Download as pdf or txt
You might also like
- Food DesertsDocument4 pagesFood Desertsapi-373103187No ratings yet
- En V50n4a06 PDFDocument8 pagesEn V50n4a06 PDFmeriza dahliaNo ratings yet
- Quality of Life Patients With Ulcus DiabeticDocument4 pagesQuality of Life Patients With Ulcus DiabeticNadiaRashyaNo ratings yet
- Calidad de Vida en Pacientes Con Disfagia Neurogénica (Quality of Life in Patients With Neurogenic Dysphagia)Document7 pagesCalidad de Vida en Pacientes Con Disfagia Neurogénica (Quality of Life in Patients With Neurogenic Dysphagia)Rodrigo VillasecaNo ratings yet
- Quality of Life and People Living With AIDS: Relationship With Sociodemographic and Health AspectsDocument9 pagesQuality of Life and People Living With AIDS: Relationship With Sociodemographic and Health AspectsCyril Jane Caanyagan AcutNo ratings yet
- Impact of Diabetic Foot and Others Comorbidities On The Quality of Life of Diabetic Patients Monitored at A Specialized Outpatient ClinicDocument10 pagesImpact of Diabetic Foot and Others Comorbidities On The Quality of Life of Diabetic Patients Monitored at A Specialized Outpatient ClinicAyu SudiantariNo ratings yet
- BrazJOralSci 2013 Vol12 Issue1 p5 10Document6 pagesBrazJOralSci 2013 Vol12 Issue1 p5 10Taufiqurrahman Abdul DjabbarNo ratings yet
- Qualidade de Vida Das Pessoas Com Diabetes MellitusDocument8 pagesQualidade de Vida Das Pessoas Com Diabetes MellitusKIYOSHI FERREIRA FUKUTANINo ratings yet
- Association Between Resilience and Quality of Life in Patients With Colon CancerDocument7 pagesAssociation Between Resilience and Quality of Life in Patients With Colon CancerICR CONSULTORESNo ratings yet
- Factors Associated To Oral Health Related Quality of Life in Patients With DiabetesDocument19 pagesFactors Associated To Oral Health Related Quality of Life in Patients With DiabeteseveliiiinNo ratings yet
- Obezitatea La Copii Si Boala ParodontalaDocument8 pagesObezitatea La Copii Si Boala ParodontalaLavinia PascuNo ratings yet
- Artigo Base 4Document8 pagesArtigo Base 4Cleo AlvesNo ratings yet
- 1.jurnal AsliDocument7 pages1.jurnal AsliWaode RadmilaNo ratings yet
- Body Mass IndexDocument6 pagesBody Mass Indexayu yuliantiNo ratings yet
- The Relationship Between Periodontal Disease and Public Health: A Population-Based StudyDocument6 pagesThe Relationship Between Periodontal Disease and Public Health: A Population-Based StudyHtet AungNo ratings yet
- Mellitus Mellitus Mellitus Mellitus MellitusDocument7 pagesMellitus Mellitus Mellitus Mellitus MellitusDjoko PriyonoNo ratings yet
- The Effect of Depression On The Quality 0f Life of Patient With Cervical Cancer at Dr. Moewardi Hospital in SurakartaDocument8 pagesThe Effect of Depression On The Quality 0f Life of Patient With Cervical Cancer at Dr. Moewardi Hospital in SurakartaEndahNo ratings yet
- Prevalence of Orthorexia Nervosa in University Students and Its Relationship With Psychopathological Aspects of Eating Behaviour DisordersDocument8 pagesPrevalence of Orthorexia Nervosa in University Students and Its Relationship With Psychopathological Aspects of Eating Behaviour DisordersSAMARPITANo ratings yet
- Original Article: The Influence of Hypertension On Quality of LifeDocument11 pagesOriginal Article: The Influence of Hypertension On Quality of LifeFadel TrianzahNo ratings yet
- Quality of Life in Patients With Neurogenic DysphagiaDocument8 pagesQuality of Life in Patients With Neurogenic DysphagiaDaniela OrtizNo ratings yet
- Disease Specific Knowledge and Lifestyle Behavior in Patients With Diabetes Mellitus 2016 Obesity MedicineDocument4 pagesDisease Specific Knowledge and Lifestyle Behavior in Patients With Diabetes Mellitus 2016 Obesity MedicineLiaAriestaNo ratings yet
- 29 110 3 PBDocument9 pages29 110 3 PBWidia WidanaNo ratings yet
- 2019-Emociones Pensamientos Experiencias en DM PDFDocument9 pages2019-Emociones Pensamientos Experiencias en DM PDFPsico AstralNo ratings yet
- Jurnal LepraDocument7 pagesJurnal LepraDipa Zoda HelfandoNo ratings yet
- Diabetes Distress Paper EfmjDocument16 pagesDiabetes Distress Paper EfmjAhmed NabilNo ratings yet
- Assessment of The Perceived Quality of Life of Non Insulin Dependent Diabetic Patients Attending The Diabetes Clinic in Kenyatta National HospitalDocument7 pagesAssessment of The Perceived Quality of Life of Non Insulin Dependent Diabetic Patients Attending The Diabetes Clinic in Kenyatta National HospitalIOSR Journal of PharmacyNo ratings yet
- Gluten Free Diet Study On Celiac DiseaseDocument9 pagesGluten Free Diet Study On Celiac DiseaseJahson WillnotloseNo ratings yet
- Problem Solving and Diabetes Self-Management: Investigation in A Large, Multiracial SampleDocument5 pagesProblem Solving and Diabetes Self-Management: Investigation in A Large, Multiracial SampleAndreea MadalinaNo ratings yet
- Out 44Document12 pagesOut 44misscindy123rNo ratings yet
- Mazujnms v2n2p29 enDocument7 pagesMazujnms v2n2p29 enDoc RuthNo ratings yet
- Caranza Diagnosis EnglishDocument3 pagesCaranza Diagnosis EnglishZuwandi Abd KadirNo ratings yet
- Health-Related Quality of Life, Self-Esteem, and Functional Status of Patients With Leg UlcersDocument8 pagesHealth-Related Quality of Life, Self-Esteem, and Functional Status of Patients With Leg UlcersHeba VerebceanNo ratings yet
- International Journal of Health Sciences and Research: Stress and Diabetes MellitusDocument8 pagesInternational Journal of Health Sciences and Research: Stress and Diabetes Mellitusamalia dikaNo ratings yet
- International Journal of Health Sciences and Research: Stress and Diabetes MellitusDocument8 pagesInternational Journal of Health Sciences and Research: Stress and Diabetes MellitusmariahelenaneiNo ratings yet
- Overweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisDocument12 pagesOverweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisLev FyodorNo ratings yet
- Perceived Barriers and Effective Strategies To Diabetic Self-ManagementDocument18 pagesPerceived Barriers and Effective Strategies To Diabetic Self-ManagementArceeJacobaHermosaNo ratings yet
- Esteves 2012Document15 pagesEsteves 2012Nawaf RuwailiNo ratings yet
- Implications of Edentulism On Quality of Life Among ElderlyDocument10 pagesImplications of Edentulism On Quality of Life Among ElderlybkprosthoNo ratings yet
- Oral Lichen PlanusDocument6 pagesOral Lichen PlanusPorcupine TreeNo ratings yet
- Efficacy of Psychological Intervention For Patients With Psoriasis Vulgaris: A Prospective StudyDocument8 pagesEfficacy of Psychological Intervention For Patients With Psoriasis Vulgaris: A Prospective StudyTeuku FadhliNo ratings yet
- Cubos de Corsi IdososDocument5 pagesCubos de Corsi Idososkarlasneris8No ratings yet
- Review Article: Diabetes: Oral Health Related Quality of Life and Oral AlterationsDocument15 pagesReview Article: Diabetes: Oral Health Related Quality of Life and Oral AlterationseveliiiinNo ratings yet
- Cervino Karbo 1Document2 pagesCervino Karbo 1Malya LarasatiNo ratings yet
- JCSM 14 706Document24 pagesJCSM 14 706materi kuliahNo ratings yet
- 2014 Article 47Document8 pages2014 Article 47emmanuelgarciafiscalNo ratings yet
- Μάθημα 7 Παράδειγμα ΜεταανάλυσηςDocument93 pagesΜάθημα 7 Παράδειγμα ΜεταανάλυσηςΠόπη ΜποζίκηNo ratings yet
- The Norwegian Version of The Quality of Life Scale (QOLS-N)Document8 pagesThe Norwegian Version of The Quality of Life Scale (QOLS-N)Andreea OniceanuNo ratings yet
- Art:10.1186/s12903 015 0052 4Document8 pagesArt:10.1186/s12903 015 0052 4Laura Mejia VergaraNo ratings yet
- Estimation of Salivary GlucoseDocument10 pagesEstimation of Salivary GlucoseSuganya MurugaiahNo ratings yet
- Nut in Clin Prac - 2024 - Graciano - Global Leadership Initiative On Malnutrition Criteria in Older Adults Who AreDocument8 pagesNut in Clin Prac - 2024 - Graciano - Global Leadership Initiative On Malnutrition Criteria in Older Adults Who AreIván OsunaNo ratings yet
- Findings From Britain: The Effects Illness Quality of Households in GreatDocument7 pagesFindings From Britain: The Effects Illness Quality of Households in GreatGunung MahameruNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchIlham T Gustama PutraNo ratings yet
- 1 s2.0 S0261561417301486 MainDocument7 pages1 s2.0 S0261561417301486 MaincaylynncreatesNo ratings yet
- 1 s2.0 S0261561423002844 MainDocument8 pages1 s2.0 S0261561423002844 MainRoland GarrozNo ratings yet
- Depression Anxiety and Stress in Oral Lichen Planus A 3gx96ie7qaDocument18 pagesDepression Anxiety and Stress in Oral Lichen Planus A 3gx96ie7qatafazzal.eduNo ratings yet
- A Obesidade Influencia Na Composição Da Microbiota SubgengivalDocument10 pagesA Obesidade Influencia Na Composição Da Microbiota SubgengivalGiovanna Lima Costa BarcelosNo ratings yet
- Abu Ruz 2015Document10 pagesAbu Ruz 2015Aini HiolaNo ratings yet
- Quality of LifeDocument18 pagesQuality of LifeAnaghesh MuruliNo ratings yet
- Ulcus Cruris, Quality of LifeDocument6 pagesUlcus Cruris, Quality of LifeHrvoje CvitanovicNo ratings yet
- Bueno 2018Document26 pagesBueno 2018Fernando VonoNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Baires Dev PreentrevistaDocument3 pagesBaires Dev PreentrevistaCarlos Gonzalo Maravi ArensNo ratings yet
- P1 - CHAPTER 10 - KNOWLEDGE CHECK - Relevant Costs and Decision Making - IMASDocument19 pagesP1 - CHAPTER 10 - KNOWLEDGE CHECK - Relevant Costs and Decision Making - IMASYeon Baek100% (1)
- Asterisk DocumentationDocument34 pagesAsterisk DocumentationSafaa Shaaban50% (2)
- Bradley Stewart ResumeDocument1 pageBradley Stewart ResumeBrad StewartNo ratings yet
- Tangent Planes and Linear ApproximationsDocument7 pagesTangent Planes and Linear ApproximationsMohd Iqbal MuttaqinNo ratings yet
- Saga of Indias Cold Chain DevelopmentDocument47 pagesSaga of Indias Cold Chain DevelopmentseadogNo ratings yet
- Input Modelling: Discrete-Event System SimulationDocument41 pagesInput Modelling: Discrete-Event System SimulationManhNo ratings yet
- Mil STD 1587e PDFDocument43 pagesMil STD 1587e PDFRaj Rajesh100% (1)
- The Color of Quality - Color Control and Measurement in Pharmaceutical IndustryDocument3 pagesThe Color of Quality - Color Control and Measurement in Pharmaceutical IndustryKonica Minolta Sensing Singapore Pte LtdNo ratings yet
- K 0 DDocument24 pagesK 0 DDevna MaheshwariNo ratings yet
- Catalytic Distillation VersionDocument4 pagesCatalytic Distillation Versionlux0008No ratings yet
- D3E8008FB63-Body On Board DiagnosticDocument172 pagesD3E8008FB63-Body On Board DiagnosticAymen HammiNo ratings yet
- CVP AnalysisDocument39 pagesCVP AnalysisIvy Marie DicoNo ratings yet
- A Ip Steering Knuckle 2020Document10 pagesA Ip Steering Knuckle 2020Sunil Kumar BadigerNo ratings yet
- InvoiceDocument2 pagesInvoiceWillian CordovaNo ratings yet
- Applied Pharmacology For The Dental Hygienist 8th Edition Haveles Test BankDocument35 pagesApplied Pharmacology For The Dental Hygienist 8th Edition Haveles Test Bankatop.remiped25zad100% (29)
- KH X-Band Mk4 Block DiagramDocument1 pageKH X-Band Mk4 Block DiagramGlobal Ship SparesNo ratings yet
- School BusDocument156 pagesSchool Bussowmeya veeraraghavanNo ratings yet
- Electrical SystemDocument283 pagesElectrical Systemzed shop73100% (1)
- Ptba PKBL 2014Document90 pagesPtba PKBL 2014AndrianNo ratings yet
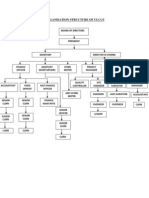
- Organisation Structure of Ulccs: Director in ChargeDocument1 pageOrganisation Structure of Ulccs: Director in ChargeMohamed RiyasNo ratings yet
- Social Media and ElectionsDocument89 pagesSocial Media and ElectionsShara LynNo ratings yet
- Unit 5 International Monetary SystemDocument19 pagesUnit 5 International Monetary SystemerikericashNo ratings yet
- En Ian8k b1000 Msan r330 r340 Icm3ge User v1.4 PDFDocument227 pagesEn Ian8k b1000 Msan r330 r340 Icm3ge User v1.4 PDFمنصورالمغربيNo ratings yet
- P1125P1/P1250E1: Output RatingsDocument6 pagesP1125P1/P1250E1: Output Ratingsmohsen_cumminsNo ratings yet
- Quality Test Bank 2Document16 pagesQuality Test Bank 2Behbehlynn100% (4)
- 2nd Cedric Burl AmpDocument2 pages2nd Cedric Burl AmpCheryl LynnNo ratings yet
- جميع اختبارات الموارد البشريةDocument12 pagesجميع اختبارات الموارد البشريةartistsarah.96No ratings yet
- For Students - AASTU - EMEng-7253 Grade Report (2023)Document1 pageFor Students - AASTU - EMEng-7253 Grade Report (2023)begosew zelalemNo ratings yet