Download as pdf or txt
You might also like
- Pediatric Drug Dosage - All in One PDFDocument15 pagesPediatric Drug Dosage - All in One PDFHuang Hasjim33% (9)
- Paediatric Dosage of Some DrugsDocument46 pagesPaediatric Dosage of Some DrugsS S LNo ratings yet
- YOUNG MIN LEE CASE STUDY Update 2Document7 pagesYOUNG MIN LEE CASE STUDY Update 2E.R.ONo ratings yet
- Paediatric Dosage of Some Drugs-1Document45 pagesPaediatric Dosage of Some Drugs-1JaneNo ratings yet
- Concept Map Finished 2Document6 pagesConcept Map Finished 2api-352785497100% (1)
- Antimicrobial Drugs FormularyDocument95 pagesAntimicrobial Drugs FormularymahamoudNo ratings yet
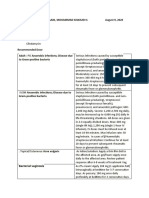
- D-6-12 Sanaani, Mohammad Khaisar H. August 9, 2020: Bacterial VaginosisDocument4 pagesD-6-12 Sanaani, Mohammad Khaisar H. August 9, 2020: Bacterial VaginosisKenMNo ratings yet
- Measles PHIDSPILDocument5 pagesMeasles PHIDSPILriczen mae vilaNo ratings yet
- Theraputic Agent in NeonateDocument7 pagesTheraputic Agent in Neonateد. محمد فريد الغنامNo ratings yet
- AntibioticsDocument13 pagesAntibioticsJOrgeNo ratings yet
- Antimicrobial PDFDocument7 pagesAntimicrobial PDFvhonNo ratings yet
- Pediatric Antibiotic DosingDocument7 pagesPediatric Antibiotic DosingAnonymous mm1yTelKNo ratings yet
- Homeo Drug CompenDocument6 pagesHomeo Drug CompenSittie Nadia MangondatoNo ratings yet
- Urinary Tract InfectionsDocument15 pagesUrinary Tract InfectionsAnonymous elSqPhzKNo ratings yet
- Antibiotik Beta Laktam: Apt. Ika Mustikaningtias, M.SCDocument26 pagesAntibiotik Beta Laktam: Apt. Ika Mustikaningtias, M.SCdita novia maharaniNo ratings yet
- Oxaciline PDFDocument7 pagesOxaciline PDFamatoryfictionliteraNo ratings yet
- Modul PneumoniaDocument16 pagesModul Pneumoniaandamar0290No ratings yet
- Degracia, John Noeh D. Drug StudyDocument15 pagesDegracia, John Noeh D. Drug StudyLenie DegraciaNo ratings yet
- Pneumonia: Fever Cough Breathlessnes S DR J Pap/ich/ GMC Kottayam/19723Document4 pagesPneumonia: Fever Cough Breathlessnes S DR J Pap/ich/ GMC Kottayam/19723Firdouse ShajiNo ratings yet
- Terapi AnakDocument10 pagesTerapi AnakIka KrastanayaNo ratings yet
- Route/Dosage: Concentration: Not To Exceed 10 Mg/ml. Do NotDocument2 pagesRoute/Dosage: Concentration: Not To Exceed 10 Mg/ml. Do NotMaria MargaritaNo ratings yet
- Common Goat Medications and "Easy To Understand" Dosages: WormersDocument2 pagesCommon Goat Medications and "Easy To Understand" Dosages: WormersCrosley NasmNo ratings yet
- Antimicrobial Regimens For The Treatment of Streptococcus Anginosus GDocument2 pagesAntimicrobial Regimens For The Treatment of Streptococcus Anginosus GKhor Chin PooNo ratings yet
- 6.1 Quick Ref Guide MNGT Antivenom Reactions SGB2021 Ver. 2Document3 pages6.1 Quick Ref Guide MNGT Antivenom Reactions SGB2021 Ver. 2anju sulishaNo ratings yet
- Kumpulan Daftar ObatDocument6 pagesKumpulan Daftar ObatZega AgustianNo ratings yet
- SPC IntratectDocument9 pagesSPC IntratectprincezettaNo ratings yet
- Antibiotic Guidelines For PediatricsDocument33 pagesAntibiotic Guidelines For PediatricsVarshini Tamil SelvanNo ratings yet
- NICU ABX ChartDocument11 pagesNICU ABX ChartdrchiNo ratings yet
- Antibiotic Treatment of Infection Due To Vibrio Vulnificus - UpToDateDocument2 pagesAntibiotic Treatment of Infection Due To Vibrio Vulnificus - UpToDateKevo VillagranNo ratings yet
- FlucloxacillinDocument4 pagesFlucloxacillinSergeNo ratings yet
- Moderately HighLY Protein Bound DrugsDocument10 pagesModerately HighLY Protein Bound DrugsArah MomoNo ratings yet
- Nidua's Drug ChartDocument5 pagesNidua's Drug ChartSarah Michelle NiduaNo ratings yet
- Finasteride: Analgesics (Non-Opioid) & AntipyreticsDocument5 pagesFinasteride: Analgesics (Non-Opioid) & AntipyreticsSarah Michelle NiduaNo ratings yet
- Antibiotic RegimetotreatpneumoniaDocument1 pageAntibiotic RegimetotreatpneumoniaNousheen ThakurNo ratings yet
- Guide Paed Bone JNTDocument11 pagesGuide Paed Bone JNTDorica GiurcaNo ratings yet
- Drug of Treatment For Meningitis: Penicillin Cefotaxime ResistantDocument5 pagesDrug of Treatment For Meningitis: Penicillin Cefotaxime ResistantNama BestNo ratings yet
- Drug StudyDocument10 pagesDrug StudybaniniycsebNo ratings yet
- Name of The Medicinal ProductDocument7 pagesName of The Medicinal ProductSyifa Dina Az-ZahraNo ratings yet
- Drugs Acting On Immune SystemDocument6 pagesDrugs Acting On Immune SystemSORENI SORENINo ratings yet
- Rle Neonate DrugsDocument13 pagesRle Neonate DrugsLhara Vhaneza CuetoNo ratings yet
- Analgesik/Pire Tik Dosis Sediaan Obat DOA OOA Drug Interaction Paracetamol IVDocument9 pagesAnalgesik/Pire Tik Dosis Sediaan Obat DOA OOA Drug Interaction Paracetamol IVNicole NgoNo ratings yet
- S Aureus TableDocument1 pageS Aureus TableCherylNo ratings yet
- EPIGENTDocument3 pagesEPIGENTmahgad100% (1)
- Ampicillin PDFDocument3 pagesAmpicillin PDFandriNo ratings yet
- Ac IphinDocument5 pagesAc IphinAdittya DuttaNo ratings yet
- Classification of PenicillinDocument3 pagesClassification of PenicillinNurfarzana NadhirahNo ratings yet
- MPC Antidote ChartDocument1 pageMPC Antidote Chartogodothomas51No ratings yet
- Levetiracetam PDFDocument3 pagesLevetiracetam PDFShaira TanNo ratings yet
- Tamiflu Epar Product Information - enDocument118 pagesTamiflu Epar Product Information - enUmar AliNo ratings yet
- 4 SeizuresDocument11 pages4 SeizuresApple MaeNo ratings yet
- Generic NameDocument4 pagesGeneric NamePharmacist Amy CharlieNo ratings yet
- Antibiotic ConversionDocument9 pagesAntibiotic ConversionfabianNo ratings yet
- Medications: Medication Name Generic/Trade Classification Pregnancy CategoryDocument8 pagesMedications: Medication Name Generic/Trade Classification Pregnancy CategoryapalestiNo ratings yet
- Levetiracetam Brand Indication Dosage Form Cost/Packing: Adult and Adolescent 16 Years 500mg BIDDocument4 pagesLevetiracetam Brand Indication Dosage Form Cost/Packing: Adult and Adolescent 16 Years 500mg BIDMark PradsNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Meningitis ReviewDocument2 pagesMeningitis ReviewBolbol hayranNo ratings yet
- Obat AnestesiDocument9 pagesObat AnestesiNatanael SusantoNo ratings yet
- 2015 Pain Management For PediatricDocument2 pages2015 Pain Management For Pediatricdiany astutiNo ratings yet
- Paediatric Drug UsageDocument13 pagesPaediatric Drug UsageasmaNo ratings yet
- AntibiocardDocument25 pagesAntibiocardchildicuNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Linezolid PDFDocument1 pageLinezolid PDFmariam ibrahimNo ratings yet
- Systemic Toxicity of Local AnaestheticsDocument1 pageSystemic Toxicity of Local Anaestheticsmariam ibrahimNo ratings yet
- AminoglycosidesDocument1 pageAminoglycosidesmariam ibrahimNo ratings yet
- Fluoroquinolones PDFDocument1 pageFluoroquinolones PDFmariam ibrahimNo ratings yet
- Linezolid PDFDocument1 pageLinezolid PDFmariam ibrahimNo ratings yet
- Daftar Pasien Neurologi Rabu, 17 FEBRUARI 2021: Lontara 3 Saraf Kamar 1Document4 pagesDaftar Pasien Neurologi Rabu, 17 FEBRUARI 2021: Lontara 3 Saraf Kamar 1Louis MailuhuNo ratings yet
- Ramsay Hunt Syndrome: Infectious DiseasesDocument3 pagesRamsay Hunt Syndrome: Infectious DiseasesAldy BimaNo ratings yet
- US Biological Symbols 05AU17Document11 pagesUS Biological Symbols 05AU17Reid KirbyNo ratings yet
- Types of Disability and Disorders-1&2Document44 pagesTypes of Disability and Disorders-1&2Digambar SahooNo ratings yet
- Polycythemia: (Primary & Secondary)Document16 pagesPolycythemia: (Primary & Secondary)Vanessa Camille DomingoNo ratings yet
- Endomaterial Cancer-1Document28 pagesEndomaterial Cancer-1A.H.ANo ratings yet
- Psikiatri: Nonfarmako: CBT Farmako: SsriDocument4 pagesPsikiatri: Nonfarmako: CBT Farmako: SsriRekapriantiNo ratings yet
- Cholera in NepalDocument57 pagesCholera in NepalBinayaNo ratings yet
- Fat-And Water-Soluble VitaminsDocument9 pagesFat-And Water-Soluble VitaminsJessa Mae OhaoNo ratings yet
- Inflammatory EssayDocument1 pageInflammatory EssayJenny BaiNo ratings yet
- Lesson PlanDocument9 pagesLesson PlanAisa B. TaerNo ratings yet
- CalamineDocument4 pagesCalamineFaye FelicesNo ratings yet
- MIO SheetDocument1 pageMIO SheetjnetNo ratings yet
- Urticaria, Angioedema, and Anaphylaxis AGO 2020Document12 pagesUrticaria, Angioedema, and Anaphylaxis AGO 2020Elizabeth HendersonNo ratings yet
- Anxiety Anna Schwartz, M.D. and Adriana Feder, M.D.: EtiologyDocument4 pagesAnxiety Anna Schwartz, M.D. and Adriana Feder, M.D.: EtiologyIrish_Tolentin_6195No ratings yet
- Ophthalmology: NEET PG 2020 QuestionsDocument17 pagesOphthalmology: NEET PG 2020 QuestionsAnmol KudalNo ratings yet
- ANT Handbook 2023Document84 pagesANT Handbook 2023latibaleni02No ratings yet
- Gall StoneDocument38 pagesGall Stoneumay83% (6)
- Gastrointestinal Stromal TumoursDocument22 pagesGastrointestinal Stromal TumoursThomas KlebNo ratings yet
- Introduction To Oncology NursingDocument35 pagesIntroduction To Oncology NursingDesh Deepak100% (1)
- Lapkas Marasmus JadiDocument48 pagesLapkas Marasmus JadiRivhan FauzanNo ratings yet
- Disease Diagnosis System: Software Requirement Specification (SRS)Document11 pagesDisease Diagnosis System: Software Requirement Specification (SRS)Shubham BhadauriaNo ratings yet
- Moh - Fahri (Dermatitis Venenata)Document5 pagesMoh - Fahri (Dermatitis Venenata)fahriitoNo ratings yet
- AbViser IAP Monitoring Device BrochureDocument2 pagesAbViser IAP Monitoring Device BrochuremasmblinkNo ratings yet
- F&E ExamDocument3 pagesF&E ExamDino PringNo ratings yet
- Impaired Gas ExchangeDocument5 pagesImpaired Gas ExchangeKM67% (3)
- Granuloma AnnulareDocument6 pagesGranuloma AnnulareGitarefinaNo ratings yet
- Thrombosis and Acute LeukemiaDocument6 pagesThrombosis and Acute Leukemiaannisa edwarNo ratings yet
- Kuliah Pakar Anemia in Pregnancy Dr. Ima IndirayaniDocument74 pagesKuliah Pakar Anemia in Pregnancy Dr. Ima IndirayaniHamba AllahNo ratings yet