Download as pdf or txt
You might also like
- Paces Exam Cases 2nd Version PDFDocument471 pagesPaces Exam Cases 2nd Version PDFMuntadher Kareem100% (1)
- PASSMEDICINE MRCP MCQs-PALLIATIVE MEDICINE AND END OF LIFE CAREDocument17 pagesPASSMEDICINE MRCP MCQs-PALLIATIVE MEDICINE AND END OF LIFE CAREHashim Ahmad100% (4)
- Neurology Multiple Choice Questions With Explanations: Volume IIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIRating: 5 out of 5 stars5/5 (2)
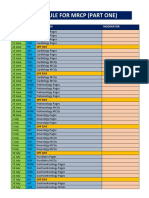
- Schedule For MRCP (Part One) PDFDocument3 pagesSchedule For MRCP (Part One) PDFImran ChaudhryNo ratings yet
- PLAB 2 Stations JAN 2020 (Updated)Document11 pagesPLAB 2 Stations JAN 2020 (Updated)Imran Chaudhry100% (5)
- Diuretic Cases and Self-Test Questions With AnswersDocument19 pagesDiuretic Cases and Self-Test Questions With AnswersRoxana CaravețeanuNo ratings yet
- Passmedicine MRCP Mcqs-Clinical SciencesDocument232 pagesPassmedicine MRCP Mcqs-Clinical SciencesHashim AhmadNo ratings yet
- PRES3 RecallsDocument9 pagesPRES3 RecallsAhmed GendiaNo ratings yet
- 86 MRCP Part 2 Sample QuestionsDocument86 pages86 MRCP Part 2 Sample QuestionsJa Gh50% (2)
- Management of Heart FailureDocument62 pagesManagement of Heart Failureapi-13265958No ratings yet
- MRCP-2 July 2021 Recall QsDocument10 pagesMRCP-2 July 2021 Recall Qszehra khowajaNo ratings yet
- 390 QuestionsDocument26 pages390 QuestionsBenie BudNo ratings yet
- Delirium Pre-Test QuestionsDocument8 pagesDelirium Pre-Test QuestionsyohanesNo ratings yet
- Kingston Hospital Blue Book 2019Document207 pagesKingston Hospital Blue Book 2019Chris Jardine LiNo ratings yet
- PMDC NEB Exam Medical FormatDocument6 pagesPMDC NEB Exam Medical FormatShawn Parker57% (7)
- 1 - Elzohry MasterClass 2010 (MRCP Part2)Document839 pages1 - Elzohry MasterClass 2010 (MRCP Part2)tejbirsingh2013100% (4)
- Plab Emergency Medicine CompleteDocument141 pagesPlab Emergency Medicine CompleteSyedKashifAli100% (1)
- MCQ Base For Final Exam PreparationDocument131 pagesMCQ Base For Final Exam PreparationPurwa Rane100% (1)
- Gastrointestinal DisordersDocument118 pagesGastrointestinal DisordersAhmad MakhloufNo ratings yet
- Chapter Six: Dha Assessment: Healthcare Professional Licensing Guide - 2013Document11 pagesChapter Six: Dha Assessment: Healthcare Professional Licensing Guide - 2013mnshzz0% (2)
- ABG Interpretation in PlabDocument11 pagesABG Interpretation in PlabRevant AgarwalNo ratings yet
- A Brief Introduction to the Multi-Specialty Recruitment Assessment (MSRA)From EverandA Brief Introduction to the Multi-Specialty Recruitment Assessment (MSRA)Rating: 5 out of 5 stars5/5 (1)
- Passmedicine MRCP Notes-Palliative Medicine and End of Life CareDocument5 pagesPassmedicine MRCP Notes-Palliative Medicine and End of Life CareMayar WaelNo ratings yet
- MCQ Paper 2016 NZDocument53 pagesMCQ Paper 2016 NZPeter Osundwa KitekiNo ratings yet
- Prometric Exam Collection: S - Page 1Document71 pagesPrometric Exam Collection: S - Page 1Edwin RajNo ratings yet
- PASSMED MRCP MCQs-PSYCHIATRYDocument33 pagesPASSMED MRCP MCQs-PSYCHIATRYStarlightNo ratings yet
- Dha TipsDocument4 pagesDha TipsSunil Wesley0% (2)
- Aga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsDocument12 pagesAga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsYasir QureshiNo ratings yet
- Drugs Affecting Neurologic SystemDocument5 pagesDrugs Affecting Neurologic SystemjustineGREATNo ratings yet
- Masterclass Book Part 2Document367 pagesMasterclass Book Part 2Eng Kian Ng100% (5)
- Clinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsDocument26 pagesClinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsNadia Ancharuz100% (1)
- ETG-Australian Therapeutic Guidelines 2020 (Part 2) .PDF - OptimizeDocument1,269 pagesETG-Australian Therapeutic Guidelines 2020 (Part 2) .PDF - OptimizeFlavin AmbroseNo ratings yet
- Medical Revision PaperDocument106 pagesMedical Revision PaperDavin SugumarNo ratings yet
- Prescription Writing HypertensionDocument18 pagesPrescription Writing HypertensionSAHILA SHEIKHNo ratings yet
- Antipsychotics MCQ's PDFDocument21 pagesAntipsychotics MCQ's PDFPauline Tendai Maniki100% (6)
- SMLE 2022 - GuideDocument41 pagesSMLE 2022 - Guidefouad tabetNo ratings yet
- Chapter 6 - Self-Assessment Q&ADocument8 pagesChapter 6 - Self-Assessment Q&AVijay Sharma100% (1)
- UQU SLE CORRECTED FILE by DR Samina FidaDocument537 pagesUQU SLE CORRECTED FILE by DR Samina Fidaasma .sassi100% (1)
- Git Exam 2015 PDFDocument50 pagesGit Exam 2015 PDFIbrahim BarhamNo ratings yet
- Family Medicine - General Practice MEQ 2006Document6 pagesFamily Medicine - General Practice MEQ 2006jermie22100% (1)
- Real Exam Ethics OSCEDocument3 pagesReal Exam Ethics OSCEmonica ortizNo ratings yet
- Plab 2 Recall 5Document137 pagesPlab 2 Recall 5Sadiya IslamNo ratings yet
- Passmedicine MRCP Mcqs-Clinical Pharmacology and ToxicologyDocument135 pagesPassmedicine MRCP Mcqs-Clinical Pharmacology and ToxicologyHashim Ahmad100% (1)
- MCQS Dr. AaliaDocument8 pagesMCQS Dr. AaliarawalianNo ratings yet
- Pharmacology Viva QuestionsDocument1 pagePharmacology Viva Questionsmaheen_ju100% (2)
- Haad Exam 1-2014Document10 pagesHaad Exam 1-2014jishan82No ratings yet
- 100 BCQ MRCP QuestionsDocument31 pages100 BCQ MRCP QuestionsMatin Ahmad Khan100% (1)
- Racgp Combined Pdfs Single FileDocument1,983 pagesRacgp Combined Pdfs Single FileVikrant100% (1)
- INTERNAL MEDICINE - Cardiovascular SystemDocument8 pagesINTERNAL MEDICINE - Cardiovascular SystemAiswaryaNo ratings yet
- Dha Prometric Feb-3 ShabeerDocument2 pagesDha Prometric Feb-3 ShabeerDr-Usman KhanNo ratings yet
- 1 ❤ Smart Sheet for History Taking in Internal Medicine خلفية سماويةDocument12 pages1 ❤ Smart Sheet for History Taking in Internal Medicine خلفية سماويةOsama A100% (1)
- MCQS Dr. Aalia New 31 October 2008Document4 pagesMCQS Dr. Aalia New 31 October 2008rawalianNo ratings yet
- ACP Board Review Nephrology 20052ndDocument35 pagesACP Board Review Nephrology 20052nddoctormido2010100% (1)
- Board Review 03Document28 pagesBoard Review 03julianzunigaNo ratings yet
- Pastest 1Document76 pagesPastest 1Hengameh JavaheryNo ratings yet
- Case Conference - FinalDocument8 pagesCase Conference - FinalNiña Lyn Paican PonlaNo ratings yet
- Diabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Side Effects of Common Drugs PDFDocument2 pagesSide Effects of Common Drugs PDFImran ChaudhryNo ratings yet
- Side Effects of Common Drugs PDFDocument2 pagesSide Effects of Common Drugs PDFImran ChaudhryNo ratings yet
- Drug Monitoring PDFDocument1 pageDrug Monitoring PDFImran ChaudhryNo ratings yet
- Topics Mcqs % Days Pages % DaysDocument2 pagesTopics Mcqs % Days Pages % DaysImran ChaudhryNo ratings yet
- Acute Management of Nephrolithiasis in Children - UpToDateDocument15 pagesAcute Management of Nephrolithiasis in Children - UpToDatedrtgodeNo ratings yet
- Spa PPT - FinalDocument45 pagesSpa PPT - FinalShivam DwivediNo ratings yet
- PcolDocument17 pagesPcolThea JulianaNo ratings yet
- Introduction and Overview of The Report: Chapter 1 PreviewDocument33 pagesIntroduction and Overview of The Report: Chapter 1 PreviewAnonymous GF8PPILW5No ratings yet
- Thesis Statement For Pain ManagementDocument4 pagesThesis Statement For Pain Managementgjdpj4jq100% (1)
- CompetitiveStrategy Dolmo PeDocument39 pagesCompetitiveStrategy Dolmo PenoqlwnNo ratings yet
- The Role of THR Operating Suite PharmacistDocument59 pagesThe Role of THR Operating Suite PharmacistRheinny IndrieNo ratings yet
- Drug Study - Morphine (Sulfate)Document3 pagesDrug Study - Morphine (Sulfate)Kian Herrera100% (2)
- Premedication: AnxietyDocument2 pagesPremedication: AnxietyMuhammad Afandy PulualaNo ratings yet
- Anesthesia Guide VASG 12-4-04Document164 pagesAnesthesia Guide VASG 12-4-04Radu TudorNo ratings yet
- Anesthesiology SamplexDocument17 pagesAnesthesiology SamplexAudrey CobankiatNo ratings yet
- Pain Management For Medical StudentsDocument37 pagesPain Management For Medical Studentsamq aloqiliNo ratings yet
- Article 1: Weed Vs Opioids: Which Is Better For Pain?: Prevent Pain in Different WaysDocument11 pagesArticle 1: Weed Vs Opioids: Which Is Better For Pain?: Prevent Pain in Different WaysdoraemonNo ratings yet
- Prescription DrugsDocument20 pagesPrescription DrugsChelsea GraceNo ratings yet
- Goljan High Yield PharmaDocument9 pagesGoljan High Yield Pharmahabdulhye100% (1)
- Toprank Nursing: Patrick Migel Mercado, RNDocument126 pagesToprank Nursing: Patrick Migel Mercado, RNNoreen PadillaNo ratings yet
- Drug Education and Vice Control (Without L.A)Document71 pagesDrug Education and Vice Control (Without L.A)Sheila May Credo-CagandahanNo ratings yet
- Identification of Pharmacological Inducers of A Reversible Hypometabolic State For Whole Organ PreservationDocument39 pagesIdentification of Pharmacological Inducers of A Reversible Hypometabolic State For Whole Organ PreservationGraciano emilio VaquinaNo ratings yet
- Reptile Anesthesia and AnalgesiaDocument43 pagesReptile Anesthesia and AnalgesiaEric CheahNo ratings yet
- Drug StudyDocument6 pagesDrug StudyGenny Lou Lumacang OriasNo ratings yet
- The Analgesic Efcacy of Bilateral Superfcial Cervical Plexus Block For Thyroid Surgery Under General AnesthesiaDocument6 pagesThe Analgesic Efcacy of Bilateral Superfcial Cervical Plexus Block For Thyroid Surgery Under General AnesthesiaCristina RamirezNo ratings yet
- OsteomyelitisDocument42 pagesOsteomyelitisKayetano Punla PanganNo ratings yet
- Marketing DemoDocument14 pagesMarketing DemoShamim Ahamed ShakilNo ratings yet
- Essay (Effect of Drug Abuse)Document13 pagesEssay (Effect of Drug Abuse)Pius AbidakunNo ratings yet
- STG General HospitalDocument682 pagesSTG General HospitalhaalefomNo ratings yet
- The Moral Hazard of Lifesaving Innovations: Naloxone Access, Opioid Abuse, and CrimeDocument67 pagesThe Moral Hazard of Lifesaving Innovations: Naloxone Access, Opioid Abuse, and CrimeepraetorianNo ratings yet
- Fentanyl Analouge SynthDocument11 pagesFentanyl Analouge SynthamesffNo ratings yet
- Case AppendicitisDocument112 pagesCase AppendicitisChen CobainNo ratings yet
- Drugs of Abuse: Evelyn B. Yumiaco M.D. Department of Pharmacology School of Medicine Angeles University FoundationDocument92 pagesDrugs of Abuse: Evelyn B. Yumiaco M.D. Department of Pharmacology School of Medicine Angeles University FoundationBenjamin PrabhuNo ratings yet
- Pharmacognosy Assignment 2Document13 pagesPharmacognosy Assignment 2Saud AlamNo ratings yet