
USL League One Return-to-Play Protocols
USL League One Return-to-Play Protocols
You might also like
- USL Step Up Women's Soccer StrategyDocument20 pagesUSL Step Up Women's Soccer StrategyUSL0% (1)
- 2022 USL Championship Record BookDocument57 pages2022 USL Championship Record BookUSL50% (2)
- 2021 SYL Player Experience PacketDocument8 pages2021 SYL Player Experience PacketUSL0% (2)
- Coaching Tiki Taka ContentsDocument5 pagesCoaching Tiki Taka ContentsJonty Toradmal0% (1)
- Textbook of Oral Medicine (Anil Govindrao Ghom, Savita Anil Ghom (Lodam) )Document1,141 pagesTextbook of Oral Medicine (Anil Govindrao Ghom, Savita Anil Ghom (Lodam) )Hritika Mehta100% (5)
- 2021 Championship Media GuideDocument73 pages2021 Championship Media GuideUSL100% (1)
- General and Oral Pathology For Dental Hygiene PracticeDocument361 pagesGeneral and Oral Pathology For Dental Hygiene Practicepsychposters100% (1)
- 2022 USL League One Media GuideDocument33 pages2022 USL League One Media GuideUSL0% (1)
- 2021 Championship Record BookDocument58 pages2021 Championship Record BookUSL100% (1)
- 2021 Return To Play Protocols - USL ChampionshipDocument62 pages2021 Return To Play Protocols - USL ChampionshipUSLNo ratings yet
- 2021 Return To Play Protocols - USL ChampionshipDocument62 pages2021 Return To Play Protocols - USL ChampionshipUSLNo ratings yet
- USL League One 2020 Record BookDocument35 pagesUSL League One 2020 Record BookUSL0% (1)
- Soccer Team Stats Tracker Pro V2.42Document1,493 pagesSoccer Team Stats Tracker Pro V2.42Gomv ConsNo ratings yet
- 2021 USL Academy League Operations ManualDocument57 pages2021 USL Academy League Operations ManualUSLNo ratings yet
- How Verheijen's Football Periodisation Inspired The Creation of SoccerPulse 1Document1 pageHow Verheijen's Football Periodisation Inspired The Creation of SoccerPulse 1Victor PetcuNo ratings yet
- Digital Video Games Approach A Designer For Invasion Games: @amyprice - 10Document6 pagesDigital Video Games Approach A Designer For Invasion Games: @amyprice - 10api-368878817No ratings yet
- USL League One 2021 Return To Play ProtocolsDocument63 pagesUSL League One 2021 Return To Play ProtocolsUSLNo ratings yet
- 2020 USL League One Media GuideDocument35 pages2020 USL League One Media GuideUSLNo ratings yet
- 2020 USL Championship Media GuideDocument41 pages2020 USL Championship Media GuideUSL33% (3)
- Alfredo Bonadeo - Montaigne and DeathDocument12 pagesAlfredo Bonadeo - Montaigne and DeathMark CohenNo ratings yet
- Lecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFDocument37 pagesLecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFstefany huangNo ratings yet
- Energy Cost and Metabolic Power in Elite Soccer A New Match Analysis ApproachDocument9 pagesEnergy Cost and Metabolic Power in Elite Soccer A New Match Analysis Approachjeduardo48No ratings yet
- Structuring A Program in Elite Professional Soccer: Strength and Conditioning Journal December 2017Document12 pagesStructuring A Program in Elite Professional Soccer: Strength and Conditioning Journal December 2017Jozef Oki SkumpijaNo ratings yet
- Tactical Periodisation in Football 1680883188Document2 pagesTactical Periodisation in Football 1680883188marcelloNo ratings yet
- A Methodology For The Analysis of Soccer Matches Based On PageRank Centrality PDFDocument16 pagesA Methodology For The Analysis of Soccer Matches Based On PageRank Centrality PDFOmar Enrique Garcia CaicedoNo ratings yet
- 12-Month Periodized Football Training ProgramDocument5 pages12-Month Periodized Football Training ProgramRon RNo ratings yet
- NOW IS THE TIME V 1 Compressed 1Document11 pagesNOW IS THE TIME V 1 Compressed 1harunabiaty849163No ratings yet
- Futsal Management Report PDFDocument37 pagesFutsal Management Report PDFJUNU CHAULAGAIN100% (1)
- The Business Model of European Football Club CompeDocument8 pagesThe Business Model of European Football Club CompeANSHUL MEHROTTRANo ratings yet
- gc101 PDFDocument45 pagesgc101 PDFFitim GabrricaNo ratings yet
- Implementing A Sustainable Club Membership Program at Goan Football PVT LTD (FC GoaDocument58 pagesImplementing A Sustainable Club Membership Program at Goan Football PVT LTD (FC GoaAli SaifyNo ratings yet
- Sport Plan User GuideDocument14 pagesSport Plan User Guidehamo pipaNo ratings yet
- Striker Manager Training (Modified)Document6 pagesStriker Manager Training (Modified)010b9No ratings yet
- Football Training and PracticesDocument8 pagesFootball Training and PracticesMichael Khunonyane100% (1)
- Football Movement and Application Assignment - Isaac BenouzekriDocument3 pagesFootball Movement and Application Assignment - Isaac BenouzekriIsaac BNo ratings yet
- 1115 Camp GuideDocument43 pages1115 Camp GuideEduardo FerranteNo ratings yet
- Wednesday Training Day Practices:: Speed EnduranceDocument7 pagesWednesday Training Day Practices:: Speed EnduranceMichael KhunonyaneNo ratings yet
- D License Log BookDocument16 pagesD License Log BookAayush SaxenaNo ratings yet
- LTAD Lead MagnetDocument38 pagesLTAD Lead Magnetsiphadube365No ratings yet
- Effects of A Contrast Training Program Without External Load On Vertical Jump, Kicking Speed, Sprint, and Agility of Young Soccer Players PDFDocument9 pagesEffects of A Contrast Training Program Without External Load On Vertical Jump, Kicking Speed, Sprint, and Agility of Young Soccer Players PDFNiña AlviaNo ratings yet
- Breakthrough BalanceDocument40 pagesBreakthrough BalanceBosko GuberinicNo ratings yet
- The FA's Longterm DevelopmentDocument6 pagesThe FA's Longterm DevelopmentBudi Handoko100% (1)
- Italian Serie A' Academy Training: An Inside Look at Two Italian Professional AcademiesDocument78 pagesItalian Serie A' Academy Training: An Inside Look at Two Italian Professional AcademiesJosé VelosaNo ratings yet
- Chelsea Football ClubDocument14 pagesChelsea Football ClubAnirudh MariaNo ratings yet
- Report 128083Document53 pagesReport 128083CueroNo ratings yet
- 1995 Joe Luxbacher - Soccer Practice Games-Human KineticsDocument164 pages1995 Joe Luxbacher - Soccer Practice Games-Human KineticsagusmulyaNo ratings yet
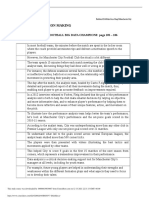
- Chapter 2: Decision Making: Case Application 2: Manchester City: Football Big Data Champions: Page 105 - 106Document6 pagesChapter 2: Decision Making: Case Application 2: Manchester City: Football Big Data Champions: Page 105 - 106Gautham100% (1)
- High-Intensity Interval Training: Loughborough University Institutional RepositoryDocument46 pagesHigh-Intensity Interval Training: Loughborough University Institutional RepositoryGytis GarbačiauskasNo ratings yet
- Lucozade Sport Pre Season Training Week 21Document1 pageLucozade Sport Pre Season Training Week 21Wan Ariff SallehNo ratings yet
- Exploratory Analysis FootballDocument6 pagesExploratory Analysis FootballMattNo ratings yet
- Journal 22Document32 pagesJournal 22nkosidlaminiNo ratings yet
- Soccer CoachDocument5 pagesSoccer Coachapi-286079185No ratings yet
- UEFA - A Licence Full DocumentDocument96 pagesUEFA - A Licence Full DocumentQUI SUIS-JE ?No ratings yet
- 08-12 SCI 09.34 Helena CostaDocument5 pages08-12 SCI 09.34 Helena CostaRicardo LuizNo ratings yet
- Soccer Psychology AssessmentDocument2 pagesSoccer Psychology AssessmentAurora NuñoNo ratings yet
- Injury Prevention Training in Football: Time To Consider Training Under Fatigue?Document4 pagesInjury Prevention Training in Football: Time To Consider Training Under Fatigue?aminNo ratings yet
- Special Olympics World Games Handball Technical ManualDocument32 pagesSpecial Olympics World Games Handball Technical ManualJenni SimcoeNo ratings yet
- Strength and Conditioining GAADocument8 pagesStrength and Conditioining GAADenis LordanNo ratings yet
- Best Foot Forward: Optimum PerformanceDocument6 pagesBest Foot Forward: Optimum PerformanceVicente Ignacio Ormazábal MedinaNo ratings yet
- Games Analysis Outdoor Team Sports by Using GPS SystemDocument35 pagesGames Analysis Outdoor Team Sports by Using GPS SystemAmin CherbitiNo ratings yet
- Receng Trends in High Intensity Aerobic - Training PDFDocument6 pagesReceng Trends in High Intensity Aerobic - Training PDFPablo100% (1)
- All About Masia 360Document7 pagesAll About Masia 360Pavol Gregora100% (1)
- Alvarado Lopez, Enoch - InterludeDocument14 pagesAlvarado Lopez, Enoch - InterludeDuvan RodeloNo ratings yet
- Youth Leagues Youth Development Review BookletDocument19 pagesYouth Leagues Youth Development Review BookletMarek Dragosz Keepers FoundationNo ratings yet
- A Guide To Developing Physical Qualities in Young AthletesDocument168 pagesA Guide To Developing Physical Qualities in Young AthletesjoaoaesfigueiredoNo ratings yet
- Preseden - Portofolio Soccer Training Centre PDFDocument147 pagesPreseden - Portofolio Soccer Training Centre PDFimam sodikunNo ratings yet
- Scottish Fa Uefa C Licence BrochureDocument5 pagesScottish Fa Uefa C Licence Brochuremohammad kamarNo ratings yet
- Manchester City FC, Annual Report 2014/15Document64 pagesManchester City FC, Annual Report 2014/15Tifoso Bilanciato100% (1)
- UEFA Equipment RegulationsDocument72 pagesUEFA Equipment RegulationsBasto WongNo ratings yet
- Fitness Testing in Football - Jens Bangsbo Magni MohrDocument144 pagesFitness Testing in Football - Jens Bangsbo Magni MohrSuman DevNo ratings yet
- Coaches Circle Issue 6 - May 2021Document24 pagesCoaches Circle Issue 6 - May 2021เซบาสเตียน ไลฟ์ลีดเดอร์No ratings yet
- Individual Defensive Skills Team DefenseDocument15 pagesIndividual Defensive Skills Team DefenseEl Cuervo Waterpolo100% (2)
- The high line: Debunking the myths surrounding the high press system used in footballFrom EverandThe high line: Debunking the myths surrounding the high press system used in footballNo ratings yet
- The Futsal Way: Maximising the Performance of Elite Football Teams Through Futsal MethodsFrom EverandThe Futsal Way: Maximising the Performance of Elite Football Teams Through Futsal MethodsNo ratings yet
- Book 4: Soccer Revelations Coaching Knowledge: Academy of Coaching Soccer Skills and Fitness DrillsFrom EverandBook 4: Soccer Revelations Coaching Knowledge: Academy of Coaching Soccer Skills and Fitness DrillsNo ratings yet
- Training Sessions For Soccer Coaches Volumes 1-2-3: Training Sessions For Soccer CoachesFrom EverandTraining Sessions For Soccer Coaches Volumes 1-2-3: Training Sessions For Soccer CoachesNo ratings yet
- Training Sessions For Soccer Coaches Volume 2: Training Sessions For Soccer Coaches, #2From EverandTraining Sessions For Soccer Coaches Volume 2: Training Sessions For Soccer Coaches, #2No ratings yet
- 2022 Mid Year MeetingDocument1 page2022 Mid Year MeetingUSLNo ratings yet
- 2022 Mid Year MeetingDocument1 page2022 Mid Year MeetingUSLNo ratings yet
- 2022 USL Academy Cup Operations ManualDocument30 pages2022 USL Academy Cup Operations ManualUSLNo ratings yet
- 2022 Mid-Year Meeting - ScheduleDocument1 page2022 Mid-Year Meeting - ScheduleUSLNo ratings yet
- 2018 SYL Player PacketDocument7 pages2018 SYL Player PacketUSLNo ratings yet
- 2021 USL League One Media GuideDocument35 pages2021 USL League One Media GuideUSLNo ratings yet
- USL Championship Return To Play ProtocolsDocument53 pagesUSL Championship Return To Play ProtocolsUSLNo ratings yet
- 2019 USL Championship Media GuideDocument42 pages2019 USL Championship Media GuideUSL100% (1)
- 2018 SYL Player PacketDocument7 pages2018 SYL Player PacketUSLNo ratings yet
- USL 2018 Media GuideDocument45 pagesUSL 2018 Media GuideUSL100% (2)
- USL 2018 Media GuideDocument45 pagesUSL 2018 Media GuideUSL100% (2)
- Muhamad Lutfi ParatuberculosisJournalDocument17 pagesMuhamad Lutfi ParatuberculosisJournalLutfi AlkaNo ratings yet
- The Classification of SicknessDocument361 pagesThe Classification of SicknessizamNo ratings yet
- Sicknessandfitnesscertificates PDFDocument6 pagesSicknessandfitnesscertificates PDFniraj_sdNo ratings yet
- Transcranial Magnetic Stimulation - Jasper AzzarelloDocument2 pagesTranscranial Magnetic Stimulation - Jasper AzzarelloJasper AZZARELLONo ratings yet
- Ethiopia: Feed The Future Innovation Lab For Livestock SystemsDocument11 pagesEthiopia: Feed The Future Innovation Lab For Livestock SystemsMitikuNo ratings yet
- FNCP Alfonso CaviteDocument8 pagesFNCP Alfonso Caviteroxjanmer_13No ratings yet
- Approach To Foot UlcerDocument29 pagesApproach To Foot Ulcermedhunkumarm100% (1)
- Community and Public Health NursingDocument13 pagesCommunity and Public Health NursingEzekiel Bunda100% (1)
- Guided Reading Nursing RolesDocument3 pagesGuided Reading Nursing Rolestatiana quinteroNo ratings yet
- CQC LetterDocument2 pagesCQC Letterapi-273787280No ratings yet
- Ocde TurismoDocument19 pagesOcde TurismoPedro MentadoNo ratings yet
- Hospital Cash Claim FormDocument5 pagesHospital Cash Claim FormVivek UmbreNo ratings yet
- HELICHRYSUMDocument4 pagesHELICHRYSUMRaul Diaz100% (2)
- 10 Import Risk Analysis: 10.1 PurposeDocument5 pages10 Import Risk Analysis: 10.1 PurposeformaniteNo ratings yet
- Violence Against Women: A Global Public Health Crisis: Mary C. EllsbergDocument4 pagesViolence Against Women: A Global Public Health Crisis: Mary C. EllsbergEco IsaiahNo ratings yet
- CH 14 Part 2 Principles of Disease & Epidemiology (FA20)Document14 pagesCH 14 Part 2 Principles of Disease & Epidemiology (FA20)sammy alanNo ratings yet
- OFC06 - Employment Application FormDocument7 pagesOFC06 - Employment Application FormMustafa ÖzdamarNo ratings yet
- Sociology Syllabus 2018 2019Document61 pagesSociology Syllabus 2018 2019Akhil SethiNo ratings yet
- EKONSULTA FormDocument13 pagesEKONSULTA FormJirhana Lindagan Karon-KampangNo ratings yet
- Disability and Life Writing: Reports From The Nineteenth-Century AsylumDocument19 pagesDisability and Life Writing: Reports From The Nineteenth-Century AsylumHS22D001 MalavikaNo ratings yet
- Rosicrucian Art of Ancient HealingDocument16 pagesRosicrucian Art of Ancient HealingVictor Lopez100% (1)
- Abstracts For Grants YaleDocument58 pagesAbstracts For Grants YaleBliss Tamar LoladzeNo ratings yet
- Public Health Advocacy PDFDocument9 pagesPublic Health Advocacy PDFBrettnia Arado0% (1)
- English Test Unit 0 12th GradeDocument3 pagesEnglish Test Unit 0 12th GradeRoughie L. PalmaNo ratings yet
- Position Paper in Support of Senate Bill 2378Document5 pagesPosition Paper in Support of Senate Bill 2378Nikko SterlingNo ratings yet
- Who/Eip/Gpe/Cas/Icidh-2 Fi/ 01.1 Distr.: LimitedDocument218 pagesWho/Eip/Gpe/Cas/Icidh-2 Fi/ 01.1 Distr.: Limitedraunak0% (1)









































































































Download as pdf or txt
You might also like
- USL Step Up Women's Soccer StrategyDocument20 pagesUSL Step Up Women's Soccer StrategyUSL0% (1)
- 2022 USL Championship Record BookDocument57 pages2022 USL Championship Record BookUSL50% (2)
- 2021 SYL Player Experience PacketDocument8 pages2021 SYL Player Experience PacketUSL0% (2)
- Coaching Tiki Taka ContentsDocument5 pagesCoaching Tiki Taka ContentsJonty Toradmal0% (1)
- Textbook of Oral Medicine (Anil Govindrao Ghom, Savita Anil Ghom (Lodam) )Document1,141 pagesTextbook of Oral Medicine (Anil Govindrao Ghom, Savita Anil Ghom (Lodam) )Hritika Mehta100% (5)
- 2021 Championship Media GuideDocument73 pages2021 Championship Media GuideUSL100% (1)
- General and Oral Pathology For Dental Hygiene PracticeDocument361 pagesGeneral and Oral Pathology For Dental Hygiene Practicepsychposters100% (1)
- 2022 USL League One Media GuideDocument33 pages2022 USL League One Media GuideUSL0% (1)
- 2021 Championship Record BookDocument58 pages2021 Championship Record BookUSL100% (1)
- 2021 Return To Play Protocols - USL ChampionshipDocument62 pages2021 Return To Play Protocols - USL ChampionshipUSLNo ratings yet
- 2021 Return To Play Protocols - USL ChampionshipDocument62 pages2021 Return To Play Protocols - USL ChampionshipUSLNo ratings yet
- USL League One 2020 Record BookDocument35 pagesUSL League One 2020 Record BookUSL0% (1)
- Soccer Team Stats Tracker Pro V2.42Document1,493 pagesSoccer Team Stats Tracker Pro V2.42Gomv ConsNo ratings yet
- 2021 USL Academy League Operations ManualDocument57 pages2021 USL Academy League Operations ManualUSLNo ratings yet
- How Verheijen's Football Periodisation Inspired The Creation of SoccerPulse 1Document1 pageHow Verheijen's Football Periodisation Inspired The Creation of SoccerPulse 1Victor PetcuNo ratings yet
- Digital Video Games Approach A Designer For Invasion Games: @amyprice - 10Document6 pagesDigital Video Games Approach A Designer For Invasion Games: @amyprice - 10api-368878817No ratings yet
- USL League One 2021 Return To Play ProtocolsDocument63 pagesUSL League One 2021 Return To Play ProtocolsUSLNo ratings yet
- 2020 USL League One Media GuideDocument35 pages2020 USL League One Media GuideUSLNo ratings yet
- 2020 USL Championship Media GuideDocument41 pages2020 USL Championship Media GuideUSL33% (3)
- Alfredo Bonadeo - Montaigne and DeathDocument12 pagesAlfredo Bonadeo - Montaigne and DeathMark CohenNo ratings yet
- Lecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFDocument37 pagesLecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFstefany huangNo ratings yet
- Energy Cost and Metabolic Power in Elite Soccer A New Match Analysis ApproachDocument9 pagesEnergy Cost and Metabolic Power in Elite Soccer A New Match Analysis Approachjeduardo48No ratings yet
- Structuring A Program in Elite Professional Soccer: Strength and Conditioning Journal December 2017Document12 pagesStructuring A Program in Elite Professional Soccer: Strength and Conditioning Journal December 2017Jozef Oki SkumpijaNo ratings yet
- Tactical Periodisation in Football 1680883188Document2 pagesTactical Periodisation in Football 1680883188marcelloNo ratings yet
- A Methodology For The Analysis of Soccer Matches Based On PageRank Centrality PDFDocument16 pagesA Methodology For The Analysis of Soccer Matches Based On PageRank Centrality PDFOmar Enrique Garcia CaicedoNo ratings yet
- 12-Month Periodized Football Training ProgramDocument5 pages12-Month Periodized Football Training ProgramRon RNo ratings yet
- NOW IS THE TIME V 1 Compressed 1Document11 pagesNOW IS THE TIME V 1 Compressed 1harunabiaty849163No ratings yet
- Futsal Management Report PDFDocument37 pagesFutsal Management Report PDFJUNU CHAULAGAIN100% (1)
- The Business Model of European Football Club CompeDocument8 pagesThe Business Model of European Football Club CompeANSHUL MEHROTTRANo ratings yet
- gc101 PDFDocument45 pagesgc101 PDFFitim GabrricaNo ratings yet
- Implementing A Sustainable Club Membership Program at Goan Football PVT LTD (FC GoaDocument58 pagesImplementing A Sustainable Club Membership Program at Goan Football PVT LTD (FC GoaAli SaifyNo ratings yet
- Sport Plan User GuideDocument14 pagesSport Plan User Guidehamo pipaNo ratings yet
- Striker Manager Training (Modified)Document6 pagesStriker Manager Training (Modified)010b9No ratings yet
- Football Training and PracticesDocument8 pagesFootball Training and PracticesMichael Khunonyane100% (1)
- Football Movement and Application Assignment - Isaac BenouzekriDocument3 pagesFootball Movement and Application Assignment - Isaac BenouzekriIsaac BNo ratings yet
- 1115 Camp GuideDocument43 pages1115 Camp GuideEduardo FerranteNo ratings yet
- Wednesday Training Day Practices:: Speed EnduranceDocument7 pagesWednesday Training Day Practices:: Speed EnduranceMichael KhunonyaneNo ratings yet
- D License Log BookDocument16 pagesD License Log BookAayush SaxenaNo ratings yet
- LTAD Lead MagnetDocument38 pagesLTAD Lead Magnetsiphadube365No ratings yet
- Effects of A Contrast Training Program Without External Load On Vertical Jump, Kicking Speed, Sprint, and Agility of Young Soccer Players PDFDocument9 pagesEffects of A Contrast Training Program Without External Load On Vertical Jump, Kicking Speed, Sprint, and Agility of Young Soccer Players PDFNiña AlviaNo ratings yet
- Breakthrough BalanceDocument40 pagesBreakthrough BalanceBosko GuberinicNo ratings yet
- The FA's Longterm DevelopmentDocument6 pagesThe FA's Longterm DevelopmentBudi Handoko100% (1)
- Italian Serie A' Academy Training: An Inside Look at Two Italian Professional AcademiesDocument78 pagesItalian Serie A' Academy Training: An Inside Look at Two Italian Professional AcademiesJosé VelosaNo ratings yet
- Chelsea Football ClubDocument14 pagesChelsea Football ClubAnirudh MariaNo ratings yet
- Report 128083Document53 pagesReport 128083CueroNo ratings yet
- 1995 Joe Luxbacher - Soccer Practice Games-Human KineticsDocument164 pages1995 Joe Luxbacher - Soccer Practice Games-Human KineticsagusmulyaNo ratings yet
- Chapter 2: Decision Making: Case Application 2: Manchester City: Football Big Data Champions: Page 105 - 106Document6 pagesChapter 2: Decision Making: Case Application 2: Manchester City: Football Big Data Champions: Page 105 - 106Gautham100% (1)
- High-Intensity Interval Training: Loughborough University Institutional RepositoryDocument46 pagesHigh-Intensity Interval Training: Loughborough University Institutional RepositoryGytis GarbačiauskasNo ratings yet
- Lucozade Sport Pre Season Training Week 21Document1 pageLucozade Sport Pre Season Training Week 21Wan Ariff SallehNo ratings yet
- Exploratory Analysis FootballDocument6 pagesExploratory Analysis FootballMattNo ratings yet
- Journal 22Document32 pagesJournal 22nkosidlaminiNo ratings yet
- Soccer CoachDocument5 pagesSoccer Coachapi-286079185No ratings yet
- UEFA - A Licence Full DocumentDocument96 pagesUEFA - A Licence Full DocumentQUI SUIS-JE ?No ratings yet
- 08-12 SCI 09.34 Helena CostaDocument5 pages08-12 SCI 09.34 Helena CostaRicardo LuizNo ratings yet
- Soccer Psychology AssessmentDocument2 pagesSoccer Psychology AssessmentAurora NuñoNo ratings yet
- Injury Prevention Training in Football: Time To Consider Training Under Fatigue?Document4 pagesInjury Prevention Training in Football: Time To Consider Training Under Fatigue?aminNo ratings yet
- Special Olympics World Games Handball Technical ManualDocument32 pagesSpecial Olympics World Games Handball Technical ManualJenni SimcoeNo ratings yet
- Strength and Conditioining GAADocument8 pagesStrength and Conditioining GAADenis LordanNo ratings yet
- Best Foot Forward: Optimum PerformanceDocument6 pagesBest Foot Forward: Optimum PerformanceVicente Ignacio Ormazábal MedinaNo ratings yet
- Games Analysis Outdoor Team Sports by Using GPS SystemDocument35 pagesGames Analysis Outdoor Team Sports by Using GPS SystemAmin CherbitiNo ratings yet
- Receng Trends in High Intensity Aerobic - Training PDFDocument6 pagesReceng Trends in High Intensity Aerobic - Training PDFPablo100% (1)
- All About Masia 360Document7 pagesAll About Masia 360Pavol Gregora100% (1)
- Alvarado Lopez, Enoch - InterludeDocument14 pagesAlvarado Lopez, Enoch - InterludeDuvan RodeloNo ratings yet
- Youth Leagues Youth Development Review BookletDocument19 pagesYouth Leagues Youth Development Review BookletMarek Dragosz Keepers FoundationNo ratings yet
- A Guide To Developing Physical Qualities in Young AthletesDocument168 pagesA Guide To Developing Physical Qualities in Young AthletesjoaoaesfigueiredoNo ratings yet
- Preseden - Portofolio Soccer Training Centre PDFDocument147 pagesPreseden - Portofolio Soccer Training Centre PDFimam sodikunNo ratings yet
- Scottish Fa Uefa C Licence BrochureDocument5 pagesScottish Fa Uefa C Licence Brochuremohammad kamarNo ratings yet
- Manchester City FC, Annual Report 2014/15Document64 pagesManchester City FC, Annual Report 2014/15Tifoso Bilanciato100% (1)
- UEFA Equipment RegulationsDocument72 pagesUEFA Equipment RegulationsBasto WongNo ratings yet
- Fitness Testing in Football - Jens Bangsbo Magni MohrDocument144 pagesFitness Testing in Football - Jens Bangsbo Magni MohrSuman DevNo ratings yet
- Coaches Circle Issue 6 - May 2021Document24 pagesCoaches Circle Issue 6 - May 2021เซบาสเตียน ไลฟ์ลีดเดอร์No ratings yet
- Individual Defensive Skills Team DefenseDocument15 pagesIndividual Defensive Skills Team DefenseEl Cuervo Waterpolo100% (2)
- The high line: Debunking the myths surrounding the high press system used in footballFrom EverandThe high line: Debunking the myths surrounding the high press system used in footballNo ratings yet
- The Futsal Way: Maximising the Performance of Elite Football Teams Through Futsal MethodsFrom EverandThe Futsal Way: Maximising the Performance of Elite Football Teams Through Futsal MethodsNo ratings yet
- Book 4: Soccer Revelations Coaching Knowledge: Academy of Coaching Soccer Skills and Fitness DrillsFrom EverandBook 4: Soccer Revelations Coaching Knowledge: Academy of Coaching Soccer Skills and Fitness DrillsNo ratings yet
- Training Sessions For Soccer Coaches Volumes 1-2-3: Training Sessions For Soccer CoachesFrom EverandTraining Sessions For Soccer Coaches Volumes 1-2-3: Training Sessions For Soccer CoachesNo ratings yet
- Training Sessions For Soccer Coaches Volume 2: Training Sessions For Soccer Coaches, #2From EverandTraining Sessions For Soccer Coaches Volume 2: Training Sessions For Soccer Coaches, #2No ratings yet
- 2022 Mid Year MeetingDocument1 page2022 Mid Year MeetingUSLNo ratings yet
- 2022 Mid Year MeetingDocument1 page2022 Mid Year MeetingUSLNo ratings yet
- 2022 USL Academy Cup Operations ManualDocument30 pages2022 USL Academy Cup Operations ManualUSLNo ratings yet
- 2022 Mid-Year Meeting - ScheduleDocument1 page2022 Mid-Year Meeting - ScheduleUSLNo ratings yet
- 2018 SYL Player PacketDocument7 pages2018 SYL Player PacketUSLNo ratings yet
- 2021 USL League One Media GuideDocument35 pages2021 USL League One Media GuideUSLNo ratings yet
- USL Championship Return To Play ProtocolsDocument53 pagesUSL Championship Return To Play ProtocolsUSLNo ratings yet
- 2019 USL Championship Media GuideDocument42 pages2019 USL Championship Media GuideUSL100% (1)
- 2018 SYL Player PacketDocument7 pages2018 SYL Player PacketUSLNo ratings yet
- USL 2018 Media GuideDocument45 pagesUSL 2018 Media GuideUSL100% (2)
- USL 2018 Media GuideDocument45 pagesUSL 2018 Media GuideUSL100% (2)
- Muhamad Lutfi ParatuberculosisJournalDocument17 pagesMuhamad Lutfi ParatuberculosisJournalLutfi AlkaNo ratings yet
- The Classification of SicknessDocument361 pagesThe Classification of SicknessizamNo ratings yet
- Sicknessandfitnesscertificates PDFDocument6 pagesSicknessandfitnesscertificates PDFniraj_sdNo ratings yet
- Transcranial Magnetic Stimulation - Jasper AzzarelloDocument2 pagesTranscranial Magnetic Stimulation - Jasper AzzarelloJasper AZZARELLONo ratings yet
- Ethiopia: Feed The Future Innovation Lab For Livestock SystemsDocument11 pagesEthiopia: Feed The Future Innovation Lab For Livestock SystemsMitikuNo ratings yet
- FNCP Alfonso CaviteDocument8 pagesFNCP Alfonso Caviteroxjanmer_13No ratings yet
- Approach To Foot UlcerDocument29 pagesApproach To Foot Ulcermedhunkumarm100% (1)
- Community and Public Health NursingDocument13 pagesCommunity and Public Health NursingEzekiel Bunda100% (1)
- Guided Reading Nursing RolesDocument3 pagesGuided Reading Nursing Rolestatiana quinteroNo ratings yet
- CQC LetterDocument2 pagesCQC Letterapi-273787280No ratings yet
- Ocde TurismoDocument19 pagesOcde TurismoPedro MentadoNo ratings yet
- Hospital Cash Claim FormDocument5 pagesHospital Cash Claim FormVivek UmbreNo ratings yet
- HELICHRYSUMDocument4 pagesHELICHRYSUMRaul Diaz100% (2)
- 10 Import Risk Analysis: 10.1 PurposeDocument5 pages10 Import Risk Analysis: 10.1 PurposeformaniteNo ratings yet
- Violence Against Women: A Global Public Health Crisis: Mary C. EllsbergDocument4 pagesViolence Against Women: A Global Public Health Crisis: Mary C. EllsbergEco IsaiahNo ratings yet
- CH 14 Part 2 Principles of Disease & Epidemiology (FA20)Document14 pagesCH 14 Part 2 Principles of Disease & Epidemiology (FA20)sammy alanNo ratings yet
- OFC06 - Employment Application FormDocument7 pagesOFC06 - Employment Application FormMustafa ÖzdamarNo ratings yet
- Sociology Syllabus 2018 2019Document61 pagesSociology Syllabus 2018 2019Akhil SethiNo ratings yet
- EKONSULTA FormDocument13 pagesEKONSULTA FormJirhana Lindagan Karon-KampangNo ratings yet
- Disability and Life Writing: Reports From The Nineteenth-Century AsylumDocument19 pagesDisability and Life Writing: Reports From The Nineteenth-Century AsylumHS22D001 MalavikaNo ratings yet
- Rosicrucian Art of Ancient HealingDocument16 pagesRosicrucian Art of Ancient HealingVictor Lopez100% (1)
- Abstracts For Grants YaleDocument58 pagesAbstracts For Grants YaleBliss Tamar LoladzeNo ratings yet
- Public Health Advocacy PDFDocument9 pagesPublic Health Advocacy PDFBrettnia Arado0% (1)
- English Test Unit 0 12th GradeDocument3 pagesEnglish Test Unit 0 12th GradeRoughie L. PalmaNo ratings yet
- Position Paper in Support of Senate Bill 2378Document5 pagesPosition Paper in Support of Senate Bill 2378Nikko SterlingNo ratings yet
- Who/Eip/Gpe/Cas/Icidh-2 Fi/ 01.1 Distr.: LimitedDocument218 pagesWho/Eip/Gpe/Cas/Icidh-2 Fi/ 01.1 Distr.: Limitedraunak0% (1)