Download as docx, pdf, or txt
You might also like
- Assignment: Case StudyDocument3 pagesAssignment: Case StudyHamza Haroon67% (3)
- Classification of Bi SyndromeDocument7 pagesClassification of Bi Syndromecharrie7100% (1)
- The Education of Nurses On The Leading Edge of TransformationDocument31 pagesThe Education of Nurses On The Leading Edge of TransformationDip Ayan M100% (2)
- Open Book Examination: NeboshDocument8 pagesOpen Book Examination: NeboshZahir KhanNo ratings yet
- Genetic Counselling: Submitted By: Jinson Raju 3 YearDocument6 pagesGenetic Counselling: Submitted By: Jinson Raju 3 YearJanet VargheseNo ratings yet
- Alopecia 160716052003Document26 pagesAlopecia 160716052003AbirajanNo ratings yet
- Lindbergh School District Directory 2013-14Document24 pagesLindbergh School District Directory 2013-14timesnewspapersNo ratings yet
- Care of Unconscious ClientDocument27 pagesCare of Unconscious ClientDonelie Kay Tapel AsanzaNo ratings yet
- Care of Unconscious PatientDocument7 pagesCare of Unconscious PatientSallieNo ratings yet
- Care of Unconscious PatientDocument5 pagesCare of Unconscious PatientRuchika Kaushal67% (3)
- Unconsciousness: Anil PatidarDocument29 pagesUnconsciousness: Anil Patidarjinal sutharNo ratings yet
- UnconsciousnessDocument16 pagesUnconsciousnessAkhilesh BabuNo ratings yet
- Care of Unconscious PatientDocument34 pagesCare of Unconscious PatientPoova RagavanNo ratings yet
- CH 1 Sociolgy For BSC Nursing StudentsDocument16 pagesCH 1 Sociolgy For BSC Nursing Students7G LearningNo ratings yet
- Presentation On Health AssessmentDocument12 pagesPresentation On Health AssessmentSimran ChauhanNo ratings yet
- Coping With Loss Griving 0 DeathDocument16 pagesCoping With Loss Griving 0 DeathSandhya Gupta100% (1)
- Mobility and ImmobilityDocument4 pagesMobility and ImmobilityChin ChanNo ratings yet
- Pulse Oximetry IDocument4 pagesPulse Oximetry IFriends Forever100% (1)
- Health Promotion and Primary Health CareDocument51 pagesHealth Promotion and Primary Health CareBhawna JoshiNo ratings yet
- l4 Care of Unconscious PatientsDocument3 pagesl4 Care of Unconscious PatientsMuhammad HaziqNo ratings yet
- ANMDocument2 pagesANMShreyas Walvekar100% (1)
- Assesment For Burns and Fluid Calculation PDFDocument10 pagesAssesment For Burns and Fluid Calculation PDFRagaviNo ratings yet
- Restraining Procedure: General Principles For Use of RestraintsDocument10 pagesRestraining Procedure: General Principles For Use of RestraintsHardeep KaurNo ratings yet
- Care of Dying PatientDocument27 pagesCare of Dying PatientAbinaya Ranganathan100% (1)
- Comfortdevices15 9 14 150627120352 Lva1 App6891Document38 pagesComfortdevices15 9 14 150627120352 Lva1 App6891SILUVERU SALOMINo ratings yet
- Cpms College of Nursing: Assignment ON Colonic IrrigationDocument3 pagesCpms College of Nursing: Assignment ON Colonic IrrigationAmy Lalringhluani ChhakchhuakNo ratings yet
- Fundamental of NursingDocument1 pageFundamental of Nursingioana_ciobincanNo ratings yet
- Lumber PDFDocument13 pagesLumber PDFPrasann RoyNo ratings yet
- Diarrhea CPDocument8 pagesDiarrhea CPAsma SaleemNo ratings yet
- Communication: DefinitionDocument18 pagesCommunication: Definitionannu panchalNo ratings yet
- NCP Self Care DeficitDocument15 pagesNCP Self Care DeficitSkye M. PetersNo ratings yet
- Application of OremDocument19 pagesApplication of OremBhekti ImansariNo ratings yet
- Pulse OximetryDocument3 pagesPulse OximetryJanna Favila100% (3)
- Steam InhalationDocument17 pagesSteam InhalationRaju Teach Kaps100% (1)
- Annotated BibliographyDocument2 pagesAnnotated Bibliographyrajwadi suzyNo ratings yet
- Characteristics of PerceptionDocument3 pagesCharacteristics of PerceptiontanmyNo ratings yet
- Cne Seminar PDFDocument58 pagesCne Seminar PDFJoseph John CrastoNo ratings yet
- Bandaging: Presented By: Sumati Singh M. Sc. Nursing 1 YearDocument35 pagesBandaging: Presented By: Sumati Singh M. Sc. Nursing 1 YearNedhi Singh100% (2)
- Range of Motion Exercises: in HealthDocument8 pagesRange of Motion Exercises: in HealthCagabcab Canibel Melany100% (1)
- Nasogastric Tube Insertion and Nasogastric FeedingDocument25 pagesNasogastric Tube Insertion and Nasogastric FeedingBasant karnNo ratings yet
- Worm InfestationDocument4 pagesWorm InfestationSachin Dwivedi100% (3)
- Ethical and Legal Issues in Critical Care NursingDocument6 pagesEthical and Legal Issues in Critical Care NursingAsna FasilNo ratings yet
- Glaucoma: DefinitionDocument5 pagesGlaucoma: DefinitionDani PhilipNo ratings yet
- Care of Terminally IllDocument38 pagesCare of Terminally IllsalmanhabeebekNo ratings yet
- Indigenoussystemofmedicine 190329102338Document27 pagesIndigenoussystemofmedicine 190329102338Shilu Mathai PappachanNo ratings yet
- HIV CounsellingDocument14 pagesHIV CounsellingEldho SabuNo ratings yet
- Health Assessment ON Genito Urinary System: Submitted To: Submitted byDocument16 pagesHealth Assessment ON Genito Urinary System: Submitted To: Submitted byAnanthibalaNo ratings yet
- Role Av Aids in Clinical TeachingDocument16 pagesRole Av Aids in Clinical Teachingtankmp100% (1)
- Assignment On Neurological AssessmentDocument20 pagesAssignment On Neurological AssessmentSumandeep KaurNo ratings yet
- Mohd Rafi'uddin Hamidon 01200910 0070Document13 pagesMohd Rafi'uddin Hamidon 01200910 0070Mohd Rafi50% (2)
- Sensory Deprivation.Document7 pagesSensory Deprivation.KJ Bindu100% (1)
- Thoracentesis IntroductionDocument8 pagesThoracentesis Introductionjyoti singhNo ratings yet
- Evolutioon of Nursing ResearchDocument28 pagesEvolutioon of Nursing ResearchLorelie AsisNo ratings yet
- Assignment On Family Welfare-1Document5 pagesAssignment On Family Welfare-1kamini ChoudharyNo ratings yet
- Pprinciples & Techniques of CouncellingDocument6 pagesPprinciples & Techniques of CouncellingAru Verma100% (1)
- Epidemiological Theory Ppt-1Document64 pagesEpidemiological Theory Ppt-1solomon rimamchirikaNo ratings yet
- Treatment of Minor AilmentsDocument43 pagesTreatment of Minor AilmentsVidhya RaniNo ratings yet
- Abdominal ParacentesisDocument14 pagesAbdominal ParacentesisManisha Thakur100% (1)
- First Aid Management For Falls and HangingDocument4 pagesFirst Aid Management For Falls and HangingAnn Merlin JobinNo ratings yet
- Retinal DetachmentDocument7 pagesRetinal Detachmentjay dewanagnNo ratings yet
- 4 Basic Element For Normal MovementDocument17 pages4 Basic Element For Normal MovementKwai Fong ChanNo ratings yet
- Careofanunconciouspatient 180329170925Document37 pagesCareofanunconciouspatient 180329170925Ann Merlin JobinNo ratings yet
- Nursing Intervention During Emergency Situation: College of Nursing and Allied Health ServicesDocument52 pagesNursing Intervention During Emergency Situation: College of Nursing and Allied Health ServicesShella Mae LineNo ratings yet
- 1 Final Bedsidemngtofpt 190213111618 1Document17 pages1 Final Bedsidemngtofpt 190213111618 1Chirag ParmarNo ratings yet
- Critical Care NursingDocument41 pagesCritical Care NursingAbirajan50% (2)
- Initial Evaluation Pneumothorax Tension Pneumo Open Pneumo Haemothorax Contusion Rib Fracture / Flail Aortic Injury Chest DrainsDocument12 pagesInitial Evaluation Pneumothorax Tension Pneumo Open Pneumo Haemothorax Contusion Rib Fracture / Flail Aortic Injury Chest DrainsAbirajanNo ratings yet
- Demonstration ON Haemodialysis: Submitted ToDocument46 pagesDemonstration ON Haemodialysis: Submitted ToAbirajanNo ratings yet
- Healthcaredeliverysystem 161101092618 PDFDocument33 pagesHealthcaredeliverysystem 161101092618 PDFAbirajanNo ratings yet
- Health Care Delivery System in India: By. Kailash NagarDocument34 pagesHealth Care Delivery System in India: By. Kailash NagarAbirajanNo ratings yet
- Maternalandchildhealth 170107033715 PDFDocument275 pagesMaternalandchildhealth 170107033715 PDFAbirajanNo ratings yet
- Understanding The Gallbladder and BileDocument10 pagesUnderstanding The Gallbladder and BileAbirajanNo ratings yet
- Cough: R.Rajalakshmi MSC (N) Medical&Surgical NursingDocument12 pagesCough: R.Rajalakshmi MSC (N) Medical&Surgical NursingAbirajanNo ratings yet
- What Is A Fever?: Cough Sore Throat Fatigue Chills NauseaDocument10 pagesWhat Is A Fever?: Cough Sore Throat Fatigue Chills NauseaAbirajanNo ratings yet
- Health Care Delivery System in India: By. Kailash NagarDocument34 pagesHealth Care Delivery System in India: By. Kailash NagarAbirajanNo ratings yet
- Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS)Document28 pagesHuman Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS)AbirajanNo ratings yet
- Counselling in Hiv/AidsDocument9 pagesCounselling in Hiv/AidsAbirajanNo ratings yet
- A Study To Assess The Knowledge, Attitude and Practices On Optional Vaccines Among Health Care Personnel in Pondicherry Institute of Medical SciencesDocument10 pagesA Study To Assess The Knowledge, Attitude and Practices On Optional Vaccines Among Health Care Personnel in Pondicherry Institute of Medical SciencesAbirajanNo ratings yet
- Nursing Management of Patient With Respiratory ProblemsDocument151 pagesNursing Management of Patient With Respiratory ProblemsAbirajan100% (3)
- Abirajan 2nd YearDocument23 pagesAbirajan 2nd YearAbirajanNo ratings yet
- First Year M.Sc. Nursing, Bapuji College of Nursing, Davangere - 4, KarnatakaDocument14 pagesFirst Year M.Sc. Nursing, Bapuji College of Nursing, Davangere - 4, KarnatakaAbirajanNo ratings yet
- AsthmaDocument10 pagesAsthmaAbirajanNo ratings yet
- DM AgntDocument18 pagesDM AgntAbirajanNo ratings yet
- F Template - Minor Quarantine Letter For Covid Close Contact - 09.03.2021Document2 pagesF Template - Minor Quarantine Letter For Covid Close Contact - 09.03.2021WXMINo ratings yet
- Medical Surgical Nursing Care 3rd Edition Burke Test BankDocument8 pagesMedical Surgical Nursing Care 3rd Edition Burke Test BankMatthew Song100% (43)
- IKDRC Class-II, III 03-2023Document4 pagesIKDRC Class-II, III 03-2023GudellikiritibabuNo ratings yet
- Homoeopathic & Biochemic Instant PrescriberDocument369 pagesHomoeopathic & Biochemic Instant Prescriberdevilcobra68No ratings yet
- Unit 3Document4 pagesUnit 3api-439595804No ratings yet
- Vitamins To CLEAN Your FATTY LIVERDocument5 pagesVitamins To CLEAN Your FATTY LIVERNiloufar GholamipourNo ratings yet
- Semi Detailed Lesson PlanDocument6 pagesSemi Detailed Lesson PlanVILLANUEVA CHADWICKNo ratings yet
- CHNDocument6 pagesCHNhelloaNo ratings yet
- Roche Et Al. 2017 Faltering GrowthDocument6 pagesRoche Et Al. 2017 Faltering GrowthSatesh BalachantharNo ratings yet
- W Advantage VolunteerDocument2 pagesW Advantage VolunteerLinh Ngô ThịNo ratings yet
- Types/Classification and Dichotomies: ResearchDocument21 pagesTypes/Classification and Dichotomies: ResearchAdrian Baguna MontemorNo ratings yet
- Alternative Work Scheme vs. On Site Labor PhilippinesDocument3 pagesAlternative Work Scheme vs. On Site Labor PhilippinesLayaDioknoNo ratings yet
- Chapter 2 - Market Analysis - Group 2Document26 pagesChapter 2 - Market Analysis - Group 2Allan AntonioNo ratings yet
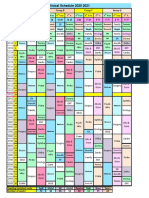
- R Schedule 2020 2021Document1 pageR Schedule 2020 2021Mohammed AhmedNo ratings yet
- Leave Fat Kids AloneDocument3 pagesLeave Fat Kids Alonesandy blehNo ratings yet
- Tinea CapitisDocument7 pagesTinea CapitiswinNo ratings yet
- Physiological, Biomechanical and Medical Aspects of Soldier Load CarriageDocument20 pagesPhysiological, Biomechanical and Medical Aspects of Soldier Load CarriageAnonymous dmhNTyNo ratings yet
- Purpose: Premier Plastic Production Company Sop For Emergency Response Plan & PreparednessDocument19 pagesPurpose: Premier Plastic Production Company Sop For Emergency Response Plan & Preparednessimranul haqNo ratings yet
- MYTHDocument6 pagesMYTHCherian MominNo ratings yet
- Gregorio, Forgive Us All: Community Health Nursing 1 Activity #1Document2 pagesGregorio, Forgive Us All: Community Health Nursing 1 Activity #1Cacamo Rexell-anNo ratings yet
- Economic Issues - CABUDSANDocument3 pagesEconomic Issues - CABUDSANSolah CabudsanNo ratings yet
- Historia de La OrtodonciaDocument9 pagesHistoria de La Ortodonciacarmonao.carina94No ratings yet
- Wolford EDM511 Case 4Document10 pagesWolford EDM511 Case 4geraldwolford1No ratings yet
- 21 Advanced Supplements Antihistamines Mast Cell StabilizersDocument18 pages21 Advanced Supplements Antihistamines Mast Cell Stabilizersdarija_ilic100% (1)
- What Is A Competent TeacherDocument2 pagesWhat Is A Competent TeacherJoy Dacuan100% (2)
- CHN - Nursing ConceptsDocument5 pagesCHN - Nursing ConceptsJessa Mae BarquillaNo ratings yet