Download as pdf or txt
You might also like
- Schedule E PDFDocument115 pagesSchedule E PDFShisArquamNo ratings yet
- York ComplaintDocument55 pagesYork ComplaintAnonymous Rk1wia100% (2)
- Topic: Recent Advances - Cardiac CT: Journal ClubDocument130 pagesTopic: Recent Advances - Cardiac CT: Journal Clubjai256No ratings yet
- Comparative Study of Laparoscopic Congenital Inguinal Hernia Repair VS Open Congenital Inguinal Hernia Repair PDFDocument3 pagesComparative Study of Laparoscopic Congenital Inguinal Hernia Repair VS Open Congenital Inguinal Hernia Repair PDFrhmathidayatNo ratings yet
- TAPP HernioplastyDocument5 pagesTAPP HernioplastyMaryam Alam KhanNo ratings yet
- El Beheiry2019Document4 pagesEl Beheiry2019achmadaNo ratings yet
- Contoversia de Hernia InguinalDocument13 pagesContoversia de Hernia InguinalOSCAR AUGUSTO QUESADA VEGANo ratings yet
- 1 s2.0 S0022346819307535 MainDocument5 pages1 s2.0 S0022346819307535 MainMeta ParamitaNo ratings yet
- Laparoscopy AppendectomyDocument3 pagesLaparoscopy AppendectomyRoxiutaLNo ratings yet
- Laparoscopic Appendectomy PostoperativeDocument6 pagesLaparoscopic Appendectomy PostoperativeDamal An NasherNo ratings yet
- Laparoscopic Appendectomy For Complicated Appendicitis - An Evaluation of Postoperative Factors.Document5 pagesLaparoscopic Appendectomy For Complicated Appendicitis - An Evaluation of Postoperative Factors.Juan Carlos SantamariaNo ratings yet
- Utd 04524 Clinical - Article KunduzDocument5 pagesUtd 04524 Clinical - Article Kunduzzenatihanen123No ratings yet
- Fifteen Years Experience in Laparoscopic Inguinal Hernia Repair in Pediatric Patients. Results and Considerations On A Debated ProcedureDocument5 pagesFifteen Years Experience in Laparoscopic Inguinal Hernia Repair in Pediatric Patients. Results and Considerations On A Debated ProcedureRagabi RezaNo ratings yet
- Morini 2021Document14 pagesMorini 2021machalliNo ratings yet
- Reoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDocument8 pagesReoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDiego Andres VasquezNo ratings yet
- Inguinal HerniaDocument9 pagesInguinal HerniaAmanda RapaNo ratings yet
- Laparoscopic Appendectomy PDFDocument4 pagesLaparoscopic Appendectomy PDFdydydyNo ratings yet
- Laparoscopic Appendicectomy in All Trimesters of PregnancyDocument7 pagesLaparoscopic Appendicectomy in All Trimesters of PregnancyJason CalvinNo ratings yet
- Complicated AppendicitisDocument4 pagesComplicated AppendicitisMedardo ApoloNo ratings yet
- Open Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialDocument7 pagesOpen Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialAthenaeum Scientific PublishersNo ratings yet
- 1 s2.0 S1015958422008909 MainDocument4 pages1 s2.0 S1015958422008909 MainYohan WijayabahuNo ratings yet
- Hernia InguinalisDocument7 pagesHernia InguinalisabduNo ratings yet
- Bun V34N3p223Document6 pagesBun V34N3p223pingusNo ratings yet
- Nah Incarcerated HerniaDocument4 pagesNah Incarcerated Herniafelix_the_meowNo ratings yet
- Umbilical Hernia: When and How: Raquel A. Maia, Hrishikesh P. Salgaonkar, Davide Lomanto, Lynette LooDocument8 pagesUmbilical Hernia: When and How: Raquel A. Maia, Hrishikesh P. Salgaonkar, Davide Lomanto, Lynette LooZauzaa NabilaNo ratings yet
- Yeh 2019Document5 pagesYeh 2019sigitdwimulyoNo ratings yet
- Laparoscopic Hernia Repair in Neonates, Infants and ChildrenDocument9 pagesLaparoscopic Hernia Repair in Neonates, Infants and ChildrenErick OematanNo ratings yet
- Hernia 2018Document5 pagesHernia 2018Razor GGNo ratings yet
- CDH ArticolDocument12 pagesCDH ArticolamasherbNo ratings yet
- Resuscitation PlusDocument6 pagesResuscitation PlusshifukaNo ratings yet
- Emergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalDocument5 pagesEmergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalleonardoNo ratings yet
- Wright 2011Document3 pagesWright 2011diana.miron.mNo ratings yet
- Journal AppDocument3 pagesJournal AppliqqamuqitaNo ratings yet
- Could Laparoscopic Colon and Rectal Surgery Become The Standard of Care? A Review and Experience With 750 ProceduresDocument9 pagesCould Laparoscopic Colon and Rectal Surgery Become The Standard of Care? A Review and Experience With 750 ProcedurespingusNo ratings yet
- Open Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective StudyDocument3 pagesOpen Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective Study'Adil MuhammadNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument9 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- 1 s2.0 S0022346820305170 MainDocument5 pages1 s2.0 S0022346820305170 MainMeta ParamitaNo ratings yet
- Alesina Et Al., 2021Document9 pagesAlesina Et Al., 2021NyomantrianaNo ratings yet
- Umesh Singh. TLTK-47Document5 pagesUmesh Singh. TLTK-47HẢI HOÀNG THANHNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectMishel Rodriguez GuzmanNo ratings yet
- 0102 6720 Abcd 32 01 E1426Document5 pages0102 6720 Abcd 32 01 E1426Amaury de la CruzNo ratings yet
- Conventional Versus Laparoscopic Surgery For Acute AppendicitisDocument4 pagesConventional Versus Laparoscopic Surgery For Acute AppendicitisAna Luiza MatosNo ratings yet
- Use Only: Intracorporeal Hybrid Single Port Conventional Laparoscopic Appendectomy in ChildrenDocument4 pagesUse Only: Intracorporeal Hybrid Single Port Conventional Laparoscopic Appendectomy in ChildrenYelisa PatandiananNo ratings yet
- International Journal of Surgery: Sri Vengadesh Gopal, Achuthan WarrierDocument4 pagesInternational Journal of Surgery: Sri Vengadesh Gopal, Achuthan WarrierRon Java FantillanNo ratings yet
- Recurrent Groin HerniaDocument6 pagesRecurrent Groin HerniaJohn-adewaleSmithNo ratings yet
- Intravenous Fluid Therapy in The Adult Surgic 2016 International Journal ofDocument1 pageIntravenous Fluid Therapy in The Adult Surgic 2016 International Journal ofoomculunNo ratings yet
- @medicinejournal European Journal of Pediatric Surgery January 2020Document126 pages@medicinejournal European Journal of Pediatric Surgery January 2020Ricardo Uzcategui ArreguiNo ratings yet
- 3 PBDocument6 pages3 PBAulia Rizqi MulyaniNo ratings yet
- Unukovych 2016Document7 pagesUnukovych 2016jdavies231No ratings yet
- Vacuum-Assisted Closure (VAC) Prevents Wound Dehiscence Following Posterior Sagittal Anorectoplasty 2020Document5 pagesVacuum-Assisted Closure (VAC) Prevents Wound Dehiscence Following Posterior Sagittal Anorectoplasty 2020Gunduz AgaNo ratings yet
- 268 2011 Article 1088 PDFDocument6 pages268 2011 Article 1088 PDFIoel Tovar TrovaNo ratings yet
- A Prospective Treatment Protocol For Outpatient Laparoscopic Appendectomy For Acute AppendicitisDocument5 pagesA Prospective Treatment Protocol For Outpatient Laparoscopic Appendectomy For Acute AppendicitisBenjamin PaulinNo ratings yet
- 10 1016@j Jpedsurg 2019 01 040Document14 pages10 1016@j Jpedsurg 2019 01 040AndikaNo ratings yet
- 43 Iajps43052018 PDFDocument6 pages43 Iajps43052018 PDFiajpsNo ratings yet
- Isj-5899 oDocument5 pagesIsj-5899 oAbhiram MundleNo ratings yet
- 1 s2.0 S0002961013004558 Main PDFDocument11 pages1 s2.0 S0002961013004558 Main PDFCarlos AlbertoNo ratings yet
- Outcomes of 207 Totally Extraperitoneal Hernia Repairs Using Self Fixation MeshDocument8 pagesOutcomes of 207 Totally Extraperitoneal Hernia Repairs Using Self Fixation Mesha kNo ratings yet
- Nonoperating Room Anesthesia Anesthesia in The Gastrointestinal SuiteDocument16 pagesNonoperating Room Anesthesia Anesthesia in The Gastrointestinal SuiteGustavo ParedesNo ratings yet
- Endoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our ExperienceDocument6 pagesEndoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our Experiencefarah maulida martaNo ratings yet
- Farach 2014Document5 pagesFarach 2014mia widiastutiNo ratings yet
- Laparoscopic Versus Open Inguinal Hernia Repair in Pediatric Patients: A Systematic ReviewDocument9 pagesLaparoscopic Versus Open Inguinal Hernia Repair in Pediatric Patients: A Systematic ReviewAbdul RahmanNo ratings yet
- Management of The Acute Appendix Mass: A Survey of Surgical PracticeDocument3 pagesManagement of The Acute Appendix Mass: A Survey of Surgical PracticeSamuel H SihotangNo ratings yet
- Surgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesFrom EverandSurgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesMelissa Phillips LaPinskaNo ratings yet
- Age-Dependent Outcomes in Asymptomatic Umbilical Hernia RepairDocument6 pagesAge-Dependent Outcomes in Asymptomatic Umbilical Hernia RepairAnisaa GayatriNo ratings yet
- Direct Hyperbilirubinemia in Newborns With GastroschisisDocument9 pagesDirect Hyperbilirubinemia in Newborns With GastroschisisAnisaa GayatriNo ratings yet
- 10 1089@sur 2019 175Document7 pages10 1089@sur 2019 175Anisaa GayatriNo ratings yet
- Laparoscopic Needle - Assisted Repair For Pediatric Inguinal HerniaDocument3 pagesLaparoscopic Needle - Assisted Repair For Pediatric Inguinal HerniaAnisaa GayatriNo ratings yet
- 9.perubahan Fisiologik BBLDocument37 pages9.perubahan Fisiologik BBLAnisaa GayatriNo ratings yet
- Jaha 118 009893Document17 pagesJaha 118 009893Anisaa GayatriNo ratings yet
- Poster 10 PALS 01 01 ENG V20100927 PDFDocument1 pagePoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNo ratings yet
- CHM Case Study ChymotrypsinDocument8 pagesCHM Case Study Chymotrypsinfanney- chanNo ratings yet
- L A Level Biology MS Jan 06Document180 pagesL A Level Biology MS Jan 06zetsubou-chanNo ratings yet
- Jurnal SkizofreniaDocument9 pagesJurnal SkizofreniaAbdul HamidNo ratings yet
- 1.1. Krisis Hipertensi - Dr. Saugi AbduhDocument29 pages1.1. Krisis Hipertensi - Dr. Saugi AbduhdmaulidaNo ratings yet
- Volume 42, Issue 34 - August 26, 2011Document56 pagesVolume 42, Issue 34 - August 26, 2011BladeNo ratings yet
- Caries Case StudyDocument19 pagesCaries Case Studyapi-279025476No ratings yet
- GASTRITISDocument11 pagesGASTRITISHemant SharmaNo ratings yet
- College of Agriculture, Rajendranagar, Hyderabad-500030: Professor Jayashankar Telangana State Agricultural UniversityDocument34 pagesCollege of Agriculture, Rajendranagar, Hyderabad-500030: Professor Jayashankar Telangana State Agricultural UniversityNur KusmiyatiNo ratings yet
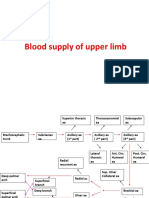
- Blood Supply of Upper LimbDocument36 pagesBlood Supply of Upper Limbteklay100% (2)
- Kidney Introduction PDF 508Document10 pagesKidney Introduction PDF 508Shailesh DixitNo ratings yet
- NCP DiarrheaDocument2 pagesNCP DiarrheaPrincess Xzmae RamirezNo ratings yet
- SITXFSA001 Student Assessment TasksDocument24 pagesSITXFSA001 Student Assessment TasksMukta AktherNo ratings yet
- Dialog AssignmentDocument4 pagesDialog AssignmentKitket Photografi & Cinematografi100% (1)
- Mina Drug StudyDocument7 pagesMina Drug StudyChi Chaw Giselle HilarioNo ratings yet
- Imaging of Solitary and Multiple Pulmonary NodulesDocument75 pagesImaging of Solitary and Multiple Pulmonary NodulesAnshulVarshneyNo ratings yet
- Streeoverlord PIDocument1 pageStreeoverlord PIdoobiedoodooNo ratings yet
- Hormone Replacement Therapy The Right Choice For Your PatientDocument9 pagesHormone Replacement Therapy The Right Choice For Your Patientdanny17phNo ratings yet
- PNLE Community Health Nursing Exam 4Document9 pagesPNLE Community Health Nursing Exam 4Denisse PalayNo ratings yet
- Posterior Reversible Encephalopathy Syndrome in A Postpartum Normotensive Post Cesarean Patient - A Case ReportDocument4 pagesPosterior Reversible Encephalopathy Syndrome in A Postpartum Normotensive Post Cesarean Patient - A Case ReportIJAR JOURNALNo ratings yet
- 7th Symbiosis B Krishna Memorial National Moot Court Competition 2015 MDocument29 pages7th Symbiosis B Krishna Memorial National Moot Court Competition 2015 MChirag AhluwaliaNo ratings yet
- Food Safety ManualDocument39 pagesFood Safety ManualAlvic Hisoler Sinadjan RodaNo ratings yet
- BloodlettingDocument5 pagesBloodlettingMaria Lana Grace DiazNo ratings yet
- Blood DonationDocument15 pagesBlood DonationperllyNo ratings yet
- Nutrition and Oral Health - (Review) : L. Leelavathi, Santa Thoudam and M. AnithaDocument5 pagesNutrition and Oral Health - (Review) : L. Leelavathi, Santa Thoudam and M. AnithaKhalisahatma BklNo ratings yet
- Biology Matters 3rd EditionDocument272 pagesBiology Matters 3rd Editionotakukat763No ratings yet
- 28-Abhishek TiwariDocument3 pages28-Abhishek TiwariAbhishek TiwariNo ratings yet