Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Biopsychology Global Edition 11Th Ed John Pinel Full ChapterDocument67 pagesBiopsychology Global Edition 11Th Ed John Pinel Full Chaptereve.sampson31489% (9)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- ECT Manual-NIMHANS Ed.2 Compressed-2Document70 pagesECT Manual-NIMHANS Ed.2 Compressed-2Utkarsh Modi50% (6)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MCQ AnswersDocument2 pagesMCQ AnswersJeyarajasekar TtrNo ratings yet
- Lifeflow BrainwavesDocument3 pagesLifeflow BrainwavesIulian GavrilovNo ratings yet
- ۔ماہنامہ الہلال۔۔شعبان المعظم 1442ھ PDFDocument95 pages۔ماہنامہ الہلال۔۔شعبان المعظم 1442ھ PDFMuhammad WajahatNo ratings yet
- Assignment 2: Mri MachineDocument6 pagesAssignment 2: Mri MachineMuhammad WajahatNo ratings yet
- Assignment 3 AishaDocument6 pagesAssignment 3 AishaMuhammad WajahatNo ratings yet
- STATISTICS 8 CHAPTERS 1 TO 6 SolveDocument8 pagesSTATISTICS 8 CHAPTERS 1 TO 6 SolveMuhammad WajahatNo ratings yet
- Anova: Overall Conclusion: Yes, After Applying The Two Way ANOVA We Find That There Is A Difference inDocument3 pagesAnova: Overall Conclusion: Yes, After Applying The Two Way ANOVA We Find That There Is A Difference inMuhammad WajahatNo ratings yet
- Mod 2Document30 pagesMod 2mailtopiyush18No ratings yet
- Jurnal 1 Ayudita Silvia HasibuanDocument6 pagesJurnal 1 Ayudita Silvia HasibuanParutigapuluh NovemberNo ratings yet
- Olbrich (2013) - EEG Biomarkers in Major DepressiveDocument15 pagesOlbrich (2013) - EEG Biomarkers in Major DepressiveJulieht RodriguezNo ratings yet
- The Brain and Introduction To EEG and FMRIDocument28 pagesThe Brain and Introduction To EEG and FMRIextraaforme932No ratings yet
- Quantifying Mental Relaxation With EEG For Use in Computer GamesDocument7 pagesQuantifying Mental Relaxation With EEG For Use in Computer GamesSoumitra KunduNo ratings yet
- Long-Term Outcome Characteristics in Mesial Temporal Lobe Epilepsy With and Without Associated Cortical DysplasiaDocument10 pagesLong-Term Outcome Characteristics in Mesial Temporal Lobe Epilepsy With and Without Associated Cortical DysplasiaGesael Passos Ferreira JuniorNo ratings yet
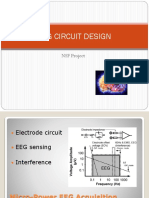
- Eeg Circuit Design: NSF ProjectDocument136 pagesEeg Circuit Design: NSF Projectrhycardo5902No ratings yet
- Concept of Using The Brain-Computer Interface To Control Hand ProsthesisDocument10 pagesConcept of Using The Brain-Computer Interface To Control Hand ProsthesisHayder AdnanNo ratings yet
- What Are Theta Brain WavesDocument7 pagesWhat Are Theta Brain WavesOttoNo ratings yet
- Similiarties and Differences Between StudiesDocument2 pagesSimiliarties and Differences Between Studieshudhudshahidaus13No ratings yet
- 1 s2.0 S0010482522003985 MainDocument12 pages1 s2.0 S0010482522003985 Mainahmed.mohammedNo ratings yet
- DR. DANIELA DENTICO (Orcid ID: 0000-0003-1050-0327) Article Type: Research ReportDocument24 pagesDR. DANIELA DENTICO (Orcid ID: 0000-0003-1050-0327) Article Type: Research ReportTanushree BNo ratings yet
- OpenViBE Basics Tutorial PDFDocument101 pagesOpenViBE Basics Tutorial PDFRogersCardenasMogollonNo ratings yet
- The Utility of Non-Invasive Brain Stimulation in RDocument10 pagesThe Utility of Non-Invasive Brain Stimulation in RsanagaumiNo ratings yet
- Wireless Monitoring of Physiological Data Using Nexus-10 & BiotraceDocument64 pagesWireless Monitoring of Physiological Data Using Nexus-10 & BiotraceInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Full Chapter Analyzing A Long Dream Series What Can We Learn About How Dreaming Works 1St Edition Michael Schredl PDFDocument53 pagesFull Chapter Analyzing A Long Dream Series What Can We Learn About How Dreaming Works 1St Edition Michael Schredl PDFlorena.ballard933100% (5)
- Evaluation of Consumer Grade EEG Headsets For BCI PDFDocument6 pagesEvaluation of Consumer Grade EEG Headsets For BCI PDFAvionicsNo ratings yet
- Seminar Report by Shashank AroraDocument33 pagesSeminar Report by Shashank AroraSanjay JangidNo ratings yet
- AP Holosync Solution Booklet Final Digital CompressedDocument64 pagesAP Holosync Solution Booklet Final Digital CompressedIanNo ratings yet
- Consequences of Sleep DeprivationDocument20 pagesConsequences of Sleep DeprivationAnonymous IXCgBcmXNo ratings yet
- Pediatric PolysomnographyDocument7 pagesPediatric Polysomnographysavvy_as_98-1No ratings yet
- Neurofeedback Technician Module 2 TrainingDocument25 pagesNeurofeedback Technician Module 2 TrainingborzupazhuhanNo ratings yet
- Neurophysiologic Basis of EEG and DC Potentials: Neuronal Membrane Potentials: Intracellular RecordingsDocument16 pagesNeurophysiologic Basis of EEG and DC Potentials: Neuronal Membrane Potentials: Intracellular RecordingsPolina HomyakovaNo ratings yet
- Nerve & Cardiac Impulse Eb Kns 2018Document78 pagesNerve & Cardiac Impulse Eb Kns 2018Lalitaditya DivakarlaNo ratings yet
- Curs 2 NeuroimagisticaDocument116 pagesCurs 2 NeuroimagisticaLucia NegruNo ratings yet
- Biblio RavenDocument60 pagesBiblio RavenSimon BenjaminNo ratings yet