Download as pdf or txt
You might also like
- Blood Chemistry and CBC Analysis - Clinical Laboratory Testing From A Functional Perspective - Quick Reference GuideDocument29 pagesBlood Chemistry and CBC Analysis - Clinical Laboratory Testing From A Functional Perspective - Quick Reference Guidejamesilluminare71% (17)
- PST 04104 Pharmaceutical Dosage FormsDocument17 pagesPST 04104 Pharmaceutical Dosage FormsambroceNo ratings yet
- Systemic Response To Injury and Metabolic SupportDocument118 pagesSystemic Response To Injury and Metabolic SupportNicole DeverasNo ratings yet
- Berbagai Macam Insulin Dan Cara KerjanyaDocument51 pagesBerbagai Macam Insulin Dan Cara KerjanyaAnonymous spBVX6t30UNo ratings yet
- Fat Around The Middle - Marilyn GlenvilleDocument46 pagesFat Around The Middle - Marilyn GlenvilleDorinNo ratings yet
- The Stubborn Fat SolutionDocument50 pagesThe Stubborn Fat SolutionMohamed Elkhder100% (2)
- Insulin 08Document99 pagesInsulin 08Archana Govindan100% (1)
- Insulin Secretion - Newer PerspectiveDocument6 pagesInsulin Secretion - Newer PerspectivehhhNo ratings yet
- L20 Signal Transduction and Mechanism of Hormone ActionDocument51 pagesL20 Signal Transduction and Mechanism of Hormone Actionyebadem228No ratings yet
- The Endocrine Pancreas & The Control of Blood Glucose: 1. A-Cells (20%)Document63 pagesThe Endocrine Pancreas & The Control of Blood Glucose: 1. A-Cells (20%)Ledia EssamNo ratings yet
- Anti Diabetik A OralDocument28 pagesAnti Diabetik A OralMelly Indah PurwantiNo ratings yet
- Unacademy 2 PDFDocument26 pagesUnacademy 2 PDFANUPAM ANAND KUMAR PANDEY MBA-INo ratings yet
- 2015 Nme 232 HormonesDocument31 pages2015 Nme 232 Hormonesshirley_ling_15No ratings yet
- Cell Signaling and Receptos TypesDocument42 pagesCell Signaling and Receptos Typesashhkhan420No ratings yet
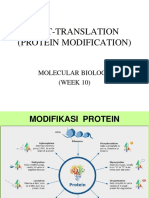
- 10 Protein ModificationDocument36 pages10 Protein ModificationvinaNo ratings yet
- Regulation of LipidsDocument13 pagesRegulation of LipidsNeha SrivastavaNo ratings yet
- Class 2Document29 pagesClass 2Roy Anderson Oropeza ClavoNo ratings yet
- DS-51421 DXC Integrated Systems Menu USDocument2 pagesDS-51421 DXC Integrated Systems Menu USzaid atcNo ratings yet
- Diabetes Mellitus AND Glucose Regulation: MarchDocument92 pagesDiabetes Mellitus AND Glucose Regulation: MarchIvone LorettaNo ratings yet
- Ppi1637a01 CK MB TabletsDocument2 pagesPpi1637a01 CK MB TabletsNehul PatilNo ratings yet
- 4 Adrenergic AgonistsDocument46 pages4 Adrenergic Agonistsmatchees-gone rogueNo ratings yet
- Lect # 3 GluconeogenesisDocument40 pagesLect # 3 GluconeogenesisUbaid ur Rahman100% (1)
- Biosynthesis of LIpidsDocument21 pagesBiosynthesis of LIpidsJoyce Hanniel CastinoNo ratings yet
- Anti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriDocument35 pagesAnti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriPoppyNo ratings yet
- Gen Bio - Reactions That Produce and Consume ATP - 2nd QuarterDocument4 pagesGen Bio - Reactions That Produce and Consume ATP - 2nd QuarterChrislyn Eds Javier AcobNo ratings yet
- Theory Part A-20.7.2016Document57 pagesTheory Part A-20.7.2016ShowmickNo ratings yet
- Farmakodinamik Obat Anti DiabetesDocument24 pagesFarmakodinamik Obat Anti DiabetesAsma Somadayo100% (1)
- Biochem Pearls8900069700399800194Document16 pagesBiochem Pearls8900069700399800194Jhon Carlo TegioNo ratings yet
- Creatine Kinase: Store at 2-8ºCDocument4 pagesCreatine Kinase: Store at 2-8ºCLaboratorios HerliNo ratings yet
- Lecture 3 How Drugs Act Molecular AspectsDocument82 pagesLecture 3 How Drugs Act Molecular AspectsAuthor Nauman ShadNo ratings yet
- Human Bioenerge-Cs and ExerciseDocument128 pagesHuman Bioenerge-Cs and ExerciseDan BernardinoNo ratings yet
- 1b. Bioenergetics. DR NaimDocument41 pages1b. Bioenergetics. DR Naimsaadali919782No ratings yet
- Ord 2.3Document33 pagesOrd 2.3LoNo ratings yet
- HB09 Intro Metabolism 21.12.2020Document54 pagesHB09 Intro Metabolism 21.12.2020Thisha MohanNo ratings yet
- IBO 2016 - Theoretical Exam ADocument57 pagesIBO 2016 - Theoretical Exam AAlexNo ratings yet
- Carbo ChemDocument123 pagesCarbo ChemHan MichelNo ratings yet
- 10 GluconeogenesisDocument18 pages10 GluconeogenesiskulturewearzmNo ratings yet
- Metabolic PathwaysDocument6 pagesMetabolic Pathwaysgelary sousaNo ratings yet
- Anti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriDocument30 pagesAnti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriDewi Putri Lenggo GeniNo ratings yet
- Nature 14953Document18 pagesNature 14953Rin ChanNo ratings yet
- ZBM0031 01LIP2RBLipolysisKit08 08Document9 pagesZBM0031 01LIP2RBLipolysisKit08 08evanconstantine77No ratings yet
- Water Soluble VitaminsDocument55 pagesWater Soluble VitaminsDr. M. Prasad Naidu100% (1)
- METABOLISMDocument11 pagesMETABOLISMking untalanNo ratings yet
- BIOLOGICAL OXIDATION & Principle of Energy MetabolismDocument84 pagesBIOLOGICAL OXIDATION & Principle of Energy MetabolismOdi YuventiusNo ratings yet
- Cell Signalling Basics Part 2Document15 pagesCell Signalling Basics Part 26ypywxdqmkNo ratings yet
- Kreb's CycleDocument8 pagesKreb's CycleHaneen HafizNo ratings yet
- Carbohydrate Metabolism 1Document22 pagesCarbohydrate Metabolism 1Affie SaikolNo ratings yet
- PDH Complex and TCA CycleDocument20 pagesPDH Complex and TCA CycleDarrion LouisNo ratings yet
- Phys 10Document22 pagesPhys 10sakwork30No ratings yet
- CH 7 Cellular Respiration CompleteDocument31 pagesCH 7 Cellular Respiration CompleteWilly WonkaNo ratings yet
- Biochemistry - 230204 - 191022Document41 pagesBiochemistry - 230204 - 191022DRJS 74No ratings yet
- 07 PDH and Tca CycleDocument23 pages07 PDH and Tca CyclePrincess Noreen SavellanoNo ratings yet
- Pharmacodynamics of Antidiabetic DrugsDocument25 pagesPharmacodynamics of Antidiabetic DrugsAbdurahman RidhoduaNo ratings yet
- IT 10 - Farmakologi Obat - Obat Di Bidang Endokrin - TEODocument34 pagesIT 10 - Farmakologi Obat - Obat Di Bidang Endokrin - TEOtattosssNo ratings yet
- 630 FullDocument12 pages630 FullMedranoReyesLuisinNo ratings yet
- Cellular Respiration PDFDocument85 pagesCellular Respiration PDFmailforprinting101No ratings yet
- En ZymologyDocument6 pagesEn ZymologyNathaniel Derige AndesNo ratings yet
- MD ch5Document27 pagesMD ch5malake.a13cj7No ratings yet
- Photosynthesis in Higher PlantsDocument3 pagesPhotosynthesis in Higher Plantsakhil01ajNo ratings yet
- Regulation & Integration of MetabolismDocument41 pagesRegulation & Integration of MetabolismMohamedNo ratings yet
- Introduction BCHN 222 2022Document39 pagesIntroduction BCHN 222 2022Francisca ManyisaNo ratings yet
- Chok Biochem 4th Shift Reviewer EyeDocument2 pagesChok Biochem 4th Shift Reviewer EyenkivcNo ratings yet
- Second LectrueDocument44 pagesSecond Lectrueapi-3700537No ratings yet
- Gluconeogenesis 2021 BCH 1216, BCH 1217 - 220729 - 143221Document39 pagesGluconeogenesis 2021 BCH 1216, BCH 1217 - 220729 - 143221Solome AkolNo ratings yet
- Co- and Post-Translational Modifications of Therapeutic Antibodies and ProteinsFrom EverandCo- and Post-Translational Modifications of Therapeutic Antibodies and ProteinsNo ratings yet
- Evalina Elias Proposal Draft 01Document5 pagesEvalina Elias Proposal Draft 01ambroceNo ratings yet
- Basic Pharmacology - Feb 2021Document11 pagesBasic Pharmacology - Feb 2021ambroceNo ratings yet
- Individual Assignment 02-Pst 05104 Pharmacology & TherapeuticsDocument1 pageIndividual Assignment 02-Pst 05104 Pharmacology & TherapeuticsambroceNo ratings yet
- 01 Pharmacology PST 05-1Document319 pages01 Pharmacology PST 05-1ambroceNo ratings yet
- Good Manufacturing Practice: Personal HygieneDocument9 pagesGood Manufacturing Practice: Personal HygieneambroceNo ratings yet
- PST 04104 Pharmaceutical Dosage Forms-Marking GuideDocument20 pagesPST 04104 Pharmaceutical Dosage Forms-Marking GuideambroceNo ratings yet
- 16.good Practice in ProductionDocument12 pages16.good Practice in ProductionambroceNo ratings yet
- The Pharmacy (Accredited Drug Dispensing Outlets) Standards and Ethics For Dispensations of Medicines Regulations G.N 185 of 2019Document35 pagesThe Pharmacy (Accredited Drug Dispensing Outlets) Standards and Ethics For Dispensations of Medicines Regulations G.N 185 of 2019ambroceNo ratings yet
- Good Manufacturing Practices of Pharmaceutical Industry: Bpharm Four 2020Document11 pagesGood Manufacturing Practices of Pharmaceutical Industry: Bpharm Four 2020ambroceNo ratings yet
- COMPLAINTDocument16 pagesCOMPLAINTambroceNo ratings yet
- Cholinergic ReceptorsDocument121 pagesCholinergic ReceptorsambroceNo ratings yet
- DRUG DISCOVERY-NewDocument60 pagesDRUG DISCOVERY-NewambroceNo ratings yet
- Natural PesticidesDocument36 pagesNatural PesticidesambroceNo ratings yet
- Kilimooooo PDFDocument4 pagesKilimooooo PDFambroceNo ratings yet
- PesticidesDocument36 pagesPesticidesambroce100% (1)
- WHO Good Manufacturing Practices (GMP) For Pharmaceutical Products: Main PrinciplesDocument10 pagesWHO Good Manufacturing Practices (GMP) For Pharmaceutical Products: Main PrinciplesambroceNo ratings yet
- Roles of Forensic PharmacistDocument1 pageRoles of Forensic PharmacistambroceNo ratings yet
- Therapeutics Summary of Last SessionDocument3 pagesTherapeutics Summary of Last SessionambroceNo ratings yet
- Pharmacognosy Group Assignment: Natural Carcinogens and Tumour PromotersDocument9 pagesPharmacognosy Group Assignment: Natural Carcinogens and Tumour PromotersambroceNo ratings yet
- Catholic University of Health and ALLIED Email: Vc@bugando - Ac.tz Call Us: +255 (0) 28 250 0881 SCIENCEDocument2 pagesCatholic University of Health and ALLIED Email: Vc@bugando - Ac.tz Call Us: +255 (0) 28 250 0881 SCIENCEambroceNo ratings yet
- Poisonous Plants: Mushroom and Other HallucinogensDocument17 pagesPoisonous Plants: Mushroom and Other HallucinogensambroceNo ratings yet
- Chapter 34 Insulin & Oral Antidiabetic DrugsDocument24 pagesChapter 34 Insulin & Oral Antidiabetic DrugsIlham RamadhanNo ratings yet
- The Influence of Telmisartan On Metformin PharmacokineticsDocument5 pagesThe Influence of Telmisartan On Metformin PharmacokineticsAdi permadiNo ratings yet
- Diabetes MellitusDocument15 pagesDiabetes Mellitusmendoza.rainnarhieNo ratings yet
- Tyg-Bmi As A Surrogate Marker in Hypertensive Patients - An Observational Study in Tertiary Care HospitalDocument7 pagesTyg-Bmi As A Surrogate Marker in Hypertensive Patients - An Observational Study in Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Fetal Origins of Adult DiseaseDocument9 pagesFetal Origins of Adult DiseaseMuljadi HartonoNo ratings yet
- Effect of Cinnamon On Diabetes Mariana Kalenichenko University of North Florida FOS 4041 April 3rd, 2018Document11 pagesEffect of Cinnamon On Diabetes Mariana Kalenichenko University of North Florida FOS 4041 April 3rd, 2018api-435685106No ratings yet
- Diabetes Mellitus PathologyDocument5 pagesDiabetes Mellitus PathologyNada MuchNo ratings yet
- Diabetes Mellitus in Children (Pedi Clinics of N. America Vol 52, No 6) WW PDFDocument275 pagesDiabetes Mellitus in Children (Pedi Clinics of N. America Vol 52, No 6) WW PDFEliMihaelaNo ratings yet
- 6 Natural Treatments For PCOSDocument3 pages6 Natural Treatments For PCOSJudi Ann MagsacayNo ratings yet
- The Blood Sugar Solution 2012Document306 pagesThe Blood Sugar Solution 2012Waqar Ahmed Awan100% (7)
- Diabetes and ExerciseDocument23 pagesDiabetes and ExerciseApurba MukherjeeNo ratings yet
- Chapter 4 Maternal PhysiologyDocument12 pagesChapter 4 Maternal PhysiologyRem AlfelorNo ratings yet
- Pancreatic Hormones & Antidiabetic DrugsDocument41 pagesPancreatic Hormones & Antidiabetic DrugsSaddamix AL OmariNo ratings yet
- DiabetesDocument515 pagesDiabetesPaola Rivera DiazNo ratings yet
- Secondary Causes of DyslipidemiaDocument3 pagesSecondary Causes of DyslipidemiaAnghelo Aldair Velásquez CarrilloNo ratings yet
- Coconut Research-Coconut Research CenterDocument38 pagesCoconut Research-Coconut Research CenterBlitzoneNo ratings yet
- Ref - Guide For People With DiabetesDocument70 pagesRef - Guide For People With DiabetesJamie SmithNo ratings yet
- BioSignature Review - Are Hormones The Key To Weight LossDocument19 pagesBioSignature Review - Are Hormones The Key To Weight LossVladimir OlefirenkoNo ratings yet
- Taiwanese Journal of Obstetrics & Gynecology: Ching-Ju Shen, Shih-Han Wang, Chien-Hung Lee, Te-Fu ChanDocument4 pagesTaiwanese Journal of Obstetrics & Gynecology: Ching-Ju Shen, Shih-Han Wang, Chien-Hung Lee, Te-Fu ChanIman Ru-ancaNo ratings yet
- Diabetis ThesisDocument23 pagesDiabetis ThesisHannah CaldinoNo ratings yet
- Diabetes MellitusDocument9 pagesDiabetes MellitusErline Suzette GabrielNo ratings yet
- Insulin Resistance & Green TeaDocument6 pagesInsulin Resistance & Green TeaSrinivasan GanapathiNo ratings yet
- Utsav2, Et AlDocument16 pagesUtsav2, Et Alnadin nNo ratings yet
- Osmun Case StudyDocument48 pagesOsmun Case StudyraffineeNo ratings yet
- Ayuno Intermitente y Diabeticos 2Document10 pagesAyuno Intermitente y Diabeticos 2vicenteNo ratings yet