
COVID-19 MoHP Protocol May 2020
COVID-19 MoHP Protocol May 2020
You might also like
- Nbme 27 With Answers and ExplanationsDocument15 pagesNbme 27 With Answers and ExplanationsZaid Marwan100% (2)
- BiPAP Full FlowchartDocument1 pageBiPAP Full FlowchartArjun KumarNo ratings yet
- MoHP Protocol For COVID19 November 2020Document28 pagesMoHP Protocol For COVID19 November 2020medya dostorNo ratings yet
- Covid 19 PathwayDocument17 pagesCovid 19 Pathwayferi adiantoNo ratings yet
- Aden Covid-19 Protocol 26-5-2020 (ASIA) 22-1Document14 pagesAden Covid-19 Protocol 26-5-2020 (ASIA) 22-1محمدرزازالتبعيNo ratings yet
- Advisory Antibody Testing 04042020 PDFDocument2 pagesAdvisory Antibody Testing 04042020 PDFSiddharthNo ratings yet
- Advisory To Start Rapid Antibody Based Blood Test For COVID-19 (4 April 2020)Document2 pagesAdvisory To Start Rapid Antibody Based Blood Test For COVID-19 (4 April 2020)narasimma8313No ratings yet
- Guide To COVID-19 in SKH ED: 30MAY22 Dennis CHIADocument35 pagesGuide To COVID-19 in SKH ED: 30MAY22 Dennis CHIAZainal Abidin Mohd Ruslan ShahNo ratings yet
- 3 Strengthening Referral System During COVID 19 PandemicDocument27 pages3 Strengthening Referral System During COVID 19 PandemicLapuyan Rural Health UnitNo ratings yet
- MoHP Protocol December 2021Document32 pagesMoHP Protocol December 2021Yoyo RashadNo ratings yet
- PHC ILI Guidlines COVID-19 FinalDocument4 pagesPHC ILI Guidlines COVID-19 Finalyalmas ugloNo ratings yet
- Sample Case Studies of COVID-19 in PregnancyDocument29 pagesSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNo ratings yet
- Corona Virus and PregnancyDocument17 pagesCorona Virus and PregnancyDESHVIKASH SWAINNo ratings yet
- Barnet Primary Care Pathway During Covid19 v1 PDFDocument1 pageBarnet Primary Care Pathway During Covid19 v1 PDFAndrew WilkinsonNo ratings yet
- FAM MED COVID 19 by SC Rana RojoDocument112 pagesFAM MED COVID 19 by SC Rana RojoAllene PaderangaNo ratings yet
- COVID Latest GuidelinesDocument48 pagesCOVID Latest Guidelinesarrestedinlove123No ratings yet
- SGD Fever and Chills Wrap UpDocument27 pagesSGD Fever and Chills Wrap UpNewbornMed FABELLANo ratings yet
- Coronavirus19 1Document60 pagesCoronavirus19 1bekbekk cabahugNo ratings yet
- PSMID Guidelines COVID 19 - EditedDocument8 pagesPSMID Guidelines COVID 19 - EditedIsrael H. ZantuaNo ratings yet
- Guía Rápida StanfordDocument6 pagesGuía Rápida StanfordDr. Victor Adolfo RochaNo ratings yet
- COVID-19 Protocol - MOHP 23march 2020Document4 pagesCOVID-19 Protocol - MOHP 23march 2020Sanaa SbdelghanyNo ratings yet
- Bu BudiDocument32 pagesBu Budinoi javuNo ratings yet
- Ruchi: InterpretationDocument2 pagesRuchi: InterpretationKuldeep KumarNo ratings yet
- MoH COVID 19 Protocol - V1.1 PDFDocument6 pagesMoH COVID 19 Protocol - V1.1 PDFHCX dghhqNo ratings yet
- Covid Antiviral Medications How To Prescribe Mar 10 2022Document38 pagesCovid Antiviral Medications How To Prescribe Mar 10 2022ABDULLAH SDNo ratings yet
- COVID-19 Protocol July 2022Document36 pagesCOVID-19 Protocol July 2022Mobile AsdNo ratings yet
- Tarun Kumar Report - 15012022 - 120821Document1 pageTarun Kumar Report - 15012022 - 120821navdeep madheshiyaNo ratings yet
- Bu Yovita Penanganan Medis Infeksi nCoV 05022020Document18 pagesBu Yovita Penanganan Medis Infeksi nCoV 05022020restulibrianiNo ratings yet
- Prevention of Nosocomial Covid 19 Another Challenge of The PandemicDocument2 pagesPrevention of Nosocomial Covid 19 Another Challenge of The PandemicZied FehriNo ratings yet
- Management Protocol Covid 19 V08 21-7-2020Document1 pageManagement Protocol Covid 19 V08 21-7-2020EdgarNo ratings yet
- Covid-19 Initial Triaging & Case Management ProtocolDocument24 pagesCovid-19 Initial Triaging & Case Management ProtocolDeepak SugumarNo ratings yet
- COVID Latest Guidelines-1Document48 pagesCOVID Latest Guidelines-1Digvijay ChavanNo ratings yet
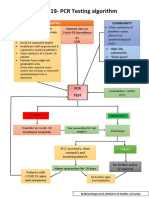
- CovidpcrtestingalgorithmDocument1 pageCovidpcrtestingalgorithmMWNo ratings yet
- Tatalaksana Kasus (13022020)Document31 pagesTatalaksana Kasus (13022020)junai arandetaNo ratings yet
- MoH COVID 19 Protocol - V1.8-1 PDFDocument13 pagesMoH COVID 19 Protocol - V1.8-1 PDFHCX dghhqNo ratings yet
- COVID-19 in Patients With HIV: Clinical Case SeriesDocument3 pagesCOVID-19 in Patients With HIV: Clinical Case SeriesPutri MaheraNo ratings yet
- Treatment Guidance For COVID-19 - 6 December 2020Document1 pageTreatment Guidance For COVID-19 - 6 December 2020meiraimNo ratings yet
- 5 Cases FungalDocument56 pages5 Cases Fungalkoteshwara raoNo ratings yet
- Covid Report PDFDocument2 pagesCovid Report PDFAthira NairNo ratings yet
- Tarun Kumar ReportDocument1 pageTarun Kumar Reportnavdeep madheshiyaNo ratings yet
- New May2020 PDFDocument7 pagesNew May2020 PDFDoctorMoodyNo ratings yet
- Covid 19 Resource GuideDocument2 pagesCovid 19 Resource GuideSenthil VelliyangiriNo ratings yet
- Covid Basics Poster v2 20211230Document2 pagesCovid Basics Poster v2 20211230Swagat MohantyNo ratings yet
- Isolation Guide enDocument24 pagesIsolation Guide enbasil aliNo ratings yet
- 7 Cases FungalDocument56 pages7 Cases Fungalkoteshwara raoNo ratings yet
- Management Protocol For Covid-19: Department of Health and Family WelfareDocument34 pagesManagement Protocol For Covid-19: Department of Health and Family Welfarechandra sekharNo ratings yet
- PROTOCOL For Management of COVID-19 Cases WB 2nd Edition.Document49 pagesPROTOCOL For Management of COVID-19 Cases WB 2nd Edition.Shahin KhanNo ratings yet
- Management of Mild Cases of COVID-19 in Low-Resource CountriesDocument2 pagesManagement of Mild Cases of COVID-19 in Low-Resource CountriesAnthony HopkinsNo ratings yet
- Saudi Moh Protocol For Patients Suspected Of/Confirmed With Covid-19Document15 pagesSaudi Moh Protocol For Patients Suspected Of/Confirmed With Covid-19AldrinNo ratings yet
- Uganda - Advanced HIV Disease - Screening ToolDocument47 pagesUganda - Advanced HIV Disease - Screening Toolithran khoNo ratings yet
- Special Coding Advice During COVID-19 Public Health EmergencyDocument31 pagesSpecial Coding Advice During COVID-19 Public Health Emergencyplayjake18No ratings yet
- The Following Guidelines Must Be Implemented:: Omicron VariantDocument13 pagesThe Following Guidelines Must Be Implemented:: Omicron VariantLdrrmo RamonNo ratings yet
- Covid-19 Inpatient Guide 092020.1Document1 pageCovid-19 Inpatient Guide 092020.1Anna JuniedNo ratings yet
- MoH Saudi Arabia COVID 19 ProtocolDocument13 pagesMoH Saudi Arabia COVID 19 Protocoladilah fazliNo ratings yet
- Covid For ClerksDocument60 pagesCovid For ClerksNehemiah FranciscoNo ratings yet
- Irfan Shaikh 38Document2 pagesIrfan Shaikh 38Altamash AnsariNo ratings yet
- Status Klinis COVID-19 Kombinasi Dengan Penyakit KardiovaskularDocument21 pagesStatus Klinis COVID-19 Kombinasi Dengan Penyakit KardiovaskularMariaAmeliaGoldieNo ratings yet
- 5908 - Muh Firdaus Kasim-Covid 19 Public Health Perspective 28032020 PDFDocument20 pages5908 - Muh Firdaus Kasim-Covid 19 Public Health Perspective 28032020 PDFDave VentraNo ratings yet
- Unified Covid-19 Algorithms: Guidelines For Primary CareDocument9 pagesUnified Covid-19 Algorithms: Guidelines For Primary Careagnes bastonNo ratings yet
- 3B - COVID-19 Update - April 2020Document40 pages3B - COVID-19 Update - April 2020Tuệ HoàngNo ratings yet
- Decision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsDocument12 pagesDecision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsPatricia Franco-VillaNo ratings yet
- NICE Way to Cure COVID -19From EverandNICE Way to Cure COVID -19Rating: 4.5 out of 5 stars4.5/5 (8)
- Oxygen ToxicityDocument4 pagesOxygen ToxicityRicard ClainkweeNo ratings yet
- Sleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongDocument6 pagesSleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongVijay KumarNo ratings yet
- The Evaluation, Diagnosis, and Treatment of The Adult Patient With Acute Hypercapnic Respiratory Failure - UpToDateDocument37 pagesThe Evaluation, Diagnosis, and Treatment of The Adult Patient With Acute Hypercapnic Respiratory Failure - UpToDateKiran AsrannaNo ratings yet
- Chapter 3Document10 pagesChapter 3rutba.ahmkhanNo ratings yet
- Oxygen Delivery NHSDocument26 pagesOxygen Delivery NHSdr satnam kaurNo ratings yet
- ARDS and Resp Failure by SardarDocument53 pagesARDS and Resp Failure by SardarQashqar & GB FolksNo ratings yet
- Respiratory Sinus ArrhythmiaDocument8 pagesRespiratory Sinus ArrhythmiaTatiana RecinosNo ratings yet
- Avoiding Common Errors in The Emergency Department-1002-1280Document280 pagesAvoiding Common Errors in The Emergency Department-1002-1280Hernando CastrillónNo ratings yet
- 2019 Article SismesxinationalcongressDocument117 pages2019 Article SismesxinationalcongresspantufoNo ratings yet
- Falla Respiratoria & Embarazo - Lapinsky 2015Document7 pagesFalla Respiratoria & Embarazo - Lapinsky 2015Fabiola Buelna GaxiolaNo ratings yet
- The Cave Divers Who Went Back For Their FriendsDocument5 pagesThe Cave Divers Who Went Back For Their FriendsRocio TobaresNo ratings yet
- Lo Tropmed 1Document49 pagesLo Tropmed 1belleNo ratings yet
- Acute Respiratory FailureDocument29 pagesAcute Respiratory FailurePurnima ChoudhuryNo ratings yet
- Modul: Intensive Care IDocument62 pagesModul: Intensive Care IHandayu GanitafuriNo ratings yet
- The Physiology of Inergen® Fire Extinguishing AgentDocument7 pagesThe Physiology of Inergen® Fire Extinguishing AgentJEAN FELLIPE BARROSNo ratings yet
- 2003, Vol.36, Issues 3, Surgery For Sleep ApneaDocument151 pages2003, Vol.36, Issues 3, Surgery For Sleep Apneamed_amitNo ratings yet
- Course Material - Breathing Exercise - For Summer 2020Document4 pagesCourse Material - Breathing Exercise - For Summer 2020emruzzamanNo ratings yet
- Ventilation Handbook WordDocument55 pagesVentilation Handbook WordHndr100% (2)
- PIIS2058534920300202Document7 pagesPIIS2058534920300202Dwi WahyudiNo ratings yet
- COPD Chronic Bronchitis EmphysemaDocument3 pagesCOPD Chronic Bronchitis EmphysemaJOHN CARLO APATANNo ratings yet
- Dr. Vernon Coleman - Masks and Mask Wearing - 100 Facts You Must Know - World Doctors AllianceDocument17 pagesDr. Vernon Coleman - Masks and Mask Wearing - 100 Facts You Must Know - World Doctors Alliancejamestahara95No ratings yet
- 281 FullDocument8 pages281 FullbcgvpilotNo ratings yet
- What Is Oxygen TheraphyDocument4 pagesWhat Is Oxygen TheraphyitsmekringNo ratings yet
- Physiology of Breathing and Respiratory Control During SleepDocument8 pagesPhysiology of Breathing and Respiratory Control During SleepAchmad Hafidz BaraqbahNo ratings yet
- Acute Respiratory FailureDocument8 pagesAcute Respiratory FailureCayunk NorlianaNo ratings yet
- Alterations in Respiratory FunctionsDocument26 pagesAlterations in Respiratory FunctionsAjeeshNo ratings yet
- Noninvasive Ventilation in Acute Respiratory Failure in Adults - UpToDateDocument27 pagesNoninvasive Ventilation in Acute Respiratory Failure in Adults - UpToDatehugo roblesNo ratings yet
- Mechanical Ventilation: Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryDocument16 pagesMechanical Ventilation: Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryGian Carlo RabagoNo ratings yet























































































Download as pdf or txt
You might also like
- Nbme 27 With Answers and ExplanationsDocument15 pagesNbme 27 With Answers and ExplanationsZaid Marwan100% (2)
- BiPAP Full FlowchartDocument1 pageBiPAP Full FlowchartArjun KumarNo ratings yet
- MoHP Protocol For COVID19 November 2020Document28 pagesMoHP Protocol For COVID19 November 2020medya dostorNo ratings yet
- Covid 19 PathwayDocument17 pagesCovid 19 Pathwayferi adiantoNo ratings yet
- Aden Covid-19 Protocol 26-5-2020 (ASIA) 22-1Document14 pagesAden Covid-19 Protocol 26-5-2020 (ASIA) 22-1محمدرزازالتبعيNo ratings yet
- Advisory Antibody Testing 04042020 PDFDocument2 pagesAdvisory Antibody Testing 04042020 PDFSiddharthNo ratings yet
- Advisory To Start Rapid Antibody Based Blood Test For COVID-19 (4 April 2020)Document2 pagesAdvisory To Start Rapid Antibody Based Blood Test For COVID-19 (4 April 2020)narasimma8313No ratings yet
- Guide To COVID-19 in SKH ED: 30MAY22 Dennis CHIADocument35 pagesGuide To COVID-19 in SKH ED: 30MAY22 Dennis CHIAZainal Abidin Mohd Ruslan ShahNo ratings yet
- 3 Strengthening Referral System During COVID 19 PandemicDocument27 pages3 Strengthening Referral System During COVID 19 PandemicLapuyan Rural Health UnitNo ratings yet
- MoHP Protocol December 2021Document32 pagesMoHP Protocol December 2021Yoyo RashadNo ratings yet
- PHC ILI Guidlines COVID-19 FinalDocument4 pagesPHC ILI Guidlines COVID-19 Finalyalmas ugloNo ratings yet
- Sample Case Studies of COVID-19 in PregnancyDocument29 pagesSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNo ratings yet
- Corona Virus and PregnancyDocument17 pagesCorona Virus and PregnancyDESHVIKASH SWAINNo ratings yet
- Barnet Primary Care Pathway During Covid19 v1 PDFDocument1 pageBarnet Primary Care Pathway During Covid19 v1 PDFAndrew WilkinsonNo ratings yet
- FAM MED COVID 19 by SC Rana RojoDocument112 pagesFAM MED COVID 19 by SC Rana RojoAllene PaderangaNo ratings yet
- COVID Latest GuidelinesDocument48 pagesCOVID Latest Guidelinesarrestedinlove123No ratings yet
- SGD Fever and Chills Wrap UpDocument27 pagesSGD Fever and Chills Wrap UpNewbornMed FABELLANo ratings yet
- Coronavirus19 1Document60 pagesCoronavirus19 1bekbekk cabahugNo ratings yet
- PSMID Guidelines COVID 19 - EditedDocument8 pagesPSMID Guidelines COVID 19 - EditedIsrael H. ZantuaNo ratings yet
- Guía Rápida StanfordDocument6 pagesGuía Rápida StanfordDr. Victor Adolfo RochaNo ratings yet
- COVID-19 Protocol - MOHP 23march 2020Document4 pagesCOVID-19 Protocol - MOHP 23march 2020Sanaa SbdelghanyNo ratings yet
- Bu BudiDocument32 pagesBu Budinoi javuNo ratings yet
- Ruchi: InterpretationDocument2 pagesRuchi: InterpretationKuldeep KumarNo ratings yet
- MoH COVID 19 Protocol - V1.1 PDFDocument6 pagesMoH COVID 19 Protocol - V1.1 PDFHCX dghhqNo ratings yet
- Covid Antiviral Medications How To Prescribe Mar 10 2022Document38 pagesCovid Antiviral Medications How To Prescribe Mar 10 2022ABDULLAH SDNo ratings yet
- COVID-19 Protocol July 2022Document36 pagesCOVID-19 Protocol July 2022Mobile AsdNo ratings yet
- Tarun Kumar Report - 15012022 - 120821Document1 pageTarun Kumar Report - 15012022 - 120821navdeep madheshiyaNo ratings yet
- Bu Yovita Penanganan Medis Infeksi nCoV 05022020Document18 pagesBu Yovita Penanganan Medis Infeksi nCoV 05022020restulibrianiNo ratings yet
- Prevention of Nosocomial Covid 19 Another Challenge of The PandemicDocument2 pagesPrevention of Nosocomial Covid 19 Another Challenge of The PandemicZied FehriNo ratings yet
- Management Protocol Covid 19 V08 21-7-2020Document1 pageManagement Protocol Covid 19 V08 21-7-2020EdgarNo ratings yet
- Covid-19 Initial Triaging & Case Management ProtocolDocument24 pagesCovid-19 Initial Triaging & Case Management ProtocolDeepak SugumarNo ratings yet
- COVID Latest Guidelines-1Document48 pagesCOVID Latest Guidelines-1Digvijay ChavanNo ratings yet
- CovidpcrtestingalgorithmDocument1 pageCovidpcrtestingalgorithmMWNo ratings yet
- Tatalaksana Kasus (13022020)Document31 pagesTatalaksana Kasus (13022020)junai arandetaNo ratings yet
- MoH COVID 19 Protocol - V1.8-1 PDFDocument13 pagesMoH COVID 19 Protocol - V1.8-1 PDFHCX dghhqNo ratings yet
- COVID-19 in Patients With HIV: Clinical Case SeriesDocument3 pagesCOVID-19 in Patients With HIV: Clinical Case SeriesPutri MaheraNo ratings yet
- Treatment Guidance For COVID-19 - 6 December 2020Document1 pageTreatment Guidance For COVID-19 - 6 December 2020meiraimNo ratings yet
- 5 Cases FungalDocument56 pages5 Cases Fungalkoteshwara raoNo ratings yet
- Covid Report PDFDocument2 pagesCovid Report PDFAthira NairNo ratings yet
- Tarun Kumar ReportDocument1 pageTarun Kumar Reportnavdeep madheshiyaNo ratings yet
- New May2020 PDFDocument7 pagesNew May2020 PDFDoctorMoodyNo ratings yet
- Covid 19 Resource GuideDocument2 pagesCovid 19 Resource GuideSenthil VelliyangiriNo ratings yet
- Covid Basics Poster v2 20211230Document2 pagesCovid Basics Poster v2 20211230Swagat MohantyNo ratings yet
- Isolation Guide enDocument24 pagesIsolation Guide enbasil aliNo ratings yet
- 7 Cases FungalDocument56 pages7 Cases Fungalkoteshwara raoNo ratings yet
- Management Protocol For Covid-19: Department of Health and Family WelfareDocument34 pagesManagement Protocol For Covid-19: Department of Health and Family Welfarechandra sekharNo ratings yet
- PROTOCOL For Management of COVID-19 Cases WB 2nd Edition.Document49 pagesPROTOCOL For Management of COVID-19 Cases WB 2nd Edition.Shahin KhanNo ratings yet
- Management of Mild Cases of COVID-19 in Low-Resource CountriesDocument2 pagesManagement of Mild Cases of COVID-19 in Low-Resource CountriesAnthony HopkinsNo ratings yet
- Saudi Moh Protocol For Patients Suspected Of/Confirmed With Covid-19Document15 pagesSaudi Moh Protocol For Patients Suspected Of/Confirmed With Covid-19AldrinNo ratings yet
- Uganda - Advanced HIV Disease - Screening ToolDocument47 pagesUganda - Advanced HIV Disease - Screening Toolithran khoNo ratings yet
- Special Coding Advice During COVID-19 Public Health EmergencyDocument31 pagesSpecial Coding Advice During COVID-19 Public Health Emergencyplayjake18No ratings yet
- The Following Guidelines Must Be Implemented:: Omicron VariantDocument13 pagesThe Following Guidelines Must Be Implemented:: Omicron VariantLdrrmo RamonNo ratings yet
- Covid-19 Inpatient Guide 092020.1Document1 pageCovid-19 Inpatient Guide 092020.1Anna JuniedNo ratings yet
- MoH Saudi Arabia COVID 19 ProtocolDocument13 pagesMoH Saudi Arabia COVID 19 Protocoladilah fazliNo ratings yet
- Covid For ClerksDocument60 pagesCovid For ClerksNehemiah FranciscoNo ratings yet
- Irfan Shaikh 38Document2 pagesIrfan Shaikh 38Altamash AnsariNo ratings yet
- Status Klinis COVID-19 Kombinasi Dengan Penyakit KardiovaskularDocument21 pagesStatus Klinis COVID-19 Kombinasi Dengan Penyakit KardiovaskularMariaAmeliaGoldieNo ratings yet
- 5908 - Muh Firdaus Kasim-Covid 19 Public Health Perspective 28032020 PDFDocument20 pages5908 - Muh Firdaus Kasim-Covid 19 Public Health Perspective 28032020 PDFDave VentraNo ratings yet
- Unified Covid-19 Algorithms: Guidelines For Primary CareDocument9 pagesUnified Covid-19 Algorithms: Guidelines For Primary Careagnes bastonNo ratings yet
- 3B - COVID-19 Update - April 2020Document40 pages3B - COVID-19 Update - April 2020Tuệ HoàngNo ratings yet
- Decision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsDocument12 pagesDecision Algorithms For The Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID - 19 PatientsPatricia Franco-VillaNo ratings yet
- NICE Way to Cure COVID -19From EverandNICE Way to Cure COVID -19Rating: 4.5 out of 5 stars4.5/5 (8)
- Oxygen ToxicityDocument4 pagesOxygen ToxicityRicard ClainkweeNo ratings yet
- Sleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongDocument6 pagesSleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongVijay KumarNo ratings yet
- The Evaluation, Diagnosis, and Treatment of The Adult Patient With Acute Hypercapnic Respiratory Failure - UpToDateDocument37 pagesThe Evaluation, Diagnosis, and Treatment of The Adult Patient With Acute Hypercapnic Respiratory Failure - UpToDateKiran AsrannaNo ratings yet
- Chapter 3Document10 pagesChapter 3rutba.ahmkhanNo ratings yet
- Oxygen Delivery NHSDocument26 pagesOxygen Delivery NHSdr satnam kaurNo ratings yet
- ARDS and Resp Failure by SardarDocument53 pagesARDS and Resp Failure by SardarQashqar & GB FolksNo ratings yet
- Respiratory Sinus ArrhythmiaDocument8 pagesRespiratory Sinus ArrhythmiaTatiana RecinosNo ratings yet
- Avoiding Common Errors in The Emergency Department-1002-1280Document280 pagesAvoiding Common Errors in The Emergency Department-1002-1280Hernando CastrillónNo ratings yet
- 2019 Article SismesxinationalcongressDocument117 pages2019 Article SismesxinationalcongresspantufoNo ratings yet
- Falla Respiratoria & Embarazo - Lapinsky 2015Document7 pagesFalla Respiratoria & Embarazo - Lapinsky 2015Fabiola Buelna GaxiolaNo ratings yet
- The Cave Divers Who Went Back For Their FriendsDocument5 pagesThe Cave Divers Who Went Back For Their FriendsRocio TobaresNo ratings yet
- Lo Tropmed 1Document49 pagesLo Tropmed 1belleNo ratings yet
- Acute Respiratory FailureDocument29 pagesAcute Respiratory FailurePurnima ChoudhuryNo ratings yet
- Modul: Intensive Care IDocument62 pagesModul: Intensive Care IHandayu GanitafuriNo ratings yet
- The Physiology of Inergen® Fire Extinguishing AgentDocument7 pagesThe Physiology of Inergen® Fire Extinguishing AgentJEAN FELLIPE BARROSNo ratings yet
- 2003, Vol.36, Issues 3, Surgery For Sleep ApneaDocument151 pages2003, Vol.36, Issues 3, Surgery For Sleep Apneamed_amitNo ratings yet
- Course Material - Breathing Exercise - For Summer 2020Document4 pagesCourse Material - Breathing Exercise - For Summer 2020emruzzamanNo ratings yet
- Ventilation Handbook WordDocument55 pagesVentilation Handbook WordHndr100% (2)
- PIIS2058534920300202Document7 pagesPIIS2058534920300202Dwi WahyudiNo ratings yet
- COPD Chronic Bronchitis EmphysemaDocument3 pagesCOPD Chronic Bronchitis EmphysemaJOHN CARLO APATANNo ratings yet
- Dr. Vernon Coleman - Masks and Mask Wearing - 100 Facts You Must Know - World Doctors AllianceDocument17 pagesDr. Vernon Coleman - Masks and Mask Wearing - 100 Facts You Must Know - World Doctors Alliancejamestahara95No ratings yet
- 281 FullDocument8 pages281 FullbcgvpilotNo ratings yet
- What Is Oxygen TheraphyDocument4 pagesWhat Is Oxygen TheraphyitsmekringNo ratings yet
- Physiology of Breathing and Respiratory Control During SleepDocument8 pagesPhysiology of Breathing and Respiratory Control During SleepAchmad Hafidz BaraqbahNo ratings yet
- Acute Respiratory FailureDocument8 pagesAcute Respiratory FailureCayunk NorlianaNo ratings yet
- Alterations in Respiratory FunctionsDocument26 pagesAlterations in Respiratory FunctionsAjeeshNo ratings yet
- Noninvasive Ventilation in Acute Respiratory Failure in Adults - UpToDateDocument27 pagesNoninvasive Ventilation in Acute Respiratory Failure in Adults - UpToDatehugo roblesNo ratings yet
- Mechanical Ventilation: Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryDocument16 pagesMechanical Ventilation: Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryGian Carlo RabagoNo ratings yet