
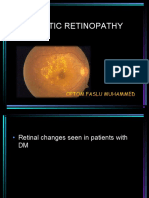
Diabetic Retinopathy
Diabetic Retinopathy
You might also like
- Diabetic RetinopathyDocument67 pagesDiabetic RetinopathyFirstyIlminovia0% (1)
- Diabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Document41 pagesDiabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Baba YagaNo ratings yet
- What Is Diabetic RetinopathyDocument6 pagesWhat Is Diabetic RetinopathyArvindan SubramaniamNo ratings yet
- Diabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeDocument63 pagesDiabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeNear DeathNo ratings yet
- Diabetic Retinopathy DR KatariaDocument65 pagesDiabetic Retinopathy DR KatariaDr Sandeep Kataria100% (1)
- Diabetic RetinopathyDocument55 pagesDiabetic RetinopathyMuhammad Bilal SaifulhaqNo ratings yet
- Diabetic Retinopathy: Dwi Lestari PohanDocument72 pagesDiabetic Retinopathy: Dwi Lestari PohanKelvin MandelaNo ratings yet
- Refrat Retinopati-DiabetikDocument20 pagesRefrat Retinopati-DiabetikDea NabilaNo ratings yet
- Lecture 11 Retina 1Document44 pagesLecture 11 Retina 1ؤيؤييسيNo ratings yet
- Diabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaDocument13 pagesDiabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaMohamad Faizul Abu HanifaNo ratings yet
- Diabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Document40 pagesDiabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Franky Frans SihombingNo ratings yet
- Diabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andDocument83 pagesDiabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andOlayemi Olorundare0% (1)
- Diabetic Eye Disease: Academic Unit of OphthalmologyDocument35 pagesDiabetic Eye Disease: Academic Unit of Ophthalmologyruwan555No ratings yet
- Diabetic RetinopathyDocument48 pagesDiabetic Retinopathykaran.A.K100% (1)
- Retinopati Diabetik - 1Document19 pagesRetinopati Diabetik - 1Yoyada SitorusNo ratings yet
- DR and Its ManagementDocument76 pagesDR and Its ManagementAravind KumarNo ratings yet
- Diabetes AND The Eye: Juliana Bentil Deborah AddoDocument50 pagesDiabetes AND The Eye: Juliana Bentil Deborah Addogideon A. owusuNo ratings yet
- Diabetic Retinopathy Presentations (Can Still Use The Older Classification)Document6 pagesDiabetic Retinopathy Presentations (Can Still Use The Older Classification)gdudex118811No ratings yet
- (Printing) Pass Medicine Notes - OphthalmologyDocument22 pages(Printing) Pass Medicine Notes - OphthalmologyJoanne HoNo ratings yet
- Diabetic Retinopathy For The Non-OphthalmologistDocument5 pagesDiabetic Retinopathy For The Non-OphthalmologistNATALIA SALAMANCA PEÑANo ratings yet
- Diabetic Retinopathy - Practice Essentials, Pathophysiology, EtiologyDocument11 pagesDiabetic Retinopathy - Practice Essentials, Pathophysiology, EtiologyIrma Kurniawati100% (1)
- Diabetic-Retinopathy GGGHGHDocument50 pagesDiabetic-Retinopathy GGGHGHjegannancyNo ratings yet
- AiraDocument17 pagesAiraPrincess Aira Bucag CarbonelNo ratings yet
- Retinal Diseases (Notes)Document76 pagesRetinal Diseases (Notes)khloud ywsefNo ratings yet
- Diabetic RetinopathyDocument18 pagesDiabetic Retinopathymohelshiekh100% (3)
- Diabetic RetinopathyDocument55 pagesDiabetic RetinopathyDrSaid Hussein GediNo ratings yet
- DIabetic REtinopathyDocument34 pagesDIabetic REtinopathyLuqman Khan YousafXaiNo ratings yet
- Treatment Diabetic RetinopathyDocument12 pagesTreatment Diabetic RetinopathyOdilia Rondang Mauli SimarmataNo ratings yet
- Diabetic RetinopathyDocument43 pagesDiabetic RetinopathyDr Sravya M VNo ratings yet
- Current Treatment OptionsDocument79 pagesCurrent Treatment OptionsANDREW OMAKANo ratings yet
- Diabetic Retinopathy: Clinical Findings and Management: Review ArticleDocument4 pagesDiabetic Retinopathy: Clinical Findings and Management: Review ArticlewadejackNo ratings yet
- Diabetic ThyDocument36 pagesDiabetic ThyItaNo ratings yet
- MEDS 1. Diabetic Retinopathy: Practice Essentials, Pathophysiology, EtiologyDocument14 pagesMEDS 1. Diabetic Retinopathy: Practice Essentials, Pathophysiology, EtiologyVivi DeviyanaNo ratings yet
- 02 DR-Classification PDFDocument5 pages02 DR-Classification PDFArghirescuNo ratings yet
- Ophthalmology - Passmedicine 2012 - 62013146Document18 pagesOphthalmology - Passmedicine 2012 - 62013146abuahmed&janaNo ratings yet
- Ocular Manifestation of Systemic DiseasesDocument58 pagesOcular Manifestation of Systemic DiseasesUmar AzlanNo ratings yet
- 5 Diabetic Macular EdemaDocument15 pages5 Diabetic Macular EdemaJohn Vargas AgudeloNo ratings yet
- Note DRDocument2 pagesNote DRZuhair Al-JaffalNo ratings yet
- ICOGuidelins For DiabeticEye CareDocument28 pagesICOGuidelins For DiabeticEye CareIrfan SadiqNo ratings yet
- Diabetic RetinopatiDocument44 pagesDiabetic RetinopatiLaurensia MassariNo ratings yet
- Diabetic RetinopathyDocument78 pagesDiabetic RetinopathyAnumeha Jindal100% (1)
- A Deep Learning Approach For The Detection of Diabetic RetinopathyDocument55 pagesA Deep Learning Approach For The Detection of Diabetic RetinopathyjegannancyNo ratings yet
- Pathology - Chapter 29 (Partial)Document3 pagesPathology - Chapter 29 (Partial)Cory GrayNo ratings yet
- Retinal Vascular DisordersDocument52 pagesRetinal Vascular Disorderssushma shresthaNo ratings yet
- Vitreo Retinal DisordersDocument47 pagesVitreo Retinal DisordersTabreez KhanNo ratings yet
- Vitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkiDocument45 pagesVitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkitusuksedotanNo ratings yet
- Diabetic Retinopathy: Dr. A.M.Ichsan, PHD, SPMDocument41 pagesDiabetic Retinopathy: Dr. A.M.Ichsan, PHD, SPMAyu Diah RestiKusuma PutriNo ratings yet
- Diabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerDocument32 pagesDiabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerCarlos HerreraNo ratings yet
- Retinal Vascular Diseas E: Christine Anne D. EspejaDocument25 pagesRetinal Vascular Diseas E: Christine Anne D. EspejaPaolo QuezonNo ratings yet
- Diabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDDocument55 pagesDiabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDadi amaliNo ratings yet
- Nonproliferative Diabetic Retinopathy and Diabetic Macular EdemaDocument37 pagesNonproliferative Diabetic Retinopathy and Diabetic Macular EdemaBhumika RathNo ratings yet
- Diabetic Retinopathy New-1Document99 pagesDiabetic Retinopathy New-1Sana AzimNo ratings yet
- Diabetic Retinopathy - Classification and Clinical Features - UpToDateDocument38 pagesDiabetic Retinopathy - Classification and Clinical Features - UpToDateRachmatBimanjayaNo ratings yet
- Retinopatia Diabetica 2018Document34 pagesRetinopatia Diabetica 2018Fanny ParraNo ratings yet
- Introduction To FundusDocument55 pagesIntroduction To FundusGingerNo ratings yet
- Diabetic RetinopathyDocument115 pagesDiabetic RetinopathyMihaela FrumusacheNo ratings yet
- Diabetic RetinopathyDocument40 pagesDiabetic RetinopathyNaman MishraNo ratings yet
- Dr. Indra DIAGNOSTIC FEATURES IN DIABETIC RETINOPATHYDocument11 pagesDr. Indra DIAGNOSTIC FEATURES IN DIABETIC RETINOPATHYdeprot87No ratings yet
- Diabetic Retinopathy: Introduction to Novel Treatment StrategiesFrom EverandDiabetic Retinopathy: Introduction to Novel Treatment StrategiesNo ratings yet
- Age-Related Macular Degeneration: Current Treatment ConceptsFrom EverandAge-Related Macular Degeneration: Current Treatment ConceptsW.E. AlbertiNo ratings yet
- Contak: Artist Management ReimaginedDocument12 pagesContak: Artist Management ReimaginedGetLyricsNo ratings yet
- Diabetic RetinopathyDocument44 pagesDiabetic RetinopathyGetLyricsNo ratings yet
- Pathophysiology of Diabetic RetinopathyDocument40 pagesPathophysiology of Diabetic RetinopathyGetLyricsNo ratings yet
- Trochlear Nerve: Presentation byDocument13 pagesTrochlear Nerve: Presentation byGetLyricsNo ratings yet
- Network Intrusion Detection System Using SnortDocument22 pagesNetwork Intrusion Detection System Using SnortGetLyricsNo ratings yet
- Oculomotor Nerve: DR / Hytham NafadyDocument52 pagesOculomotor Nerve: DR / Hytham NafadyGetLyricsNo ratings yet
- Multimodalremotemovementsensing 191118200104Document63 pagesMultimodalremotemovementsensing 191118200104GetLyricsNo ratings yet
- Techniquesofretinoscopy 180210035327Document14 pagesTechniquesofretinoscopy 180210035327GetLyricsNo ratings yet
- Fundusmetamaterials 190827040758Document43 pagesFundusmetamaterials 190827040758GetLyricsNo ratings yet
- Multiphotonsegmentation2bvasculature 190808162232Document218 pagesMultiphotonsegmentation2bvasculature 190808162232GetLyricsNo ratings yet
- Smearlayerinendodontics 170106182934Document80 pagesSmearlayerinendodontics 170106182934GetLyricsNo ratings yet
- Corneal OpacityDocument65 pagesCorneal OpacityAnnasaheb PatilNo ratings yet
- Fitzpatrick Skin Type FormDocument1 pageFitzpatrick Skin Type FormminoucheNo ratings yet
- MSDS Eye PillowDocument2 pagesMSDS Eye Pillowrahayu wirayantiNo ratings yet
- 3M™ Centurion™ Safety Splash Goggle 454AF, 40305-00000-10 Clear Anti-Fog LensDocument2 pages3M™ Centurion™ Safety Splash Goggle 454AF, 40305-00000-10 Clear Anti-Fog LensJerry C KurianNo ratings yet
- Brochure Iolmaster 700 ModfDocument11 pagesBrochure Iolmaster 700 ModfTT XNo ratings yet
- 5 6337055981314245059Document498 pages5 6337055981314245059A.c. RaghuNo ratings yet
- BS 02738-1-1998Document15 pagesBS 02738-1-1998miguel.sampaio.estevesNo ratings yet
- Protective Effects of Blue Light-Blocking Shades On Phototoxicity in Human Ocular Surface CellsDocument6 pagesProtective Effects of Blue Light-Blocking Shades On Phototoxicity in Human Ocular Surface CellsHans Steven KurniawanNo ratings yet
- Research Paper About Contact LensesDocument6 pagesResearch Paper About Contact Lensesrykkssbnd100% (1)
- SOCT Copernicus: OPTOPOL Technology S.ADocument4 pagesSOCT Copernicus: OPTOPOL Technology S.AakhterNo ratings yet
- Reader 39 S Digest UK - 05 2021Document146 pagesReader 39 S Digest UK - 05 2021Mon LayNo ratings yet
- Forceps-Induced Birth Injury To The Cornea: Ruba Alobaidy, Sathish SrinivasanDocument2 pagesForceps-Induced Birth Injury To The Cornea: Ruba Alobaidy, Sathish SrinivasanseptianarifwandiniNo ratings yet
- Primary Baerveldt Versus Trabeculectomy Study After 5 Years of Follow-UpDocument8 pagesPrimary Baerveldt Versus Trabeculectomy Study After 5 Years of Follow-UptiaraleshaNo ratings yet
- Nidek AR600 PDFDocument70 pagesNidek AR600 PDFMilton CâmeraNo ratings yet
- Revision Date: 00: Material Safety Data SheetDocument7 pagesRevision Date: 00: Material Safety Data SheetObbyNo ratings yet
- Addis Ababa UniversityDocument44 pagesAddis Ababa UniversityNathan Berhanu100% (1)
- Blue Light Blindness StudyDocument9 pagesBlue Light Blindness StudyJackson D.S.No ratings yet
- Safety Data Sheet: 1. IdentificationDocument8 pagesSafety Data Sheet: 1. IdentificationSergio FernandesNo ratings yet
- Wednesday 15 January 2020: Human BiologyDocument24 pagesWednesday 15 January 2020: Human Biologyaqib ameerNo ratings yet
- ICD 10-Mata AdmisiDocument2 pagesICD 10-Mata AdmisiRedho WinandaNo ratings yet
- Physical Examination:-: Vital SignsDocument4 pagesPhysical Examination:-: Vital SignspriyaNo ratings yet
- DANAR Material Safety DatasheetDocument4 pagesDANAR Material Safety DatasheetRiadiAdiNo ratings yet
- Vital Signs, GCS, PerrlaDocument25 pagesVital Signs, GCS, PerrlaAshley Nicole Velasco TaperlaNo ratings yet
- Aes 05 37Document13 pagesAes 05 37Marco Antonio MiraveteNo ratings yet
- School For Perfect Eyesight, PondicherryDocument8 pagesSchool For Perfect Eyesight, PondicherryKemkengNo ratings yet
- Blepharitis An Inflammatory Condition of The EyelidsDocument4 pagesBlepharitis An Inflammatory Condition of The EyelidsTasyaNo ratings yet
- Health Assessment FinalsDocument25 pagesHealth Assessment FinalserythromycinNo ratings yet
- MSDS Bentagi Legenda WBSS 5071 ClearDocument4 pagesMSDS Bentagi Legenda WBSS 5071 ClearFindora InternusaNo ratings yet
- ButyldiglycolDocument7 pagesButyldiglycolJaleel AhmedNo ratings yet
- 76-80 SOAL FixDocument2 pages76-80 SOAL FixBery Decky SaputraNo ratings yet


































































































Download as pdf or txt
You might also like
- Diabetic RetinopathyDocument67 pagesDiabetic RetinopathyFirstyIlminovia0% (1)
- Diabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Document41 pagesDiabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Baba YagaNo ratings yet
- What Is Diabetic RetinopathyDocument6 pagesWhat Is Diabetic RetinopathyArvindan SubramaniamNo ratings yet
- Diabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeDocument63 pagesDiabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeNear DeathNo ratings yet
- Diabetic Retinopathy DR KatariaDocument65 pagesDiabetic Retinopathy DR KatariaDr Sandeep Kataria100% (1)
- Diabetic RetinopathyDocument55 pagesDiabetic RetinopathyMuhammad Bilal SaifulhaqNo ratings yet
- Diabetic Retinopathy: Dwi Lestari PohanDocument72 pagesDiabetic Retinopathy: Dwi Lestari PohanKelvin MandelaNo ratings yet
- Refrat Retinopati-DiabetikDocument20 pagesRefrat Retinopati-DiabetikDea NabilaNo ratings yet
- Lecture 11 Retina 1Document44 pagesLecture 11 Retina 1ؤيؤييسيNo ratings yet
- Diabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaDocument13 pagesDiabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaMohamad Faizul Abu HanifaNo ratings yet
- Diabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Document40 pagesDiabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Franky Frans SihombingNo ratings yet
- Diabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andDocument83 pagesDiabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andOlayemi Olorundare0% (1)
- Diabetic Eye Disease: Academic Unit of OphthalmologyDocument35 pagesDiabetic Eye Disease: Academic Unit of Ophthalmologyruwan555No ratings yet
- Diabetic RetinopathyDocument48 pagesDiabetic Retinopathykaran.A.K100% (1)
- Retinopati Diabetik - 1Document19 pagesRetinopati Diabetik - 1Yoyada SitorusNo ratings yet
- DR and Its ManagementDocument76 pagesDR and Its ManagementAravind KumarNo ratings yet
- Diabetes AND The Eye: Juliana Bentil Deborah AddoDocument50 pagesDiabetes AND The Eye: Juliana Bentil Deborah Addogideon A. owusuNo ratings yet
- Diabetic Retinopathy Presentations (Can Still Use The Older Classification)Document6 pagesDiabetic Retinopathy Presentations (Can Still Use The Older Classification)gdudex118811No ratings yet
- (Printing) Pass Medicine Notes - OphthalmologyDocument22 pages(Printing) Pass Medicine Notes - OphthalmologyJoanne HoNo ratings yet
- Diabetic Retinopathy For The Non-OphthalmologistDocument5 pagesDiabetic Retinopathy For The Non-OphthalmologistNATALIA SALAMANCA PEÑANo ratings yet
- Diabetic Retinopathy - Practice Essentials, Pathophysiology, EtiologyDocument11 pagesDiabetic Retinopathy - Practice Essentials, Pathophysiology, EtiologyIrma Kurniawati100% (1)
- Diabetic-Retinopathy GGGHGHDocument50 pagesDiabetic-Retinopathy GGGHGHjegannancyNo ratings yet
- AiraDocument17 pagesAiraPrincess Aira Bucag CarbonelNo ratings yet
- Retinal Diseases (Notes)Document76 pagesRetinal Diseases (Notes)khloud ywsefNo ratings yet
- Diabetic RetinopathyDocument18 pagesDiabetic Retinopathymohelshiekh100% (3)
- Diabetic RetinopathyDocument55 pagesDiabetic RetinopathyDrSaid Hussein GediNo ratings yet
- DIabetic REtinopathyDocument34 pagesDIabetic REtinopathyLuqman Khan YousafXaiNo ratings yet
- Treatment Diabetic RetinopathyDocument12 pagesTreatment Diabetic RetinopathyOdilia Rondang Mauli SimarmataNo ratings yet
- Diabetic RetinopathyDocument43 pagesDiabetic RetinopathyDr Sravya M VNo ratings yet
- Current Treatment OptionsDocument79 pagesCurrent Treatment OptionsANDREW OMAKANo ratings yet
- Diabetic Retinopathy: Clinical Findings and Management: Review ArticleDocument4 pagesDiabetic Retinopathy: Clinical Findings and Management: Review ArticlewadejackNo ratings yet
- Diabetic ThyDocument36 pagesDiabetic ThyItaNo ratings yet
- MEDS 1. Diabetic Retinopathy: Practice Essentials, Pathophysiology, EtiologyDocument14 pagesMEDS 1. Diabetic Retinopathy: Practice Essentials, Pathophysiology, EtiologyVivi DeviyanaNo ratings yet
- 02 DR-Classification PDFDocument5 pages02 DR-Classification PDFArghirescuNo ratings yet
- Ophthalmology - Passmedicine 2012 - 62013146Document18 pagesOphthalmology - Passmedicine 2012 - 62013146abuahmed&janaNo ratings yet
- Ocular Manifestation of Systemic DiseasesDocument58 pagesOcular Manifestation of Systemic DiseasesUmar AzlanNo ratings yet
- 5 Diabetic Macular EdemaDocument15 pages5 Diabetic Macular EdemaJohn Vargas AgudeloNo ratings yet
- Note DRDocument2 pagesNote DRZuhair Al-JaffalNo ratings yet
- ICOGuidelins For DiabeticEye CareDocument28 pagesICOGuidelins For DiabeticEye CareIrfan SadiqNo ratings yet
- Diabetic RetinopatiDocument44 pagesDiabetic RetinopatiLaurensia MassariNo ratings yet
- Diabetic RetinopathyDocument78 pagesDiabetic RetinopathyAnumeha Jindal100% (1)
- A Deep Learning Approach For The Detection of Diabetic RetinopathyDocument55 pagesA Deep Learning Approach For The Detection of Diabetic RetinopathyjegannancyNo ratings yet
- Pathology - Chapter 29 (Partial)Document3 pagesPathology - Chapter 29 (Partial)Cory GrayNo ratings yet
- Retinal Vascular DisordersDocument52 pagesRetinal Vascular Disorderssushma shresthaNo ratings yet
- Vitreo Retinal DisordersDocument47 pagesVitreo Retinal DisordersTabreez KhanNo ratings yet
- Vitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkiDocument45 pagesVitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkitusuksedotanNo ratings yet
- Diabetic Retinopathy: Dr. A.M.Ichsan, PHD, SPMDocument41 pagesDiabetic Retinopathy: Dr. A.M.Ichsan, PHD, SPMAyu Diah RestiKusuma PutriNo ratings yet
- Diabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerDocument32 pagesDiabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerCarlos HerreraNo ratings yet
- Retinal Vascular Diseas E: Christine Anne D. EspejaDocument25 pagesRetinal Vascular Diseas E: Christine Anne D. EspejaPaolo QuezonNo ratings yet
- Diabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDDocument55 pagesDiabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDadi amaliNo ratings yet
- Nonproliferative Diabetic Retinopathy and Diabetic Macular EdemaDocument37 pagesNonproliferative Diabetic Retinopathy and Diabetic Macular EdemaBhumika RathNo ratings yet
- Diabetic Retinopathy New-1Document99 pagesDiabetic Retinopathy New-1Sana AzimNo ratings yet
- Diabetic Retinopathy - Classification and Clinical Features - UpToDateDocument38 pagesDiabetic Retinopathy - Classification and Clinical Features - UpToDateRachmatBimanjayaNo ratings yet
- Retinopatia Diabetica 2018Document34 pagesRetinopatia Diabetica 2018Fanny ParraNo ratings yet
- Introduction To FundusDocument55 pagesIntroduction To FundusGingerNo ratings yet
- Diabetic RetinopathyDocument115 pagesDiabetic RetinopathyMihaela FrumusacheNo ratings yet
- Diabetic RetinopathyDocument40 pagesDiabetic RetinopathyNaman MishraNo ratings yet
- Dr. Indra DIAGNOSTIC FEATURES IN DIABETIC RETINOPATHYDocument11 pagesDr. Indra DIAGNOSTIC FEATURES IN DIABETIC RETINOPATHYdeprot87No ratings yet
- Diabetic Retinopathy: Introduction to Novel Treatment StrategiesFrom EverandDiabetic Retinopathy: Introduction to Novel Treatment StrategiesNo ratings yet
- Age-Related Macular Degeneration: Current Treatment ConceptsFrom EverandAge-Related Macular Degeneration: Current Treatment ConceptsW.E. AlbertiNo ratings yet
- Contak: Artist Management ReimaginedDocument12 pagesContak: Artist Management ReimaginedGetLyricsNo ratings yet
- Diabetic RetinopathyDocument44 pagesDiabetic RetinopathyGetLyricsNo ratings yet
- Pathophysiology of Diabetic RetinopathyDocument40 pagesPathophysiology of Diabetic RetinopathyGetLyricsNo ratings yet
- Trochlear Nerve: Presentation byDocument13 pagesTrochlear Nerve: Presentation byGetLyricsNo ratings yet
- Network Intrusion Detection System Using SnortDocument22 pagesNetwork Intrusion Detection System Using SnortGetLyricsNo ratings yet
- Oculomotor Nerve: DR / Hytham NafadyDocument52 pagesOculomotor Nerve: DR / Hytham NafadyGetLyricsNo ratings yet
- Multimodalremotemovementsensing 191118200104Document63 pagesMultimodalremotemovementsensing 191118200104GetLyricsNo ratings yet
- Techniquesofretinoscopy 180210035327Document14 pagesTechniquesofretinoscopy 180210035327GetLyricsNo ratings yet
- Fundusmetamaterials 190827040758Document43 pagesFundusmetamaterials 190827040758GetLyricsNo ratings yet
- Multiphotonsegmentation2bvasculature 190808162232Document218 pagesMultiphotonsegmentation2bvasculature 190808162232GetLyricsNo ratings yet
- Smearlayerinendodontics 170106182934Document80 pagesSmearlayerinendodontics 170106182934GetLyricsNo ratings yet
- Corneal OpacityDocument65 pagesCorneal OpacityAnnasaheb PatilNo ratings yet
- Fitzpatrick Skin Type FormDocument1 pageFitzpatrick Skin Type FormminoucheNo ratings yet
- MSDS Eye PillowDocument2 pagesMSDS Eye Pillowrahayu wirayantiNo ratings yet
- 3M™ Centurion™ Safety Splash Goggle 454AF, 40305-00000-10 Clear Anti-Fog LensDocument2 pages3M™ Centurion™ Safety Splash Goggle 454AF, 40305-00000-10 Clear Anti-Fog LensJerry C KurianNo ratings yet
- Brochure Iolmaster 700 ModfDocument11 pagesBrochure Iolmaster 700 ModfTT XNo ratings yet
- 5 6337055981314245059Document498 pages5 6337055981314245059A.c. RaghuNo ratings yet
- BS 02738-1-1998Document15 pagesBS 02738-1-1998miguel.sampaio.estevesNo ratings yet
- Protective Effects of Blue Light-Blocking Shades On Phototoxicity in Human Ocular Surface CellsDocument6 pagesProtective Effects of Blue Light-Blocking Shades On Phototoxicity in Human Ocular Surface CellsHans Steven KurniawanNo ratings yet
- Research Paper About Contact LensesDocument6 pagesResearch Paper About Contact Lensesrykkssbnd100% (1)
- SOCT Copernicus: OPTOPOL Technology S.ADocument4 pagesSOCT Copernicus: OPTOPOL Technology S.AakhterNo ratings yet
- Reader 39 S Digest UK - 05 2021Document146 pagesReader 39 S Digest UK - 05 2021Mon LayNo ratings yet
- Forceps-Induced Birth Injury To The Cornea: Ruba Alobaidy, Sathish SrinivasanDocument2 pagesForceps-Induced Birth Injury To The Cornea: Ruba Alobaidy, Sathish SrinivasanseptianarifwandiniNo ratings yet
- Primary Baerveldt Versus Trabeculectomy Study After 5 Years of Follow-UpDocument8 pagesPrimary Baerveldt Versus Trabeculectomy Study After 5 Years of Follow-UptiaraleshaNo ratings yet
- Nidek AR600 PDFDocument70 pagesNidek AR600 PDFMilton CâmeraNo ratings yet
- Revision Date: 00: Material Safety Data SheetDocument7 pagesRevision Date: 00: Material Safety Data SheetObbyNo ratings yet
- Addis Ababa UniversityDocument44 pagesAddis Ababa UniversityNathan Berhanu100% (1)
- Blue Light Blindness StudyDocument9 pagesBlue Light Blindness StudyJackson D.S.No ratings yet
- Safety Data Sheet: 1. IdentificationDocument8 pagesSafety Data Sheet: 1. IdentificationSergio FernandesNo ratings yet
- Wednesday 15 January 2020: Human BiologyDocument24 pagesWednesday 15 January 2020: Human Biologyaqib ameerNo ratings yet
- ICD 10-Mata AdmisiDocument2 pagesICD 10-Mata AdmisiRedho WinandaNo ratings yet
- Physical Examination:-: Vital SignsDocument4 pagesPhysical Examination:-: Vital SignspriyaNo ratings yet
- DANAR Material Safety DatasheetDocument4 pagesDANAR Material Safety DatasheetRiadiAdiNo ratings yet
- Vital Signs, GCS, PerrlaDocument25 pagesVital Signs, GCS, PerrlaAshley Nicole Velasco TaperlaNo ratings yet
- Aes 05 37Document13 pagesAes 05 37Marco Antonio MiraveteNo ratings yet
- School For Perfect Eyesight, PondicherryDocument8 pagesSchool For Perfect Eyesight, PondicherryKemkengNo ratings yet
- Blepharitis An Inflammatory Condition of The EyelidsDocument4 pagesBlepharitis An Inflammatory Condition of The EyelidsTasyaNo ratings yet
- Health Assessment FinalsDocument25 pagesHealth Assessment FinalserythromycinNo ratings yet
- MSDS Bentagi Legenda WBSS 5071 ClearDocument4 pagesMSDS Bentagi Legenda WBSS 5071 ClearFindora InternusaNo ratings yet
- ButyldiglycolDocument7 pagesButyldiglycolJaleel AhmedNo ratings yet
- 76-80 SOAL FixDocument2 pages76-80 SOAL FixBery Decky SaputraNo ratings yet