Download as pdf or txt
You might also like
- 1.5.2.3.00102 Reagent Insert Kit CRPDocument2 pages1.5.2.3.00102 Reagent Insert Kit CRPenoen_risa902883% (6)
- Regulation of Tissue Oxygenation: Second EditionDocument114 pagesRegulation of Tissue Oxygenation: Second EditionrezqNo ratings yet
- Classical Music Therapy As The Intervention To Relieve Headache in ADocument3 pagesClassical Music Therapy As The Intervention To Relieve Headache in AmargaretNo ratings yet
- Pubarticlegingivaoxygenation PDFDocument5 pagesPubarticlegingivaoxygenation PDFAhmed BadrNo ratings yet
- Research Paper On OxygenDocument5 pagesResearch Paper On Oxygenegya6qzc100% (1)
- Source 3Document2 pagesSource 3api-243328873No ratings yet
- Walsh Oxygen TheraoyDocument18 pagesWalsh Oxygen TheraoyelfiahNo ratings yet
- Collins2015 - Relating Oxygen Partial Pressure, Saturation and Content The Hb-Oxy Dissociation CurveDocument8 pagesCollins2015 - Relating Oxygen Partial Pressure, Saturation and Content The Hb-Oxy Dissociation CurveDinNo ratings yet
- Therapeuric GassesDocument3 pagesTherapeuric GassesAoun EmpNo ratings yet
- Term Paper On OxygenDocument7 pagesTerm Paper On Oxygenauhavmpif100% (1)
- Review: Running Head: Nitric Oxide and Energy Balance in HypoxiaDocument70 pagesReview: Running Head: Nitric Oxide and Energy Balance in HypoxiaAprilihardini LaksmiNo ratings yet
- Oxidante AntioxidanteDocument8 pagesOxidante AntioxidanteJuan Felipe CifuentesNo ratings yet
- Cells 11 00978Document12 pagesCells 11 00978wcswcsNo ratings yet
- Improvement of Fermentation Performance of Gluconobacter Oxydans by Combination of Enhanced Oxygen Mass Transfer in Compressed-Oxygen-Supplied Sealed System and Cell-Recycle Techni..Document6 pagesImprovement of Fermentation Performance of Gluconobacter Oxydans by Combination of Enhanced Oxygen Mass Transfer in Compressed-Oxygen-Supplied Sealed System and Cell-Recycle Techni..Rosyida Ismi (Rosyi)No ratings yet
- Biochemical and Physiological Effect of Silver BioDocument17 pagesBiochemical and Physiological Effect of Silver BioVILEOLAGOLDNo ratings yet
- Physiology, Oxygen Transport: April 2019Document5 pagesPhysiology, Oxygen Transport: April 2019Soha SonaNo ratings yet
- Grade 11 Life Sciences Remote Learning Booklet - Term 3 & 4Document91 pagesGrade 11 Life Sciences Remote Learning Booklet - Term 3 & 4destineemande07No ratings yet
- Oxygen in Culture Media PDFDocument6 pagesOxygen in Culture Media PDFSiko NcembuNo ratings yet
- Mitochondrial Respiration and Redox Coupling in Articular ChondrocytesDocument14 pagesMitochondrial Respiration and Redox Coupling in Articular ChondrocytesndsjNo ratings yet
- Final Capstone Paper - Rayan SamaouiDocument17 pagesFinal Capstone Paper - Rayan Samaouiapi-750186768No ratings yet
- Aplicacao Do Ozonio Na MedicinaDocument12 pagesAplicacao Do Ozonio Na MedicinaJoão Jacques Legatti100% (1)
- The Rate of Oxygen Utilization by CellsDocument32 pagesThe Rate of Oxygen Utilization by CellsMariano PerezNo ratings yet
- The Oxygen Therapy: Current Medicinal Chemistry January 2013Document25 pagesThe Oxygen Therapy: Current Medicinal Chemistry January 2013Violeta TamarovaNo ratings yet
- 2016 Article 23Document8 pages2016 Article 23lathifatulNo ratings yet
- CoQ10 and The Treatment of PeriodontitisDocument8 pagesCoQ10 and The Treatment of Periodontitismichael DariasNo ratings yet
- Ajpheart 01030 2002Document8 pagesAjpheart 01030 2002aguslistyNo ratings yet
- Blood Gas Analysis For Bedside DiagnosisDocument6 pagesBlood Gas Analysis For Bedside DiagnosisMuhamad Wirawan AdityoNo ratings yet
- Modelling Microalgal Activity As A Function of Inorganic Carbon Concentration: Accounting For The Impact of PH On The Bicarbonate SystemDocument9 pagesModelling Microalgal Activity As A Function of Inorganic Carbon Concentration: Accounting For The Impact of PH On The Bicarbonate Systemdandikelana29No ratings yet
- Molecular Origin of The Elastic State of Aqueous HA (G. Giubertoni - 2019)Document7 pagesMolecular Origin of The Elastic State of Aqueous HA (G. Giubertoni - 2019)lejartkNo ratings yet
- Biotechnology ReportsDocument9 pagesBiotechnology ReportsNurkholis Bin AbdulNo ratings yet
- Dental Caries From A Molecular Microbiological PerspectiveDocument15 pagesDental Caries From A Molecular Microbiological PerspectiveMedical TubeNo ratings yet
- 2016analysis of Plasma Lipid Peroxidation and Antioxidant Enzymes Status in Patients of Oral Leukoplakia A Case Control StudyDocument6 pages2016analysis of Plasma Lipid Peroxidation and Antioxidant Enzymes Status in Patients of Oral Leukoplakia A Case Control StudyDr. DeeptiNo ratings yet
- Vias Moleculares EritrocitariasDocument18 pagesVias Moleculares EritrocitariasBruna CarvalhoNo ratings yet
- Dien Hoa-Sensor 2020Document15 pagesDien Hoa-Sensor 2020Kim ThắmNo ratings yet
- The Effffect of Nitric o Ide On Mitochondrial RespirationDocument23 pagesThe Effffect of Nitric o Ide On Mitochondrial RespirationDaniel Amaro VillajulcaNo ratings yet
- Chemie Ingenieur Technik - 2020 - Seidel - Oxygen Mass Transfer in Biopharmaceutical Processes Numerical and ExperimentalDocument20 pagesChemie Ingenieur Technik - 2020 - Seidel - Oxygen Mass Transfer in Biopharmaceutical Processes Numerical and Experimentalmike maoNo ratings yet
- Scientific PaperDocument14 pagesScientific PaperAhmed Hamdy KhattabNo ratings yet
- JBJSDocument8 pagesJBJSDr Aleksandar DejanovicNo ratings yet
- Effect HyperbaricDocument7 pagesEffect HyperbaricdeffyNo ratings yet
- A Review of Hydrogen As A New Medical TherapyDocument8 pagesA Review of Hydrogen As A New Medical TherapyfooykokNo ratings yet
- 01 ATV 0000249408 55796 DaDocument8 pages01 ATV 0000249408 55796 DaSvetlana Khyn SeseNo ratings yet
- Calcium Hydroxide - A Great Calcific WallDocument5 pagesCalcium Hydroxide - A Great Calcific WallAki AvlonNo ratings yet
- Objectives of Hemodynamic Resuscitation: Update IN Intensive Care: Hemodynamic Monitoring IN THE Critically ILL PatientDocument10 pagesObjectives of Hemodynamic Resuscitation: Update IN Intensive Care: Hemodynamic Monitoring IN THE Critically ILL PatientMateoZuluagaGomezNo ratings yet
- Dissolved Oxygen Research PaperDocument7 pagesDissolved Oxygen Research Paperfvjebmpk100% (1)
- Biomineralogy of Angiogenesis PDFDocument7 pagesBiomineralogy of Angiogenesis PDFFortune JournalsNo ratings yet
- Physiology of Oxygen TransportDocument8 pagesPhysiology of Oxygen TransportAldo FebrianNo ratings yet
- Hydrogen Sulfide and Mitochondria: ReviewsDocument13 pagesHydrogen Sulfide and Mitochondria: ReviewsАнна ШаповаловаNo ratings yet
- Biochem Week 1Document17 pagesBiochem Week 1divineNo ratings yet
- Donors and RoleDocument17 pagesDonors and RoleAbubakar BelloNo ratings yet
- Anti-Cancer Effects of Cerium Oxide Nanoparticles and Its Intracellular Redox ActivityDocument9 pagesAnti-Cancer Effects of Cerium Oxide Nanoparticles and Its Intracellular Redox ActivityBashar AliNo ratings yet
- Effects of Co2Document62 pagesEffects of Co2satish cooperNo ratings yet
- Limitaciones Oximetria 20Document6 pagesLimitaciones Oximetria 20Henry CruzNo ratings yet
- The Relationship Between Oxidant-Antioxidant Status and Bronchial Obstructive Parameters in Patients With COPDDocument4 pagesThe Relationship Between Oxidant-Antioxidant Status and Bronchial Obstructive Parameters in Patients With COPDOyunbiligt BaatarNo ratings yet
- Micromachines 12 01251Document25 pagesMicromachines 12 01251distributor.company.ivanovoNo ratings yet
- Cellulose ThesisDocument8 pagesCellulose Thesisfjdxfc4v100% (2)
- Hyperbaric Oxygen: Its Mechanisms and Efficacy: BackgroundDocument11 pagesHyperbaric Oxygen: Its Mechanisms and Efficacy: BackgroundCicing NasklengNo ratings yet
- The Red Cell Storage Lesion andDocument12 pagesThe Red Cell Storage Lesion andhasanahNo ratings yet
- Carboxytherapy Non Invasive Method in DermatologyDocument7 pagesCarboxytherapy Non Invasive Method in DermatologyAmir Hossein AmiriNo ratings yet
- UR V8 ISS1-2 2to8Document7 pagesUR V8 ISS1-2 2to8Richar Tomy TNo ratings yet
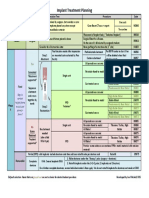
- Implant TX Plan GridDocument1 pageImplant TX Plan GridAhmed BadrNo ratings yet
- Ijdr 12414Document5 pagesIjdr 12414Ahmed BadrNo ratings yet
- 6038ed9dcef5d IJAR-35170Document5 pages6038ed9dcef5d IJAR-35170Ahmed BadrNo ratings yet
- M Vista in Class 3Document12 pagesM Vista in Class 3Ahmed BadrNo ratings yet
- MetaanalysisDocument12 pagesMetaanalysisAhmed BadrNo ratings yet
- Prognosis 2021Document10 pagesPrognosis 2021Ahmed BadrNo ratings yet
- 5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Document21 pages5ce2249c7c5e2f337802a9e5 - JIACD Sticky Bone December 2015Ahmed BadrNo ratings yet
- PlateletFunctionTesting FINAL PDFDocument14 pagesPlateletFunctionTesting FINAL PDFAhmed BadrNo ratings yet
- Korkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeDocument10 pagesKorkmaz-Balli2021 Article ClinicalEvaluationOfTheTreatmeAhmed BadrNo ratings yet
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- 3A 2B Immediate ImplantDocument6 pages3A 2B Immediate ImplantAhmed BadrNo ratings yet
- Content ServerDocument10 pagesContent ServerAhmed BadrNo ratings yet
- 22 CE CreditsDocument11 pages22 CE CreditsAhmed BadrNo ratings yet
- Medical Hypotheses: Letter To EditorsDocument2 pagesMedical Hypotheses: Letter To EditorsAhmed BadrNo ratings yet
- Guidelines For Immediate ImplanttDocument11 pagesGuidelines For Immediate ImplanttAhmed BadrNo ratings yet
- Periodontal Plastic Surgery For The Management of Altered Passive EruptionDocument3 pagesPeriodontal Plastic Surgery For The Management of Altered Passive EruptionAhmed BadrNo ratings yet
- Sickle - Cell - Guidelines TTTDocument2 pagesSickle - Cell - Guidelines TTTAhmed BadrNo ratings yet
- 2010 Sofia Aroca SoteloDocument52 pages2010 Sofia Aroca SoteloAhmed BadrNo ratings yet
- A Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureDocument11 pagesA Modified Suture Technique For Plastic Periodontal and Implant Surgery-The Double-Crossed SutureAhmed BadrNo ratings yet
- Pubarticlegingivaoxygenation PDFDocument5 pagesPubarticlegingivaoxygenation PDFAhmed BadrNo ratings yet
- Multiple Choice Questions-Mechanical Plaque ControlDocument12 pagesMultiple Choice Questions-Mechanical Plaque ControlAhmed BadrNo ratings yet
- 22 Jispwidthofattachedgingiva PDFDocument5 pages22 Jispwidthofattachedgingiva PDFAhmed BadrNo ratings yet
- Bone Loss&Patterns of Bone Destruction: Bone Distruction Due ToDocument23 pagesBone Loss&Patterns of Bone Destruction: Bone Distruction Due ToAhmed BadrNo ratings yet
- Furcation 31 12 14Document25 pagesFurcation 31 12 14Ahmed BadrNo ratings yet
- Furcation 31 12 14Document25 pagesFurcation 31 12 14Ahmed BadrNo ratings yet
- Saudi ExamDocument201 pagesSaudi ExamAhmed Badr100% (5)
- Aloe Vera Benefits & Information (Aloe Barbadensis)Document5 pagesAloe Vera Benefits & Information (Aloe Barbadensis)ygjyoNo ratings yet
- DAFTAR PUSTAKA CHFDocument39 pagesDAFTAR PUSTAKA CHFiganuryantiNo ratings yet
- Presentation Auto 2Document33 pagesPresentation Auto 2mlllNo ratings yet
- модуль варіант №3 контрольDocument8 pagesмодуль варіант №3 контрольShambhu AshokNo ratings yet
- Mimickers of UrticariaDocument9 pagesMimickers of UrticariaNaeNo ratings yet
- Metal and The SkinDocument441 pagesMetal and The SkinAGUSTONI pUJIATO100% (2)
- Physical Therapy Approaches For Wound CareDocument94 pagesPhysical Therapy Approaches For Wound CarewirdhaNo ratings yet
- 5 6337055981314245059Document498 pages5 6337055981314245059A.c. RaghuNo ratings yet
- GastritisDocument13 pagesGastritisDewi RosalindaNo ratings yet
- Intel STS Semifinalists 2016Document32 pagesIntel STS Semifinalists 2016BayAreaNewsGroupNo ratings yet
- KURNIK Et Al 2010 HaemophiliaDocument7 pagesKURNIK Et Al 2010 HaemophiliaAna-Maria MarcuNo ratings yet
- Role of Neutrophils in Periodontal DiseaseDocument65 pagesRole of Neutrophils in Periodontal DiseaseGaurav Phaphriya40% (5)
- Immunity (Lecture Notes)Document5 pagesImmunity (Lecture Notes)Anisha NishanthNo ratings yet
- NRDPUlcerative Colitis PDFDocument21 pagesNRDPUlcerative Colitis PDFLuminita HutanuNo ratings yet
- Skin Innervation: Important Roles During Normal and Pathological Cutaneous RepairDocument19 pagesSkin Innervation: Important Roles During Normal and Pathological Cutaneous RepairafbmgNo ratings yet
- Malnutrition: Undernutrition - Simple and Stress StarvationDocument9 pagesMalnutrition: Undernutrition - Simple and Stress StarvationDini Fajriah OmariNo ratings yet
- BambooDocument6 pagesBambooShabbir AliNo ratings yet
- Chapter 22 (Excerpt From Feel Good Nutrigenomics: Your Roadmap To Health)Document16 pagesChapter 22 (Excerpt From Feel Good Nutrigenomics: Your Roadmap To Health)Dr. Amy Yasko100% (3)
- Aloe Vera MiracleDocument20 pagesAloe Vera Miracleanon-287110100% (19)
- Rheumatoid ArthritisDocument29 pagesRheumatoid ArthritisvijitajayaminiNo ratings yet
- Shalu Bathla - Textbook of Periodontics-Jaypee Brothers, Medical Publishers Pvt. Ltd. (2017)Document818 pagesShalu Bathla - Textbook of Periodontics-Jaypee Brothers, Medical Publishers Pvt. Ltd. (2017)Vonny MariaNo ratings yet
- EBSCOhost 3 PDFDocument27 pagesEBSCOhost 3 PDFWawan Febri RamdaniNo ratings yet
- Earthing: Health Implications of Reconnecting The Human Body To The Earth's Surface ElectronsDocument9 pagesEarthing: Health Implications of Reconnecting The Human Body To The Earth's Surface ElectronsgilsonrossatoNo ratings yet
- Salus Silver TSL2 - FormattedDocument52 pagesSalus Silver TSL2 - Formattedhilajo1363No ratings yet
- Gut Bacteria in Health and DiseaseDocument10 pagesGut Bacteria in Health and DiseasevvvNo ratings yet
- ArthrocentesisDocument10 pagesArthrocentesisPranave PNo ratings yet
- Prof. Marco GiammancoDocument159 pagesProf. Marco GiammancomarcogiammancoNo ratings yet
- Critical Care AnesthesiaDocument451 pagesCritical Care AnesthesiaMichael Andrews100% (7)