Download as pdf or txt
You might also like
- List of Specific Brainwave Frequency BenefitsDocument6 pagesList of Specific Brainwave Frequency BenefitsBen Natale100% (11)
- Infertility: Dr. Carolina Paula C. MartinDocument6 pagesInfertility: Dr. Carolina Paula C. MartinMaikka IlaganNo ratings yet
- DISC, Drugs, Infection, Thick Basal MembraneDocument5 pagesDISC, Drugs, Infection, Thick Basal MembraneHOPENo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- HerniaDocument5 pagesHerniasarguss14100% (5)
- Lec 2 - Blood VesselsDocument12 pagesLec 2 - Blood VesselsJeffrey LübbertNo ratings yet
- Vasculitis MindnodeDocument1 pageVasculitis MindnodeToño VargasNo ratings yet
- Polycystic Kidney DiseaseDocument9 pagesPolycystic Kidney DiseaseCésar Aguilar ContrerasNo ratings yet
- Pedia Finals ReviewerDocument9 pagesPedia Finals ReviewerMarron Jane GanoticeNo ratings yet
- Shanz - Pedia Ii 2.05Document3 pagesShanz - Pedia Ii 2.05Petrina XuNo ratings yet
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocument10 pages(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanNo ratings yet
- Cerebral PalsyDocument14 pagesCerebral PalsyWaode SittrisnawatiNo ratings yet
- Gyne ReflectionDocument18 pagesGyne ReflectionKC Dela RosaNo ratings yet
- Dermatology Biologics Boards Fodder DIR Winter 2017Document6 pagesDermatology Biologics Boards Fodder DIR Winter 2017riskhakov100% (1)
- Shanz - Pedia 1.04Document8 pagesShanz - Pedia 1.04Petrina XuNo ratings yet
- Dengue Virus: DescriptionDocument12 pagesDengue Virus: Descriptionpedia blue bookNo ratings yet
- Prostate GlandsDocument3 pagesProstate GlandsDragan PetrovicNo ratings yet
- Distal To Ligament of Treitz: CausesDocument8 pagesDistal To Ligament of Treitz: CausesKiara GovenderNo ratings yet
- (Surg2) 5.3 Urology Part 2 - Dr. YusiDocument19 pages(Surg2) 5.3 Urology Part 2 - Dr. YusiAlloiBialbaNo ratings yet
- Hernias: Mark A. Malangoni, Michael J. RosenDocument28 pagesHernias: Mark A. Malangoni, Michael J. RosenHenryOeiNo ratings yet
- Ob Finals Williams SamplexDocument86 pagesOb Finals Williams SamplexJustine MembridoNo ratings yet
- Disease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesDocument11 pagesDisease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesSara AshurstNo ratings yet
- 4 PEDIA 8 - Bleeding DisordersDocument5 pages4 PEDIA 8 - Bleeding DisordersRainy Liony DuhNo ratings yet
- Vasculitis ReviewDocument132 pagesVasculitis Reviewajmal_rashid@hotmail.com100% (2)
- Abdominal Mass Differential PresentationDocument42 pagesAbdominal Mass Differential Presentationdeb haartNo ratings yet
- GYNE 4.01b InfertilityDocument4 pagesGYNE 4.01b InfertilityGray SnellNo ratings yet
- Types of Arthritis: SOLOMON SALLFORSDocument3 pagesTypes of Arthritis: SOLOMON SALLFORSSolomon Seth SallforsNo ratings yet
- Precocius PubertyDocument4 pagesPrecocius PubertyJoanne LimNo ratings yet
- Gynecology: 3.09 - AmenorrheaDocument13 pagesGynecology: 3.09 - AmenorrheaAnna Mae MarantanNo ratings yet
- Embryology of The EarDocument3 pagesEmbryology of The EarJem MontañaNo ratings yet
- Surgical Anatomy of The Chest Wall, Pleura, and MediastinumDocument8 pagesSurgical Anatomy of The Chest Wall, Pleura, and MediastinumNooneNo ratings yet
- ENDOCRINE PATHOLOGY WebpathDocument35 pagesENDOCRINE PATHOLOGY Webpathapi-3766657No ratings yet
- Legal Medicine Review PDFDocument10 pagesLegal Medicine Review PDFGhie TangonanNo ratings yet
- Dse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesDocument5 pagesDse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesLuka Desabelle- JustoNo ratings yet
- GYNE 4.05a Bening Ang Malignant Lesions of The VulvaDocument11 pagesGYNE 4.05a Bening Ang Malignant Lesions of The VulvaGray SnellNo ratings yet
- Part 1Document58 pagesPart 1Abdulrahman KatibNo ratings yet
- Trans Congenital MalformationsDocument10 pagesTrans Congenital MalformationsRemelou Garchitorena AlfelorNo ratings yet
- Lower Gi Case Presentation PDFDocument35 pagesLower Gi Case Presentation PDFapi-448999672No ratings yet
- Herpes Simplex Virus: 2 SerotypesDocument18 pagesHerpes Simplex Virus: 2 Serotypespedia blue bookNo ratings yet
- Anatomy of The Nose & Paranasal Air SinusesDocument4 pagesAnatomy of The Nose & Paranasal Air SinusesMusfique RashidNo ratings yet
- 1 Benign and Malignant Lesions of The CervixDocument46 pages1 Benign and Malignant Lesions of The CervixRohitNo ratings yet
- (SURG) 5.4b Management of Soft Tissue SarcomaDocument6 pages(SURG) 5.4b Management of Soft Tissue SarcomaKenneth TorresNo ratings yet
- ENT 1.2 Diseases of The Nose, Paranasal Sinuses, and Face PDFDocument18 pagesENT 1.2 Diseases of The Nose, Paranasal Sinuses, and Face PDFZazaNo ratings yet
- Fammed Family Life CycleDocument3 pagesFammed Family Life CycleTMC PGI GENER MICKONo ratings yet
- Vulval CaDocument54 pagesVulval CaChethana BhatNo ratings yet
- Pathophysiology: Rectal CarcinomaDocument25 pagesPathophysiology: Rectal CarcinomaCristina CristinaNo ratings yet
- Breech Delivery and Vacuum ExtractionDocument71 pagesBreech Delivery and Vacuum ExtractionRendy Adhitya PratamaNo ratings yet
- ENT Benign Neck MassesDocument2 pagesENT Benign Neck MassesLucyellowOttemoesoeNo ratings yet
- Pedia Bacte Table 08amDocument25 pagesPedia Bacte Table 08ampedia blue bookNo ratings yet
- Gyne Case COCDocument37 pagesGyne Case COCLian BaylosisNo ratings yet
- PEDIA para 08AMDocument17 pagesPEDIA para 08AMpedia blue bookNo ratings yet
- Case On Upper GI Bleeding: Interns Chua, EsquidaDocument59 pagesCase On Upper GI Bleeding: Interns Chua, EsquidaJoyce ChuaNo ratings yet
- Gynecology: Recurrent Pregnancy LossDocument6 pagesGynecology: Recurrent Pregnancy LossDawn Marco100% (1)
- Differential Diagnosis Fever With RashDocument15 pagesDifferential Diagnosis Fever With RashJeetat OngNo ratings yet
- Approach To Anemia: - Reticulocyte Count Is Most Important TestDocument15 pagesApproach To Anemia: - Reticulocyte Count Is Most Important TestJanella SuerteNo ratings yet
- Lupus Case PresentationDocument48 pagesLupus Case PresentationRoscelie KhoNo ratings yet
- Benign Gynecologic TumorsDocument57 pagesBenign Gynecologic TumorsDexter IanNo ratings yet
- Gastrointestinal Diseases Part1Document7 pagesGastrointestinal Diseases Part1sarguss14100% (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoNo ratings yet
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocument7 pagesDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (2)
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoNo ratings yet
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoNo ratings yet
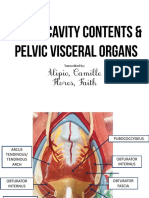
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoNo ratings yet
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoNo ratings yet
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoNo ratings yet
- Child PsychiatryDocument6 pagesChild PsychiatryVon HippoNo ratings yet
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoNo ratings yet
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoNo ratings yet
- 1) Any Medical Student or GraduateDocument27 pages1) Any Medical Student or GraduateVon HippoNo ratings yet
- Abdominal: Al HerniaDocument3 pagesAbdominal: Al HerniaVon Hippo100% (1)
- Fluid and Electrolytes YMDocument8 pagesFluid and Electrolytes YMVon HippoNo ratings yet
- Compilation of Platings in MicrobiologyDocument6 pagesCompilation of Platings in MicrobiologyVon HippoNo ratings yet
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoNo ratings yet
- Book: - RecordingDocument8 pagesBook: - RecordingVon HippoNo ratings yet
- NEPHRO - Renal Stones PDFDocument3 pagesNEPHRO - Renal Stones PDFVon HippoNo ratings yet
- 2013 Compiled para Exams and Shiftings PDFDocument27 pages2013 Compiled para Exams and Shiftings PDFVon HippoNo ratings yet
- Biochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Document14 pagesBiochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Von HippoNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- Army Public School Gopalpur: Class-Xii Science Subject - Biology Chapter-3 Human Reproduction NotesDocument5 pagesArmy Public School Gopalpur: Class-Xii Science Subject - Biology Chapter-3 Human Reproduction NotesAshok KumarNo ratings yet
- Health Effects of Androgen Abuse - A Review of The HAARLEM StudyDocument6 pagesHealth Effects of Androgen Abuse - A Review of The HAARLEM StudyEmile VeenstraNo ratings yet
- Issa Dna CoachDocument4 pagesIssa Dna Coachamirreza jmNo ratings yet
- Biochemistry One Liners by Medical LearnerDocument13 pagesBiochemistry One Liners by Medical LearnerSwapnil PawarNo ratings yet
- Who Wants To Be A Millionaire LabsDocument39 pagesWho Wants To Be A Millionaire LabsjustinNo ratings yet
- LTHT Paediatric Administration Guide Intravenous Sodium BicarbonateDocument2 pagesLTHT Paediatric Administration Guide Intravenous Sodium BicarbonateAjay KumarNo ratings yet
- AndrologyDocument93 pagesAndrologyhari krishnaa athotaNo ratings yet
- Ether Element Is Most Responsible Element For The Powerful ManifestationDocument2 pagesEther Element Is Most Responsible Element For The Powerful ManifestationMustafa AliNo ratings yet
- Fernanda Horrillo Ism ResreachDocument5 pagesFernanda Horrillo Ism Resreachapi-297188520No ratings yet
- Lab FQ 7 10 CompiledDocument61 pagesLab FQ 7 10 CompiledZylith NanaseNo ratings yet
- (20493614 - Endocrine Connections) How Glucagon-Like Peptide 1 Receptor Agonists WorkDocument13 pages(20493614 - Endocrine Connections) How Glucagon-Like Peptide 1 Receptor Agonists WorkEka RahmawatiNo ratings yet
- 5 TH Key PointDocument12 pages5 TH Key PointDr-Sanjay SinghaniaNo ratings yet
- Review of LiteratureDocument54 pagesReview of LiteratureShweta YaragattiNo ratings yet
- CH19 2 Biology WsDocument5 pagesCH19 2 Biology Ws陳詩淇No ratings yet
- 12) Drug Excretion and EliminationDocument14 pages12) Drug Excretion and EliminationManmeet Kohli IyerNo ratings yet
- Neonatal PharmacologyDocument61 pagesNeonatal PharmacologyAnaNo ratings yet
- 5.botswana CELEBRATIONS EnvironmentDocument51 pages5.botswana CELEBRATIONS EnvironmentYunus ElonNo ratings yet
- EndocrinologyDocument25 pagesEndocrinologyMaryam ShahzadiNo ratings yet
- Daun BinahongDocument9 pagesDaun Binahongkampus merdeka21No ratings yet
- Snake Venom Research PapersDocument8 pagesSnake Venom Research Papershxmchprhf100% (1)
- PNLE IV For Care of Clients With Physiologic and Psychosocial AlterationsDocument10 pagesPNLE IV For Care of Clients With Physiologic and Psychosocial AlterationsANGELINE PALATINONo ratings yet
- Bio Ninth Mcqs by Naveed ButtDocument22 pagesBio Ninth Mcqs by Naveed ButtNaveed Ahmed ButtNo ratings yet
- TPN CalculationDocument3 pagesTPN CalculationSARANYANo ratings yet
- Vet Systemic PathologyDocument66 pagesVet Systemic PathologySanjay KumarNo ratings yet
- Han, N. Et Al. 2016. Research Progress On Natural Benzophenanthridine Alkaloids and Their Pharmacological Functions A ReviweDocument9 pagesHan, N. Et Al. 2016. Research Progress On Natural Benzophenanthridine Alkaloids and Their Pharmacological Functions A ReviweshaniNo ratings yet
- Drug Study ONG CaseDocument3 pagesDrug Study ONG Casereized02No ratings yet
- Physical Education: Exercise For Fitness Quarter 1 Week 2 Module 2Document5 pagesPhysical Education: Exercise For Fitness Quarter 1 Week 2 Module 2Arlice Mae LleraNo ratings yet
- Aristo Ch.32 Textbook AnswersDocument9 pagesAristo Ch.32 Textbook AnswersyanaaNo ratings yet
- Nursing Shift PlannerDocument4 pagesNursing Shift PlannerSam NobleNo ratings yet