Download as doc, pdf, or txt
You might also like
- Critical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFDocument335 pagesCritical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFSami Atawi100% (1)
- Guidelines For The Design and Construction of Health Care FacilitiesDocument370 pagesGuidelines For The Design and Construction of Health Care Facilitiesmasoodae94% (16)
- Final HR Manual PDFDocument31 pagesFinal HR Manual PDFdubaisrinivasulu100% (1)
- Consensus Statement On The Early Management of Crush Injury and Prevention of Crush SyndromeDocument8 pagesConsensus Statement On The Early Management of Crush Injury and Prevention of Crush SyndromeHaris SahirulNo ratings yet
- Trauma: Submitted To Mrs. Meenal Sharma Assistant Professor Presented by A Ms - Nisha Kaushik MSC Nursing Ist YearDocument24 pagesTrauma: Submitted To Mrs. Meenal Sharma Assistant Professor Presented by A Ms - Nisha Kaushik MSC Nursing Ist YearIshaBrijeshSharmaNo ratings yet
- Askep Luka BakarDocument59 pagesAskep Luka BakarRahmiwulandariNo ratings yet
- Presentation MulkishkoDocument3 pagesPresentation Mulkishkonmammadova04No ratings yet
- Polytrauma ManagementDocument70 pagesPolytrauma ManagementStar Cruise88% (8)
- Thoracic Trauma 7Document25 pagesThoracic Trauma 7zerish0208No ratings yet
- Official Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedDocument24 pagesOfficial Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedJéssica SantosNo ratings yet
- Consensus On Crush1Document7 pagesConsensus On Crush1Erwin CandraNo ratings yet
- Transport Injuries: DR Mohd Kaleem Khan Assistant Professor Department of Forensic Medicine J.N.M.C.H., A.M.U., AligarhDocument34 pagesTransport Injuries: DR Mohd Kaleem Khan Assistant Professor Department of Forensic Medicine J.N.M.C.H., A.M.U., AligarhKaleem KhanNo ratings yet
- Askep Luka BakarDocument59 pagesAskep Luka BakarRahmiwulandariNo ratings yet
- Preventable Death: Dco: DR Thit Lwin School of Medicine UMSDocument56 pagesPreventable Death: Dco: DR Thit Lwin School of Medicine UMSStar CruiseNo ratings yet
- Pathophysiology of Traumatic Shock: International Traumacare (Itaccs)Document4 pagesPathophysiology of Traumatic Shock: International Traumacare (Itaccs)Irina OdajiuNo ratings yet
- Critical Care and Management of Penetrating and Blunt Trauma in Siberian HuskyDocument6 pagesCritical Care and Management of Penetrating and Blunt Trauma in Siberian Huskytmi500558No ratings yet
- 112 - Prone Position1Document6 pages112 - Prone Position1Chaya RaghuNo ratings yet
- Thoracic Vascular TraumaDocument24 pagesThoracic Vascular TraumaKezia TambunanNo ratings yet
- OrthopaedicsDocument19 pagesOrthopaedicsYavani KulasinghamNo ratings yet
- 7 - Hemodynamic Disorders ShockDocument21 pages7 - Hemodynamic Disorders ShockShna SaadiNo ratings yet
- 1.1 Exposure To MicrogravityDocument19 pages1.1 Exposure To MicrogravityNujella BalajiNo ratings yet
- Lecture 1Document7 pagesLecture 1aemad2096No ratings yet
- Blast Injuries & Gunshot WoundsDocument93 pagesBlast Injuries & Gunshot WoundsdocpreetiNo ratings yet
- Penetrating Chest Trauma PDFDocument5 pagesPenetrating Chest Trauma PDFFerina FernandaNo ratings yet
- Blast InjuriesDocument17 pagesBlast InjuriesRoman MamunNo ratings yet
- RESUME STROKE and SPINAL CORD INJURYDocument8 pagesRESUME STROKE and SPINAL CORD INJURYYopy OctavianaNo ratings yet
- European Course Trauma CareDocument7 pagesEuropean Course Trauma CareYaclinNo ratings yet
- Postgrad Med J 2005 Pope 309 14Document9 pagesPostgrad Med J 2005 Pope 309 14Steven LiaNo ratings yet
- Damage Control SurgeryDocument68 pagesDamage Control SurgeryMAMA LALANo ratings yet
- Trauma 1Document45 pagesTrauma 1Abdul HaiNo ratings yet
- Advanced Trauma and Life Support (ATLS) : EpidemiologyDocument7 pagesAdvanced Trauma and Life Support (ATLS) : EpidemiologyMohamed FarahatNo ratings yet
- 13.1 Basic Trauma Life SupportDocument13 pages13.1 Basic Trauma Life Supportrhamadani.farahNo ratings yet
- Complications of FracturesDocument19 pagesComplications of Fracturesمحمد رأفتNo ratings yet
- JRNL-Responding To Trauma Your Priorities in The First HourDocument8 pagesJRNL-Responding To Trauma Your Priorities in The First HourArs MoriendiNo ratings yet
- IM361B-PathPhysio Orals 2020Document95 pagesIM361B-PathPhysio Orals 2020Mi PatelNo ratings yet
- Osifo Multiple Injured PXDocument81 pagesOsifo Multiple Injured PXOsifo EmmanuelNo ratings yet
- Postoperative ComplicationsDocument43 pagesPostoperative ComplicationsAyuub AbdirizakNo ratings yet
- Decompression IllnessDocument12 pagesDecompression Illnesstonylee24No ratings yet
- Initial Management of The Trauma PatientDocument124 pagesInitial Management of The Trauma PatientdanocprexoidNo ratings yet
- LP Surgery ChestDocument6 pagesLP Surgery Chestangelmd83No ratings yet
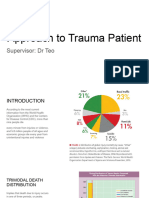
- Approach To Trauma PatientDocument36 pagesApproach To Trauma PatientTitusNo ratings yet
- Ch15.Polytrauma PatientDocument10 pagesCh15.Polytrauma PatientGibranKashogiNo ratings yet
- Traumatic AsphyxiaDocument15 pagesTraumatic AsphyxiaAnil AggrawalNo ratings yet
- Emergency Anaesthetic Management of Extensive Thoracic TraumaDocument7 pagesEmergency Anaesthetic Management of Extensive Thoracic TraumaYoz MpNo ratings yet
- Anesthesia For Thoracic Trauma - OpenAnesthesiaDocument7 pagesAnesthesia For Thoracic Trauma - OpenAnesthesiaReddyNo ratings yet
- Management of Poly Traumatized Patient-1Document20 pagesManagement of Poly Traumatized Patient-1Taha Al-morsiNo ratings yet
- Pelvic Trauma Final 210409Document8 pagesPelvic Trauma Final 210409Dwi ApriliziaNo ratings yet
- Crush InjuryDocument8 pagesCrush Injuryfadhil03No ratings yet
- Terapi Caritan Pada TraumaDocument4 pagesTerapi Caritan Pada TraumaChandra HartonoNo ratings yet
- Br. J. Anaesth. 2012 Dutton I39 46Document8 pagesBr. J. Anaesth. 2012 Dutton I39 46fitrah fajrianiNo ratings yet
- Anesthesia For Multiple Trauma IntroductionDocument126 pagesAnesthesia For Multiple Trauma IntroductionabdishakurNo ratings yet
- Unit 4 Nursing Care of Clients With Musculoskeletal DisordersDocument100 pagesUnit 4 Nursing Care of Clients With Musculoskeletal DisordersE. Tito Julianda SinagaNo ratings yet
- Anesthesia For The Trauma PatientDocument48 pagesAnesthesia For The Trauma PatientÐr SalmaNo ratings yet
- Limb AmputationDocument97 pagesLimb AmputationSatya Prakash TiwariNo ratings yet
- Chylothorax: Aetiology, Diagnosis and Therapeutic Options: Respiratory Medicine September 2009Document9 pagesChylothorax: Aetiology, Diagnosis and Therapeutic Options: Respiratory Medicine September 2009Kessi VikaneswariNo ratings yet
- Approach To The Patient With Shock: Section 2Document13 pagesApproach To The Patient With Shock: Section 2Akriti GuptaNo ratings yet
- Trauma Nursing IntroductionDocument12 pagesTrauma Nursing Introductionanimesh pandaNo ratings yet
- Polytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaDocument57 pagesPolytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaAbuhafezbaka100% (1)
- Shock - StatPearls - NCBI BookshelfDocument5 pagesShock - StatPearls - NCBI BookshelfSYAFIRA LAILA NURULITANo ratings yet
- Musculoskeletal TrumaDocument30 pagesMusculoskeletal TrumaadnanreshunNo ratings yet
- Radiofrequency Cetap eDocument4 pagesRadiofrequency Cetap ematameaNo ratings yet
- Bone TBCDocument26 pagesBone TBCmatameaNo ratings yet
- Bone TumorsDocument29 pagesBone TumorsmatameaNo ratings yet
- Chelt TherapyDocument2 pagesChelt TherapymatameaNo ratings yet
- ACL RehabDocument8 pagesACL RehabmatameaNo ratings yet
- Physiotherapy Rehabilitation Guidelines - Knee ArthrosDocument7 pagesPhysiotherapy Rehabilitation Guidelines - Knee ArthrosmatameaNo ratings yet
- Acl Rehab ProtocolDocument35 pagesAcl Rehab Protocolmatamea100% (3)
- Fisioterapia en AvmDocument13 pagesFisioterapia en Avmapi-326940690No ratings yet
- Bibliography (Critical Care Nursing)Document2 pagesBibliography (Critical Care Nursing)bijoiiNo ratings yet
- Intensive Care NursesDocument15 pagesIntensive Care NursesUlysses GamayonNo ratings yet
- Qualitative ResearchDocument9 pagesQualitative ResearchGideon M KimariNo ratings yet
- Moduevo Ceiling Supply Units Accessories Catalog BrochureDocument32 pagesModuevo Ceiling Supply Units Accessories Catalog BrochureEinstein A. MustafaNo ratings yet
- Curriculum Vitae: Sweety.P.PaulDocument4 pagesCurriculum Vitae: Sweety.P.PaulAbhilashPaulNo ratings yet
- Ventilator-Associated Pneumonia - Risk Factors & Prevention (Beth Augustyn)Document8 pagesVentilator-Associated Pneumonia - Risk Factors & Prevention (Beth Augustyn)ariepitonoNo ratings yet
- Vital Signs: Valid Indicators To Assess Pain in Intensive Care Unit Patients? An Observational, Descriptive StudyDocument7 pagesVital Signs: Valid Indicators To Assess Pain in Intensive Care Unit Patients? An Observational, Descriptive Studybardah wasalamahNo ratings yet
- Therapeutic Nursing InterventionsDocument2 pagesTherapeutic Nursing Interventionsapi-539369902No ratings yet
- Tormax Product Catalog Usa - 812Document8 pagesTormax Product Catalog Usa - 812dennys pradanaNo ratings yet
- Alvin Timbancaya, MD: ClinicsDocument2 pagesAlvin Timbancaya, MD: ClinicsRhena May AdoNo ratings yet
- Gyn - DelivaryDocument1 pageGyn - DelivaryRakshan Farm FreshNo ratings yet
- Clinical Practice Guidelines For The Sustained Use of Sedatives and Analgesics in The Critically Ill AdultDocument23 pagesClinical Practice Guidelines For The Sustained Use of Sedatives and Analgesics in The Critically Ill AdultMontse Gorchs MolistNo ratings yet
- Reinhardt Ryann ResumeDocument1 pageReinhardt Ryann Resumeapi-639569078No ratings yet
- DNP Project Manuscript eDocument71 pagesDNP Project Manuscript eapi-577634408100% (1)
- iHFG Part C Space Standards DimensionsDocument7 pagesiHFG Part C Space Standards DimensionsShalini MinnaNo ratings yet
- Medical English VocabularyDocument21 pagesMedical English VocabularyGil Ruano100% (2)
- Resume Uchealth DenverDocument2 pagesResume Uchealth Denverapi-356240113No ratings yet
- INTENSIVE CARE UNIT Gurugram Civil HospitalDocument7 pagesINTENSIVE CARE UNIT Gurugram Civil HospitalOmprakash Sundrani100% (1)
- Tape: A Dirty Business: by Steve Bierman, MDDocument11 pagesTape: A Dirty Business: by Steve Bierman, MDshinichi_kudoNo ratings yet
- Hospital Training Report NewDocument30 pagesHospital Training Report NewOMR XEROXNo ratings yet
- Case Study PDFDocument8 pagesCase Study PDFSonu KumawatNo ratings yet
- 03 BasicsDocument12 pages03 BasicsjosuanvictorNo ratings yet
- Communication Skills and Ethics in Medical PracticeDocument43 pagesCommunication Skills and Ethics in Medical PracticeRaihanShaheedNo ratings yet
- Supplies Estimating Needs 1. Analyzing Program NeedsDocument9 pagesSupplies Estimating Needs 1. Analyzing Program Needsloveseeker06No ratings yet
- Parashospitaltriff PDFDocument96 pagesParashospitaltriff PDFBajane wala baba बजाने वाला बाबाNo ratings yet
- Alex Hardin Resume 2015Document3 pagesAlex Hardin Resume 2015api-306883462No ratings yet