
- Hyperlipidemia 1Document54 pagesHyperlipidemia 1MarrkNo ratings yet
- Ninja - Antihyperlipidemics PDFDocument3 pagesNinja - Antihyperlipidemics PDFErica Hyeyeon Lee100% (1)
- Lab ClassDocument23 pagesLab ClassTIPSY ANTONYNo ratings yet
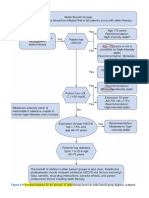
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- BBM Lipoprotein Metabolism Related DisordersDocument26 pagesBBM Lipoprotein Metabolism Related Disorderskaterina KarinaNo ratings yet
- DyslipidemiaDocument63 pagesDyslipidemiaJuhliad LebenuNo ratings yet
- DyslipidaemiaDocument34 pagesDyslipidaemiaMusfique RashidNo ratings yet
- Atherosclerosis & DyslipidemiasDocument28 pagesAtherosclerosis & DyslipidemiasTsegaye HailuNo ratings yet
- A Modern Approach To Dyslipidemia: ReviewDocument43 pagesA Modern Approach To Dyslipidemia: ReviewElberNo ratings yet
- What Is HyperlipidemiaDocument9 pagesWhat Is Hyperlipidemiaichanara100% (2)
- Chapter 24 - DylipidaemiaDocument7 pagesChapter 24 - DylipidaemiaMark Harold GonzalesNo ratings yet
- PENAFIEL M5 April2-2023Document11 pagesPENAFIEL M5 April2-2023Precious Valerie PenafielNo ratings yet
- MNT-Dislipidemia-Unja 20022019 PDFDocument48 pagesMNT-Dislipidemia-Unja 20022019 PDFAnonymous o3Q3QXENo ratings yet
- Dislipid 2 PDFDocument4 pagesDislipid 2 PDFWahyuningsih HamidNo ratings yet
- Primary Dyslipidaemias and ATS: Eliška MarklováDocument28 pagesPrimary Dyslipidaemias and ATS: Eliška MarklováSharpie Hawt'RawkStarNo ratings yet
- CC1 Intro To Lipids 2016Document60 pagesCC1 Intro To Lipids 2016Patrisha BuanNo ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Farmakoterapi HiperlipidemiaDocument123 pagesFarmakoterapi HiperlipidemiaJustian DwatamaNo ratings yet
- Familial Hyperlipidemia Type 2a - StatPearls - NCBI BookshelfDocument6 pagesFamilial Hyperlipidemia Type 2a - StatPearls - NCBI BookshelfMohammed shamiul ShahidNo ratings yet
- Lipid Disorders - AMBOSS-2Document12 pagesLipid Disorders - AMBOSS-2Mohammed shamiul ShahidNo ratings yet
- Far Eastern University - Nicanor Reyes Medical FoundationDocument2 pagesFar Eastern University - Nicanor Reyes Medical FoundationJyl Yan SelasorNo ratings yet
- ApoB 2Document7 pagesApoB 2Alex AlexNo ratings yet
- 0043 PDFDocument12 pages0043 PDFZuhdan AnnajmutstsaqibNo ratings yet
- Lab Investigations in Cardiology 22Document22 pagesLab Investigations in Cardiology 22TIPSY ANTONYNo ratings yet
- Familial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Document43 pagesFamilial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Gourav Kumar SinhaNo ratings yet
- 13 FullDocument16 pages13 FullGyse LemaNo ratings yet
- Patho Common Stuff - RobbinsDocument7 pagesPatho Common Stuff - RobbinsMaf BNo ratings yet
- High Yield AnatomyDocument7 pagesHigh Yield AnatomyMaf BNo ratings yet
- JNC8 HTNDocument2 pagesJNC8 HTNTaradifaNurInsi0% (1)
- CT - Reviewer (Revalida)Document4 pagesCT - Reviewer (Revalida)Maf BNo ratings yet
- Cruz, Leslee A. 2E - FeunrmfDocument1 pageCruz, Leslee A. 2E - FeunrmfMaf BNo ratings yet
- The Breast - Part 2 Dr. Roberto B. Acuña: Hormonal Non-HormonalDocument14 pagesThe Breast - Part 2 Dr. Roberto B. Acuña: Hormonal Non-HormonalMaf BNo ratings yet
- Nutrition FinalDocument3 pagesNutrition Finalcassy SadieNo ratings yet
- Niacin and NAD+ DeficiencyDocument19 pagesNiacin and NAD+ DeficiencykatzrayNo ratings yet
- LabelDocument9 pagesLabelNadya Alkadza100% (1)
- Nbme 22 NotesDocument1 pageNbme 22 NotesGeovy YépezNo ratings yet
- 27 - Najla - Tugas Individu PSGDocument7 pages27 - Najla - Tugas Individu PSGDIII - Gizi - NajlaNo ratings yet
- Lesson 10Document13 pagesLesson 10armin509No ratings yet
- B. Common Deficiency DiseasesDocument25 pagesB. Common Deficiency DiseasesHezmund TalonNo ratings yet
- Formulation and Evaluation of Chewable Multivitamin Tablet: Original ArticleDocument4 pagesFormulation and Evaluation of Chewable Multivitamin Tablet: Original Articlesacharum zhafirohNo ratings yet
- Jujube (Sidr) (Ber)Document29 pagesJujube (Sidr) (Ber)refiabuNo ratings yet
- Biology Form 4 Chapter 6 - VitaminsDocument3 pagesBiology Form 4 Chapter 6 - VitaminsSim Zong Xern0% (1)
- Document 2Document7 pagesDocument 2rNo ratings yet
- Vitamins and Hormones-ISC CHEMISTRY PROJECT - All About Chemistry - Reader Mode For Google Chrome™Document29 pagesVitamins and Hormones-ISC CHEMISTRY PROJECT - All About Chemistry - Reader Mode For Google Chrome™Madhav OjhaNo ratings yet
- Nutrition Lecture Notes Module 2 ContinuationDocument5 pagesNutrition Lecture Notes Module 2 ContinuationfallenNo ratings yet
- Advanced Nutritional BiochemistryDocument90 pagesAdvanced Nutritional BiochemistryAkinleye peter100% (1)
- Social Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictDocument3 pagesSocial Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictRashmi MishraNo ratings yet
- Water Soluble Vitamins Lecture For 1st Year MBBS by DR Sadia HaroonDocument67 pagesWater Soluble Vitamins Lecture For 1st Year MBBS by DR Sadia HaroonIMDCBiochem100% (2)
- Vitamin EDocument29 pagesVitamin ESiva Krishna NeppaliNo ratings yet
- Deficiency Diseases and Malnutrition GK Notes in PDFDocument5 pagesDeficiency Diseases and Malnutrition GK Notes in PDFvamsiprasannakoduruNo ratings yet
- Water Soluble VitaminsDocument10 pagesWater Soluble Vitaminsspaces queenNo ratings yet
- Vitamin DeficiencyDocument43 pagesVitamin DeficiencyAathi Pathmanathan100% (1)
- Vitamins Table FormDocument7 pagesVitamins Table FormR-Chian Jose GermanpNo ratings yet
- The Ultimate Guide To Dietary SupplementsDocument18 pagesThe Ultimate Guide To Dietary SupplementsNina VodaNo ratings yet
- Hair, Nails, and Skin: Differentiating Cutaneous Manifestations of Micronutrient DeficiencyDocument14 pagesHair, Nails, and Skin: Differentiating Cutaneous Manifestations of Micronutrient DeficiencyIrving EuanNo ratings yet
- Vintamin B3: Vitamin B3 (Niacin) Is Used Commonly To Refer To Two Different Compounds, Nicotinic Acid and NiacinamideDocument7 pagesVintamin B3: Vitamin B3 (Niacin) Is Used Commonly To Refer To Two Different Compounds, Nicotinic Acid and NiacinamideJianhua ShiNo ratings yet
- Banana Nutrition Health BenefitsDocument9 pagesBanana Nutrition Health BenefitsUmar PervezNo ratings yet
- Turmeric Nutrition FactsDocument40 pagesTurmeric Nutrition FactsUdhaya KumarNo ratings yet
- A Green Process For Niacinamide ProductionDocument301 pagesA Green Process For Niacinamide ProductionClaudia CelestinoNo ratings yet